INTRODUCTION
Lumbar disc herniation (LDH) is a common disease, but its occurrence, diagnosis, and clinical outcomes after conservative treatment with medication have been poorly documented. Prevention and initial management of LDH in the primary health care unit is important in order to prevent further deterioration.
Numerous studies have explored causative factors of primary LDH. One factor is pathology that increases lumbar segment motion, such as general joint laxity (GJL).1,2,3,4) However, the role of GJL in the development of LDH is unclear. To date, GJL has been evaluated as a potential causative factor of chronic joint pain,5,6,7,8,9) and recent studies have suggested associations between GJL and spine-related disorders such as lower back pain, accelerated disc degeneration, and disc recurrence following discectomy for primary LDH.1,2,4,5,6,8,10,11,12,13) Considering previous articles, GJL might be a causative factor of primary LDH,13) but this possibility has not been adequately studied. In addition, the impact of GJL on clinical outcomes after conservative treatment for LDH has not been investigated to our knowledge.
Therefore, we aimed to evaluate the relationship between GJL and LDH occurrence and compare clinical outcomes after conservative treatment with medication in LDH patients with and without GJL. We hypothesized that GJL is a causative factor for LDH occurrence and affects the outcomes of conservative treatment.
METHODS
1. Participants
We obtained approval from the institutional review board of corresponding author's hospital for this study (AFMC-10-125). This was a retrospective study from prospectively collected data from an Armed Forces hospital in Korea that investigated the impact of GJL on young male patients with and without LDH. From the prospectively collected data, patients who were recruited in 2011 and fully complied with inclusion and exclusion criteria were enrolled in the current study. We reviewed demographic data and clinical outcomes after conservative treatment in patients with LDH regardless of the presence of GJL.
LDH was diagnosed by magnetic resonance images (MRI) of the lumbar spine that corresponded with definite symptoms or signs of an LDH lesion. All enrolled LDH patients underwent the same conservative treatment for at least 3 months, which included non-steroidal anti-inflammatory drugs, gabapentin, and physical therapy. Successful improvement after conservative treatment was defined as >50% improvement in pre-treatment pain intensity following treatment and maintenance of this improvement for one month or longer.
This study only included patients who met the following inclusion criteria: (1) diagnosis of LDH, based on lumbar spine MRI, that corresponded to the clinical manifestation and physical examination; (2) male sex; (3) between 20 and 30 years of age; (4) volunteered for this study with written informed consent; and (5) followed up for at least 2 years. We excluded patients who met any of the following criteria: (1) fractures, infection, or tumors of the lumbar spine; (2) trauma history of the lumbar spine; (3) female sex; (4) an allergic or problematic history with the applicable medications; (5) a follow-up period of less than 2 years; and (6) inability to accurately fill out the questionnaires during regular follow-up times due to medical problems such as stroke or dementia. These inclusion and exclusion criteria were used to avoid any potential confounding effects. Informed consent was obtained from all patients.
2. Subjects
As described above, this study was conducted with fully compliant subjects from a large group of patients (1,382 patients) to investigate the relationship between GJL and spine-related disorders. The study included 128 males who met our inclusion and exclusion criteria and who presented at the Armed Forces hospital from January 2011 to December 2011. The control group included 276 males who were matched for age and body mass index (BMI) with the study group during the same reference period as the large group of recruited patients. Potential participants were informed that their decision to participate was voluntary and that refusal to participate would not affect their treatment.
