INTRODUCTION
As the obese population increases, the incidence of metabolic syndrome is also increasing. There has been a recent report1-4) on the relationship between the diagnostic criteria of metabolic syndrome or changes in the pulmonary function and cardiovascular mortality and total mortality. As such, there is increasing interest in changes in metabolic syndrome associated with changes in pulmonary function.
In a number of recent studies, it was reported that among the changes in pulmonary function, pulmonary function, deterioration is related to hypertension, type 2 diabetes, low-density lipoprotein cholesterol, overall obesity, abdominal obesity and insulin resistance.5-9) Among the above listed factors, hypertension, diabetes, and abdominal obesity are included as diagnostic criteria for metabolic syndrome, hence it can be inferred that identifying the relationship between metabolic syndrome and pulmonary function deterioration is meaningful.
In a study on the relationship between pulmonary function deterioration and metabolic syndrome, pulmonary function deterioration was detected where there is metabolic syndrome. Even when gender, age, smoking status, alcohol drinking and physical activity factors were reflected, limited pulmonary function deterioration showed independent relevance to increased risk of metabolic syndrome.8)
Obese people have shown signs of pulmonary function deterioration,8-9) hence, a simple pulmonary function test during health examination can be used as a predictive factor for metabolic syndrome in obese people.
As such, this study will look into the relationship based on the changes in metabolic syndrome diagnostic criteria and pulmonary function indices, like forced expiratory volume for 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio.
METHODS
1. Subjects
This study targeted those who underwent a health examination at the Eulji General Hospital Health Center between January 2, 2008 and August 13, 2008. The age of the subjects ranged from over 20 to under 70 years old, and included 1,370 people out of the total 1,566 patients. The subjects who reported a clinical history on cardiovascular disease (myocardial infarct, angina pectoris) and pulmonary disease (asthma, chronic obstructive pulmonary disease) or cancer, were excluded based on their survey answers. Those with no pulmonary function test results or body measurements (waist circumference, height) were also excluded.
2. Measurements
1) Survey
Prior to conducting the general health examination, patients' consent was attained to conduct a survey. The patients were asked to record specifically their past clinical history, the types of drugs they are taking, their alcohol and smoking history, and physical activity level, etc. Those who found it difficult to fill out the survey were assisted by nurses.
As for physical activity level, subjects were classified into 1) light activity: walking for less than 2 hours a day, working in an office, or working as a housewife with little household chores, 2) medium level activity: walking for 2-4 hours a day, working in manufacturing or service industry, or working as a housewife with a lot of household chores, 3) hard activity: working in agriculture, fishery, civil engineering or construction industry, 4) severe activity: athletes, or those who transport wood or engage in farming work during farming season.
2) Physical measurement
Waist circumference was measured from the center point of the last rib and iliac spine. Height and weight were measured while wearing light clothing (health examination gown). For obesity level, body mass index (BMI) was used, which is the value attained by dividing the body weight (kg) against the height (m2), to classify the subjects into obese (BMI Ōēź 25 kg/m2), overweight (23 kg/m2 Ōēż BMI < 25 kg/m2) and normal weight (BMI < 23 kg/m2) groups. With the blood test, triglyceride, high-density lipoprotein cholesterol (HDL-C), and fasting blood sugar were measured. Blood pressure was measured using an automatic sphygmomanometer after taking over 5 minutes of rest.
3) Pulmonary function test
Pulmonary function was measured between 8 AM and 12 PM using a spirometer (model 2130; SensorMedics Co., Yorba Linda, CA, USA). Subject was in a seated position, and the measurement was taken by an experienced nurse. To reduce any variance in measurement by the person taking the measurement the same nurse measured everyone. The values measured were FEV1, FVC, FEV1/FVC.
