INTRODUCTION
Coffee has phenolic compounds such as chlorogenic acid and caffeic acid that have strong antioxidant activity and anti-inflammatory effects, as well as the potential to induce autophagy.1,2,3,4) Considering these pharmacological benefits of coffee, studies have been conducted to investigate the association between coffee consumption and several clinical conditions. The results of these studies suggest that habitual coffee consumption is associated with lower prevalence of diabetes or pre-diabetes,5) insulin resistance,6) stroke,7) Parkinson's disease,8) and cardiovascular disease.9) There is also evidence that coffee consumption is associated with decreased risks for some types of cancer.10)
Sarcopenia has been defined as the loss of muscle mass and strength,11) which is progressive, and mainly related to age.12) It can result in mobility disorders, physical disability, poor quality of life, and even death.13) Several factors are related to the pathogenesis of sarcopenia. Age-related changes such as decreased levels and sensitivity of anabolic hormones, lack of physical activity, nutritional deficiencies, and comorbid diseases all contribute to the onset and progression of sarcopenia. These changes are hypothesized to lead inflammation with increased circulating levels of inflammatory cytokines, oxidative stress, suppressed muscle autophagy, and increased apoptosis by altering intra- and extracellular processes.14,15,16) In addition, oxidative metabolism generates reactive oxygen species, which alters skeletal muscle mitochondrial DNA and can lead to sarcopenia.17)
In one animal trial of aged mice to examine the effect of coffee on skeletal muscles, coffee attenuated the reduction of age-related muscle weight and muscle power, and stimulated regeneration of injured muscle compared to controls. Furthermore, pro-inflammatory mediators such as tumor necrosis factor-alpha and interleukin 6 decreased after coffee treatment.18)
Despite these findings, studies of the effect of coffee on sarcopenia in humans are uncommon. In this epidemiological study, we analyzed the association of coffee consumption and sarcopenia in elderly Korean men.
METHODS
1. Study Population
Data are from the cross-sectional survey of the second and third year (2008–2009) of the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV) and the first and second year (2010–2011) of the KNHANES V, conducted by the Korea Centers for Disease Control and Prevention (KCDC). Originally conducted in 1998, the KNHANES is performed periodically as a cross-sectional and nationally representative survey to investigate the general health and nutritional status of the Korean population. It uses a complex, stratified, multistage, probability-cluster sampling method, which enables the collection of extensive and nationally representative data. The protocols for the KNHANES IV and V were approved by the institutional review board of the KCDC (2008-04EXP-01-C, 2009-01CON-03-2C, 2010-02CON-21-C, 2011-02CON-06-C). All participants provided written informed consent before completing the survey, which included a health interview, a nutritional survey, and a health examination. Data were collected via household interviews and standardized physical examinations. During the period from 2008 to 2011, 9,043 males took part in the KNHANES, and 2,451 men aged 60 years or older. Within the sample of men who were at least 60 years of age, individuals with stroke (144), myocardial infarction or angina (153), liver cirrhosis (17), renal failure (12), or cancer (344) were excluded. The final 1,781 subjects were included for the analysis.
2. Assessment of Coffee Intake
Self-reported coffee consumption data were obtained through dietary interviews. A food frequency questionnaire was used to assess the usual dietary intake over the preceding year. Participants were asked how many cups of coffee they drank during a day, a week or a month. In the questionnaire, the frequency of coffee intake was classified into ten categories: rarely, 6–11 cups per year, 1 cup per month, 2–3 cups per month, 1 cup per week, 2–3 cups per week, 4–6 cups per week, 1 cup per day, 2 cups per day, and 3 or more cups per day. Four coffee consumption groups were constructed: less than 1 cup per day (<1 cup), 1 cup per day (1 cup), 2 cups per day (2 cups), and 3 or more cups per day (≥3 cups), because of the excessively small samples and the small differences between data of each section of the four groups. No distinction was made between caffeinated and decaffeinated coffee, or between the individual types of coffee (boiled, filtered, or instant).
3. Definition of Sarcopenia
Whole and regional body compositions of participants were measured using dual-energy X-ray absorptiometry (DXA, Discovery-W fan-beam densitometer; Hologic Inc., Bedford, MA, USA). According to the definition of sarcopenia proposed by Baumgartner et al.,11) we summed the muscle mass of the four limbs from DXA as appendicular skeletal muscle mass (ASM) and defined a skeletal muscle mass index (SMI) as ASM divided by height squared, ASM/height2 (kg/m2). The cutoff value for sarcopenia was 2 standard deviations (SDs) below the mean SMI of young males (20–39 years). Participants were divided into groups with and without sarcopenia.
4. Statistical Analysis
We applied weights from the KNHANES to calculate estimated means, proportions, and standard errors for the Korean population. We also used complex-sample logistic regression analysis to evaluate the relationship between sarcopenia and coffee consumption. Results were considered to be statistically significant when the P-value was less than 0.05. To estimate P for trends, coffee consumption group variable was regarded as a continuous variable in the trend analysis. Data were analyzed using IBM SPSS ver. 20.0 for Windows (IBM Corp., Armonk, NY, USA).