3. Outcome Measures
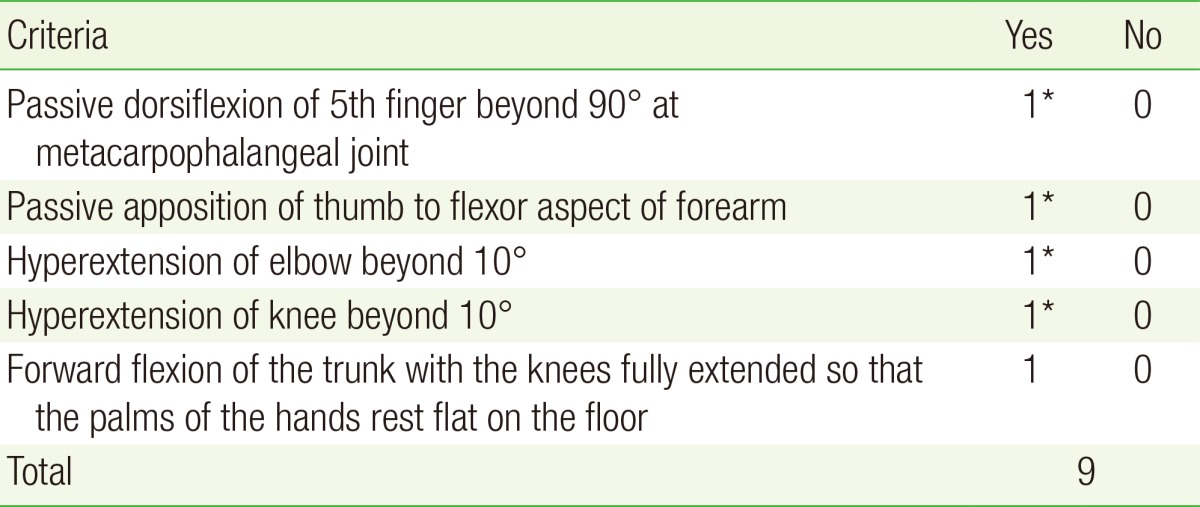
The primary outcome measure was the presence or absence of GJL. The Beighton scale was used to determine whether GJL was present, and the range of joint motion was assessed with a standard clinical set of goniometers (Table 1). A threshold cutoff value of 4 of 9 total points was used to determine the presence of GJL, as in a previous study.13,14) The evaluation of GJL was analyzed by one research coordinator who was not otherwise involved in this study.
The secondary outcome measure was the clinical outcome, which was evaluated with the visual analog scale (VAS) for pain and the Oswestry disability index (ODI). Scores were obtained before treatment and again at 1 month, 3 months, 6 months, 1 year, and 2 years after treatment. The VAS score for pain was evaluated separately for the lower back and the lower extremities. Patients were instructed to make a mark on a horizontally oriented, 10-point VAS labeled 'no pain' (0 point) at the far left and 'greatest pain' (10 point) at the far right. The ODI (version 2) is a self-reported questionnaire measuring back-specific function including pain intensity, personal care, lifting, walking, sitting, standing, sleeping, sex life, social life, and traveling. The questionnaire consists of 10 items each with 6 response levels. Each item is scored from 0 to 5, and the total score is converted to a 0 to 100 scale.15) Questionnaires, chart data, and clinical records were also analyzed by one research coordinator who was not otherwise involved in this study. Patients were not allowed to review their previous scores.
4. Statistical Analysis
To compare the differences between the LDH patients with and without GJL, we used an independent Student t-test for continuous variables that were normally distributed. We used chi-square test and Fisher's exact test for categorical variables. We used the Spearman correlation to assess the relationships between primary LDH and variables such as gender, age, height, weight, BMI, hypertension, diabetes, smoking history, and GJL. Multivariate logistic regression analysis was then conducted for variables that showed a significant correlation with primary LDH occurrence, and we also determined the odds ratio. SAS ver. 9.1.3 (SAS Institute Inc., Cary, NC, USA) was used for all analyses, and two-tailed P-values<0.05 were considered statistically significant.