3. Definition of Metabolic Syndrome
Metabolic syndrome, based on the Asia criteria of the American Heart Association/National Heart, Lung, and Blood Institute,10) is diagnosed when 3 out of the following 5 categories are satisfied: 1) blood pressure of systolic blood pressure Ōēź 130 mm Hg or diastolic blood pressure Ōēź 85 mm Hg, or is taking a hypertension drug, 2) fasting blood sugar Ōēź 100 mg/dL, or is taking a diabetes drug, 3) triglyceride Ōēź 150 mg/dL, or is taking a dyslipidemia drug, 4) low HDL-C (male < 40 mg/dL, female < 50 mg/dL), or is taking a dyslipidemia drug, or 5) the waist circumference applied is male Ōēź 90 cm, female Ōēź 80 cm. Also, female waist circumference of over 85 cm was also applied based on the Korean Society for the Study of Obesity.11)
4. Statistical Analysis
The data was shown as mean ┬▒ standard deviation. For the difference in variables among the groups, Student t-test and Žć2-test were used. For the relationship between each of the metabolic syndrome factors and pulmonary function, Pierson partial correlation coefficient was used, having modified the age and height factors. For the existence of metabolic syndrome and the relationship with pulmonary function, analysis of covariance was used by controlling the physical activity level and smoking level. This data was analyzed by using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
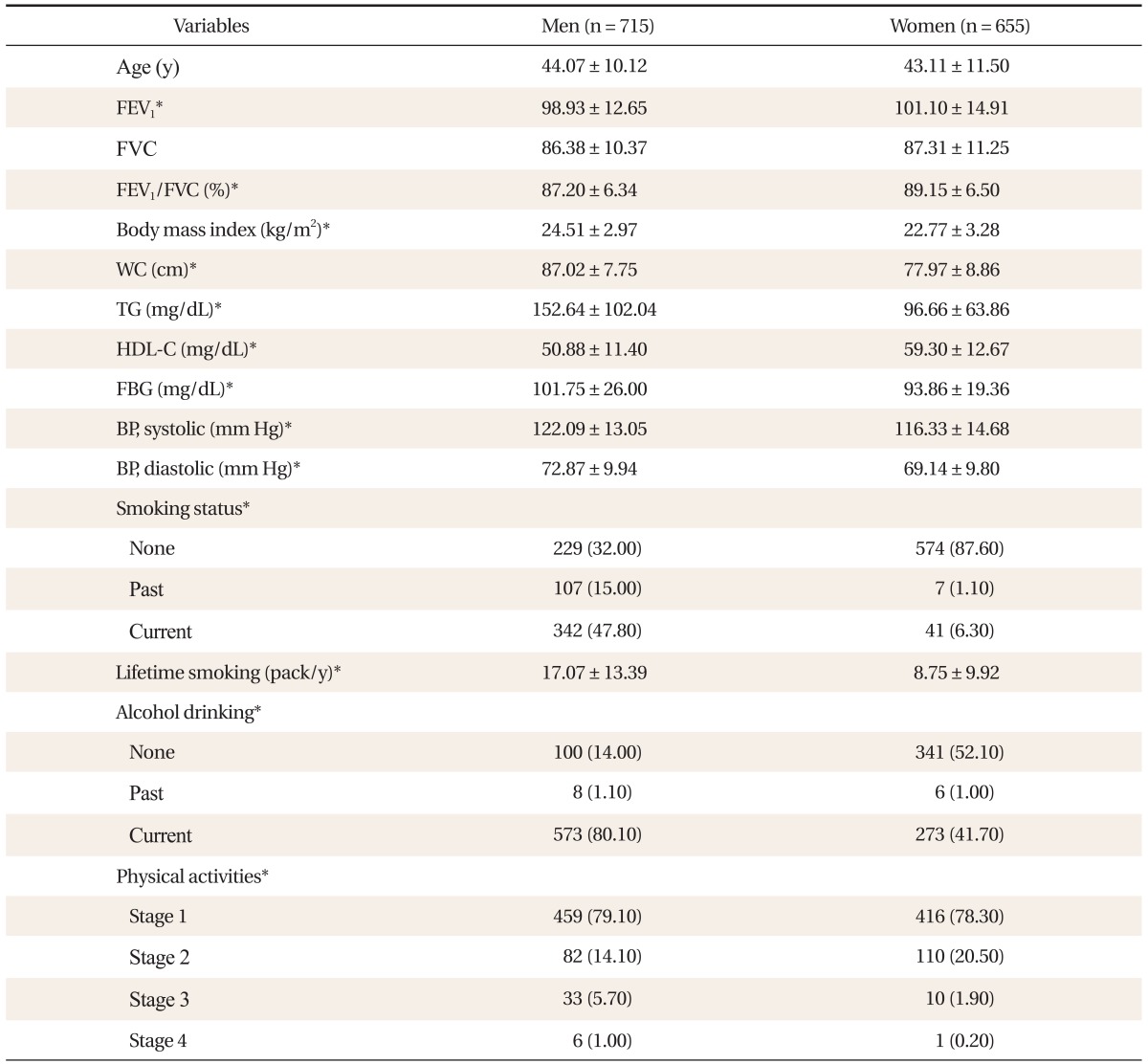
1. General Characteristics