RESULTS
1. Demographic Data
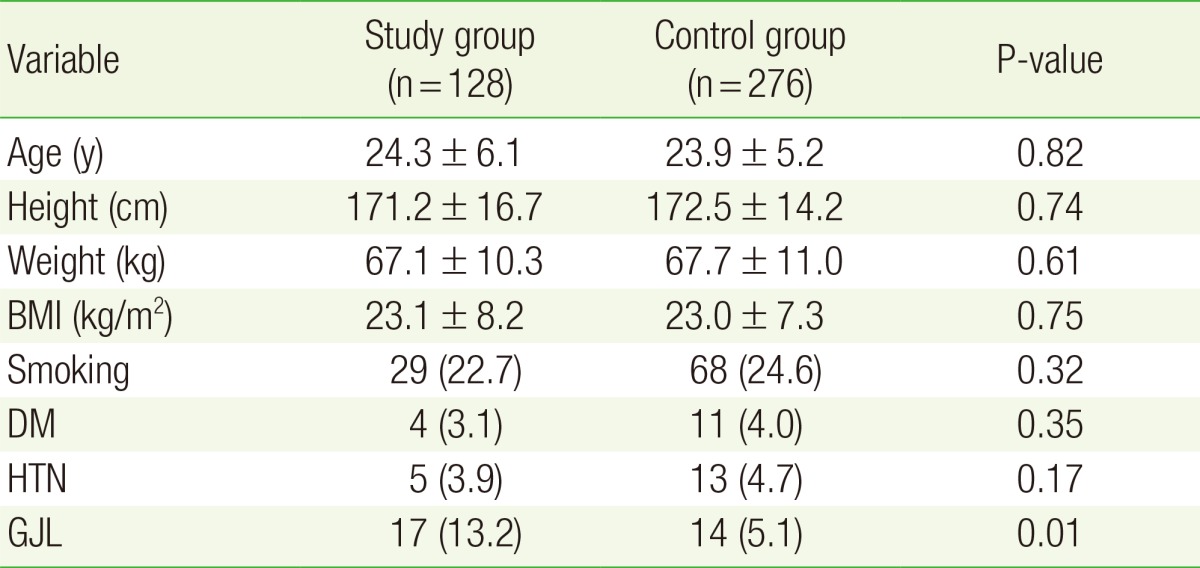
We retrospectively reviewed 128 patients in the study group and 276 patients in the control group, and none were lost to follow-up. Demographic variables, such as age and smoking history, did not differ significantly between the groups (Table 2).
2. Prevalence of General Joint Laxity and Factors Affecting Lumbar Disc Herniation
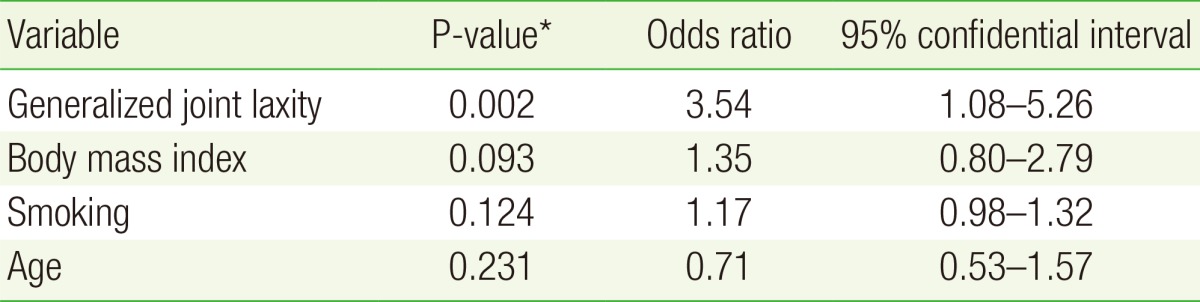
The prevalence of GJL was significantly higher in the study group (17/128 patients, 13.2%) than in the study group (14/276 patients, 5.1%; P=0.01) (Table 2). In correlation analysis using the Spearman method, weight (r=0.162, P=0.03), BMI (r=0.131, P=0.03), and GJL (r=0.372, P<0.01) were significantly correlated with primary LDH occurrence. In logistic regression analysis, only GJL (P=0.002) was associated with the occurrence of LDH as an independent causative factor (Table 3), and the odds ratio for LDH and the occurrence of GJL was 3.54 (95% confidence interval, 1.08 to 5.26).