Average age of men and women was 44.07 ┬▒ 10.12 years old (male) and 43.11 ┬▒ 11.50 years old (female), respectively. Pulmonary function figures were higher in women than men. As for BMI, men's average was 24.51 ┬▒ 2.97 kg/m2 and women's average was 22.77 ┬▒ 3.28 kg/m2. The ratio of obese people (BMI Ōēź 25 kg/m2) was 42.9% and 23.7%, respectively, for men and women. The distribution of metabolic syndrome was statistically higher for men than women at 25.5% versus 17.3%. Women had lower triglyceride and fasting blood sugar levels than men, but HDL-C was statistically higher. In men, systolic blood pressure was 122.09 ┬▒ 13.05 mm Hg and diastolic blood pressure was 72.87 ┬▒ 9.94 mm Hg, which is statistically higher than women's systolic blood pressure of 116.33 ┬▒ 14.68 mm Hg and diastolic blood pressure of 69.14 ┬▒ 9.80 mm Hg.
As for the smoking ratio, current smoker ratio stands at 47.8% for men and 6.3% for women, showing a higher smoking rate in men with higher total smoking volume (Table 1).
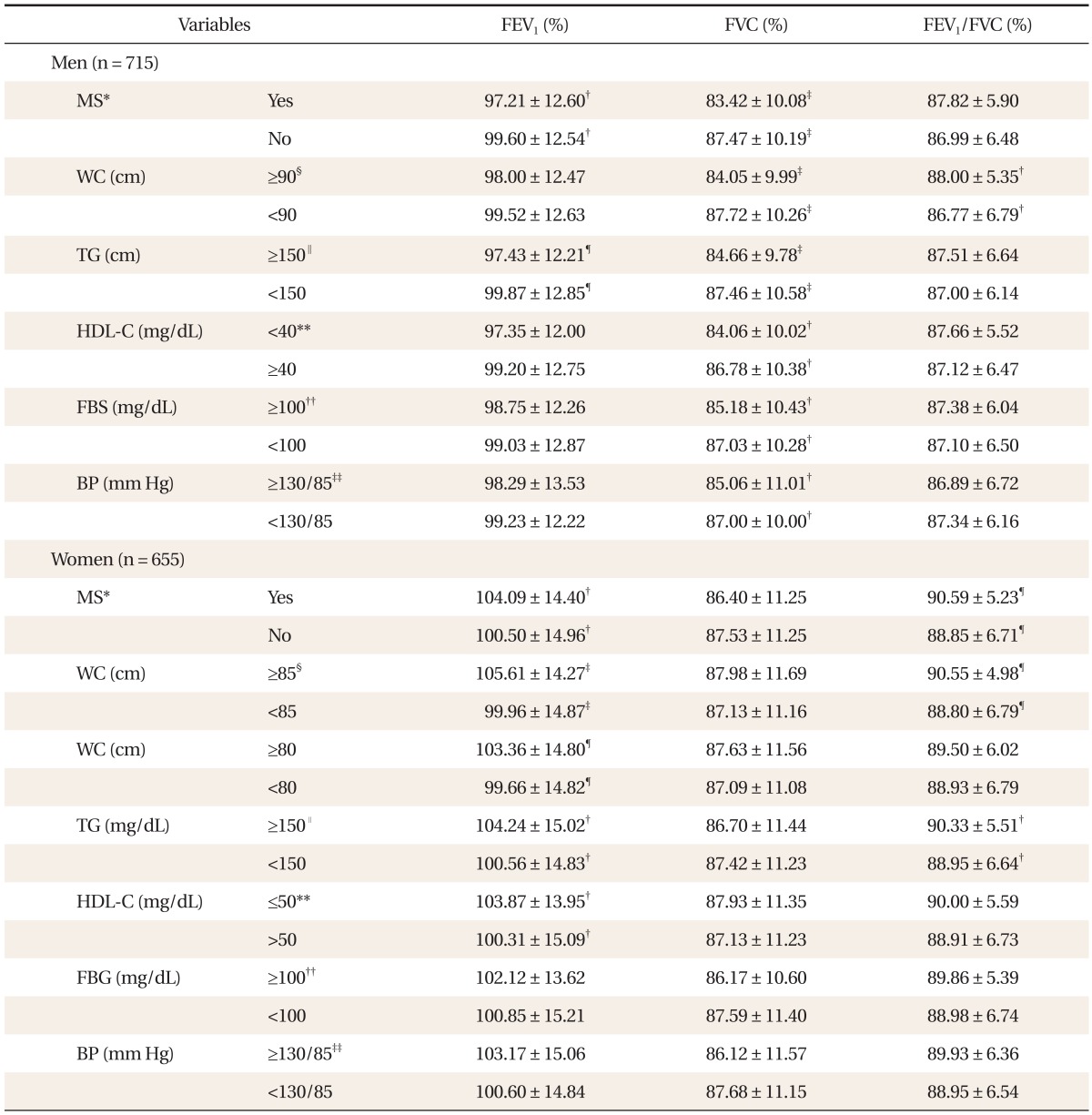
2. Relationship between Diagnostic Criteria for Metabolic Syndrome and Pulmonary Function
Among males, there were big differences in FVC according to whether or not he had metabolic syndrome. In fact, the FVC difference was 83.42 ┬▒ 10.08%, 87.47 ┬▒ 10.19% (P < 0.001). In addition, people with waist circumference of 90 cm or above had FVC of 84.05 ┬▒ 9.99%, while for those with waist circumference below 90 cm it was 87.72 ┬▒ 10.26% (P < 0.001). Moreover, FVC of people with above 150 mg/dL of triglyceride was 84.66 ┬▒ 9.78% while it was 87.46 ┬▒ 10.58% (P < 0.001) for those with triglyceride of below 150 mg/dL. In particular, waist circumference and triglyceride showed the most significant difference of P < 0.001. On the other hand, FEV1 was 97.43 ┬▒ 12.21% for triglyceride levels above 150 mg/dL, while below 150 mg/dL, FEV1 recorded was 99.87 ┬▒ 12.85% (P < 0.01). As such, the difference was only evident between metabolic syndrome and triglyceride level. The FEV1/FVC ratio difference was found to be correlated only to waist circumference. Among females, FVC didn't show any significant difference in any of these items. FEV1 showed a difference according to whether or not she had metabolic syndrome and waist circumference of 85 cm and 80 cm, respectively, and whether the HDL-C level was high or low. However, there was no correlation found between FEV1 and pulmonary function. The FEV1/FVC ratio difference was found among those females with waist circumference of 85 cm or above and whether or not she had triglyceride and metabolic syndrome (Table 2).
In order to identify correlation between metabolic syndrome and pulmonary function, we have controlled the level of smoking and degree of physical activity, which all have influence on pulmonary function. When smoking and degree of physical activity were controlled, males showed significant correlation between metabolic syndrome and FVC, while females showed significant correlation between metabolic syndrome and FEV1/FVC (No table was provided).