3. Clinical Outcomes
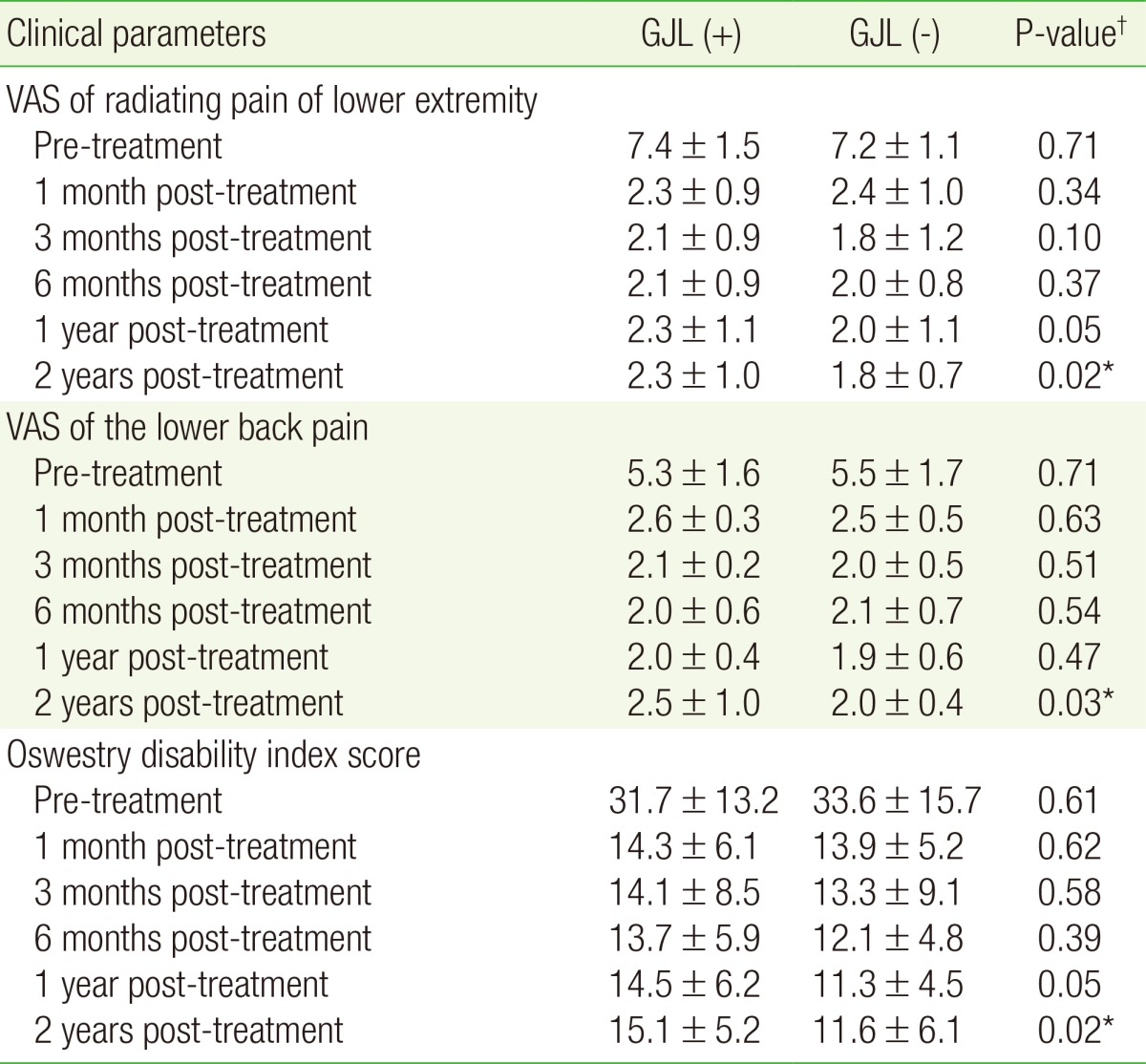
Clinical outcomes are summarized in Table 4. All LDH patients at the final follow-up had improved significantly compared to baseline (P<0.01); however, the VAS and ODI scores at the final follow-up were worse in patients with GJL compared to those in patients without GJL. The presence of GJL in LDH patients was associated with worse clinical outcomes in terms of VAS scores lower extremity pain (P=0.02), lower back pain (P=0.03), and the ODI score (P=0.03).
DISCUSSION
Conditions that increase lumbar segment motion include rheumatic disorders, Ehlers-Danlos syndrome, Marfan syndrome, and benign joint hypermobility syndrome,8,10,12,13) of which GJL is the most familiar and common disease entity. GJL was considered an asymptomatic disorder in the past; however, it has recently been shown that GJL is often associated with specific disorders and clinical manifestations. Several clinicians have investigated GJL due to its relationship to diseases such as acute anterior shoulder dislocation and ligament injury.5,15,16,17) Likewise, GJL may be a causative factor for LDH.13) Previous studies have determined that lower back pain, accelerated disc degeneration, and the recurrence of disc herniation following discectomy for primary LDH are closely related to the presence of GJL at baseline.2,9,11,18) In this respect, GJL may also be a predictor for primary LDH, but previous studies have not fully documented whether GJL is related to the occurrence of primary LDH, and the relationship between GJL and the clinical outcomes after conservative treatment for LDH is still controversial. Thus, we aimed to address these questions in the current study.