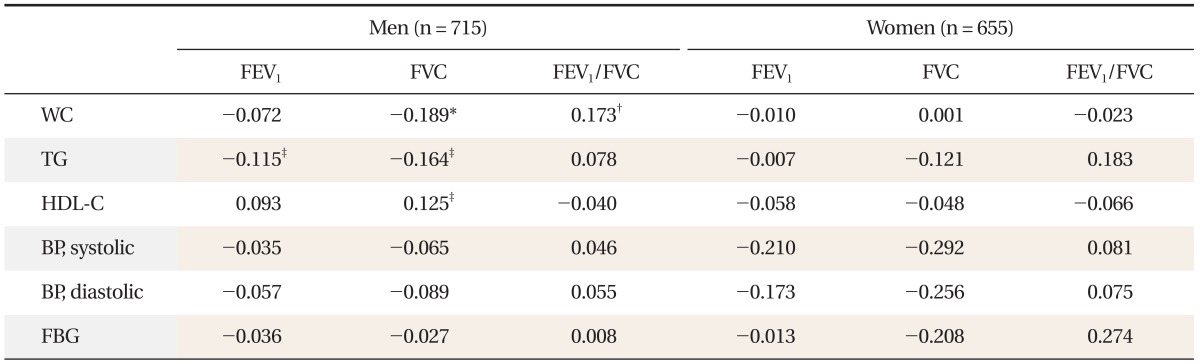
3. Correlation between Diagnostic Criteria for Metabolic Syndrome and Pulmonary Function
When age, height as well as total smoking amount were factored in, FVC showed significant negative correlation with waist circumference & triglyceride levels among males, while it showed positive correlation with HDL-C. In particular, waist circumference with a value of P < 0.001 showed a high level of negative correlation. FEV1 showed negative correlation with triglyceride levels, while FEV1/FVC ratio showed positive correlation with waist circumference. Meanwhile, females showed no correlation with pulmonary function measurement value as well as metabolic syndrome component (Table 3).
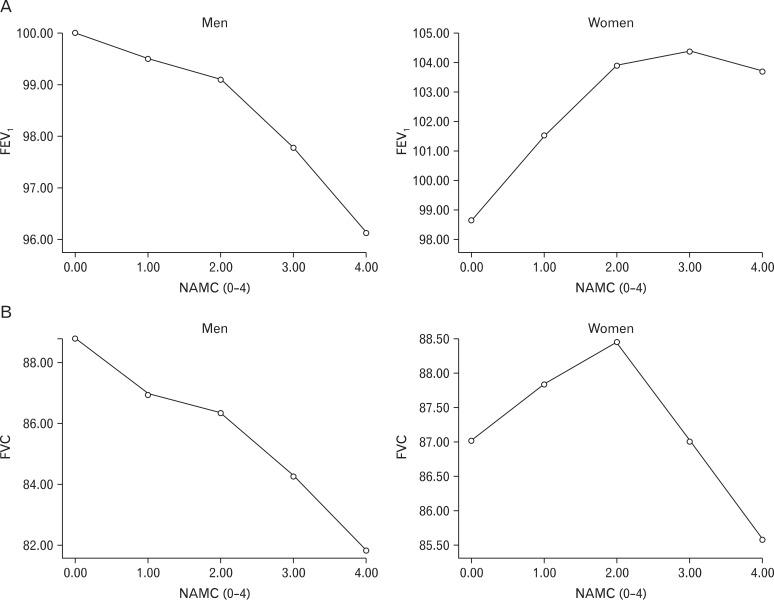
4. The Relationship between Number of Components That Serve as the Criteria for Diagnosing Metabolic Syndrome and Pulmonary Function
Pulmonary function changed according to the degree of severity of metabolic syndrome. In the case of males, FVC declined as severity of metabolic syndrome increased, while there was no correlative relationship found among females (Figure 1).
DISCUSSION
This study aimed to find relevance between components that serve as the criteria for diagnosing metabolic syndrome and poor performing pulmonary function. Among males, every diagnostic component of metabolic syndrome had significant correlation with poor pulmonary function. On the other hand, among females, FVC had a tendency of poor pulmonary function but with no significant relevance.
Many studies conclude that pulmonary function drops among obese people.12,13) Previously, studies have used BMI, waist circumference, waist/hip circumference ratio, abdominal thickness (height) and skin thickness test as the markers that show obesity.14-16) However, as of recent, studies focus on abdominal obesity as indicative of overall level of obesity. As such, this study tried to examine the waist circumference that demonstrates abdominal obesity as well as the relationship between metabolic syndrome components that are easily found among obese people and effects these factors have on pulmonary function.
According to the study, reverse-correlation was found between diagnostic components of metabolic syndrome and pulmonary function. Among males, while there were significant differences in FVC according to whether or not there were any diagnostics components for metabolic syndrome, there were no FVC differences found among females. However, for both males and females, pulmonary function differed significantly according to waist circumference. For males, there was a significant statistical difference in FVC and FEV1/FVC. In the case of females, for waist circumference of 85 cm, both FEV1 and FEV1/FVC had a significant statistical difference, while waist circumference of 80 cm only showed a significant statistical difference in FEV1. In particular, among males, the partial correlation coefficient of waist circumference was FVC -0.189, FEV1/FVC 0.173.
According to a study conducted by Leone et al.,17) both males and females showed reverse-correlation between all diagnostic components of metabolic syndrome and pulmonary function. As in this study, abdominal obesity was reported as the most powerful predictor of poor pulmonary function.17) In addition, Chen et al.18) found out that both males and females showed negative correlation between FEV1/FVC and waist circumference even after age, height, weight, workload, energy consumption, and smoking were factored in. Thus, the bigger the waist circumference becomes, the greater its impact on pulmonary function, eventually having partial impact on the movements of diaphragm and chest.18) Canoy et al.16) took the waist/hip circumference ratio as the indicator of abdominal obesity to verify that both FEV1 and FVC show reverse correlation both among males and females.
In Australia, Lazarus et al.14) showed that FVC has negative correlation with males' waist circumference and that no relationship was found among females.14) Moreover, according to a study conducted by Ochs-Balcom et al.,19) males' FEV1 and FVC showed negative correlation in all obesity markers (weight and level of obesity) as well as markers for abdominal obesity (waist circumference, ratio of waist/hip circumference, abdominal height). However, among females, only the abdominal height and waist circumference showed negative correlation with FEV1, while all markers of obesity showed negative correlation with FVC. In particular, the reverse relationship between FEV1 and abdominal height was evident only among those obese people with BMI of over 25 kg/m2.19)
According to this study, in men, correlation between waist circumference and FVC, FEV1/FVC ratio was statistically significant in terms of partial correlation coefficient where age, height and total smoking amount was reflected. For women, the correlation was not statistically significant across all respiratory indexes. The results were similar to the research conducted by Harik-Khan et al.,20) which showed that FVC and FEV1 and waist circumference and hip circumference had negative correlation for men, whereas for women, only FVC had correlation and FEV1 showed no correlation. To explain such differences by gender, it could be assumed that fat distribution could affect diaphragm and thoracic movements of women more than men and that waist circumference and hip circumference ratio does not affect pulmonary function.20)
Carey et al.21) said that changes in weight and obesity are related to FEV1 and in particular, weight increase of the group with the highest obesity level showed greater FEV1 reduction. Such results demonstrated a wider gap in men because male abdominal fat accumulated relatively more during the 7-year research period and in women, hip circumference tended to increase more. Thus, their increase in waist/hip circumference ratio was lower than men. Results of this study were also different by sex since males showed a higher level of obesity than women, with a higher ratio of men having abdominal fat.
Nakajima et al.22) showed correlation between FVC and metabolic syndrome level, such as an increase in the sum of metabolic syndrome diagnostics factors. The research demonstrated that an increase in the severity of metabolic syndrome impairs lung function in men but not in women. The results indicate that in addition to the relationship between each metabolic syndrome factor and weaker pulmonary function, people with more metabolic syndrome factors are more vulnerable to pulmonary function impairment. Therefore, additional studies on how to control these metabolic factors to influence pulmonary function in metabolic patients is necessary.
Not much research has been conducted on the association between metabolic syndrome components and lung function impairment. Since such studies were almost non-existent in Korea, this research regarding pulmonary function impairment in Asians is very significant. It is also meaningful in showing the relationship between pulmonary function, metabolic syndrome, and sex, as such studies had never previously been performed.
However, given that the analysis was conducted on Koreans coming from a certain region and health examinees, it is hard to generalize the outcome of the research to all ethnic groups. Also, since women were not classified into groups before and after menopause, the results may not be statistically significant and should be validated further through additional research. The research had some constraints as a cross-sectional study with not many morbidly obese patients included in the analysis. Further research should be conducted, and in particular, studies on morbidly obese patients are also necessary.