As described above, increasing lumbar segment motion is related to lower back pain and accelerated disc degeneration of the lumbar spine.1,2,4,6,10,13,18) Given the close relationship between recurrent LDH and segmental hypermobility, a disease entity affecting lumbar segment motion might cause LDH; however, this possibility has not been thoroughly assessed. The results of the current study suggest that GJL might be associated with LDH occurrence; the prevalence of GJL was significantly higher in the study group (13.2%; 17/128) than in the control group (5.1%; 14/276). Spearman correlation analysis revealed that weight (r=0.162, P=0.03), BMI (r=0.131, P=0.03), and GJL (r=0.372, P<0.01) were significantly correlated with primary LDH occurrence. In multivariate logistic regression analysis, GJL was the only significant predictor of LDH. The clinical outcomes of conservative treatment for LDH patients with and without GJL (group A and group B, respectively) revealed that GJL might aggravate the efficacy of conservative treatment, which may also explain the differences between pre-treatment and 2 years post-treatment in both groups: VAS scores for radiating pain were 5.1±0.8 in group A and 5.5±0.6 in group B; VAS scores for lower back pain were 2.8±0.6 in group A and 3.5±0.4 in group B; and ODI scores were 16.6±6.3 in group A and 22±5.7 in group B. Based on the outcomes, GJL may not improve despite proper conservative treatments with medication and physical treatment for LDH. In addition, the presence of GJL at baseline may be associated with LDH occurrence.
This study has several limitations. First, it was retrospectively designed with a relatively small sample size (404 patients) and a short follow-up (2 years). To better establish the impact of GJL on the occurrence of LDH and the treatment outcomes, further studies should use a prospective randomized controlled design and follow a larger number of patients over an extended time. Second, we only included young males in this study. The prevalence of GJL decreases with age and is sex-dependent (3 times more common in female patients than male patients),12,13,19) and the Beighton scale as a diagnostic criteria for GJL differs by sex.1,8,13) For these reasons, we limited our study to young males in order to minimize confounding effects. However, including only males can complicate statistical analysis due to the inherent non-normal distribution, and our results might not apply to all populations. Third, we did not consider other possible factors that influence LDH occurrence, including socioeconomic status, alcohol history, and appointment in the army. Finally, we used a score of 4 points or more on the Beighton scale to diagnose GJL. Although a diagnostic gold standard for GJL has not been established, previous studies have demonstrated that the Beighton scale with a cutoff value of 4 points showed a greater diagnostic accuracy with higher sensitivity, specificity, and reliability than other diagnostic modalities and their cut-off values.1,13,14,19)
Despite these limitations, the current study has a number of strengths. First, this study occurred at an Armed Forces Hospital, so all enrolled patients participated in regular follow-up visits. Performing the study at an Armed Forces Hospital also ensured that the study population was homogenous with respect to sports and physical activity.13) Such homogeneity reduced the risk that the outcomes were influenced by confounding factors. Finally, this is an unique study to evaluate the impact of GJL on LDH occurrence and clinical outcomes after conservative treatment. Given the lack of information on the relationship between GJL and LDH, our results lay the foundation for further research.
In conclusion, this study assessed whether GJL is a causative factor for LDH and a negative prognostic factor for clinical improvement after conservative treatment for LDH. We demonstrated that GJL may be related to LDH occurrence and may be a potential factor in its occurrence. In addition, GJL in LDH patients may be associated with a worse clinical outcome after conservative treatment compared to LDH patients without GJL. Consequently, GJL should be evaluated initially in patients with LDH, and this information should be communicated to patients. Additional studies should be performed with a larger sample size, an extended follow-up period, and a prospective randomized design in order to better understand the relationship between GJL and LDH and the impact of GJL on treatment outcomes.