RESULTS
1. Comparison of the Groups with and without Sarcopenia
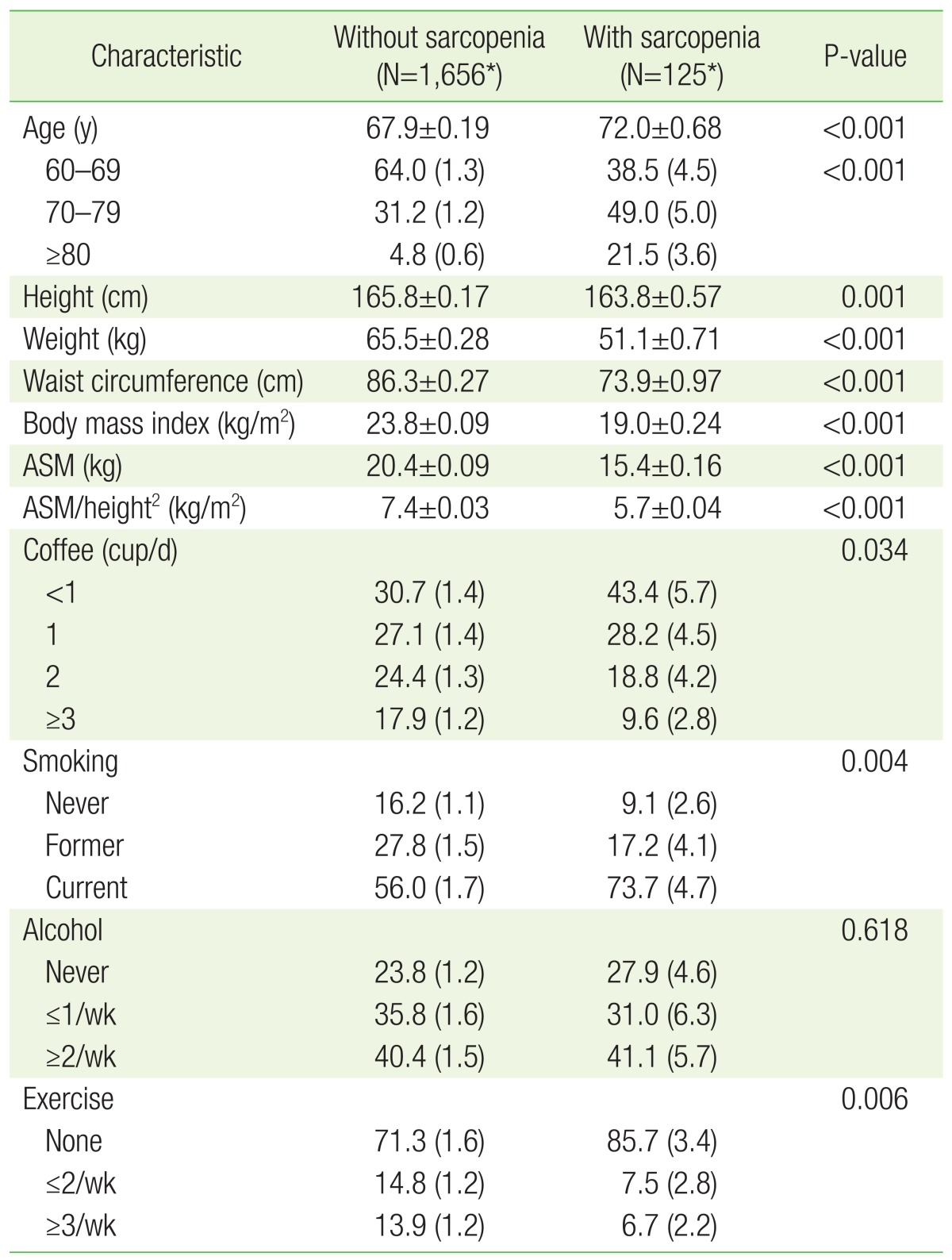
The clinical characteristics of the Korean elderly men who were included in this analysis are shown in Table 1. These estimates were calculated using complex-sample general linear regression and analyzed using complex-sample logistic regression methods (Table 1). All 1,781 study subjects were men aged 60 years or older and their mean age was 68.2 years. With the sarcopenia definition as described in the methods, the cutoff point of sarcopenia in men was 6.07 kg/m2. The mean age of men with sarcopenia was 72.0±0.68 years, which was significantly higher than in men without sarcopenia, 67.9±0.19 years (P<0.001). Similarly, the mean height and weight of individuals without sarcopenia was 165.8±0.17 cm and 65.5±0.28 kg, respectively, while those of the sarcopenia group was 163.8±0.57 cm (P=0.001) and 51.1±0.71 kg (P<0.001). Furthermore, the mean SMI in men without sarcopenia was 7.4±0.03 kg/m2 and 5.7±0.04 kg/m2 in the group with sarcopenia (P<0.001). Smoking status and exercise frequency were significantly different between two groups (P=0.004, P=0.006, respectively), but there was no difference in alcohol consumption frequency (P=0.618).
The proportion of coffee consumption by stratified frequencies was significantly different between the two groups (P=0.034). Additionally, the ratio of the number of persons who drank less than 1 cup of coffee per day and 1 cup per day was relatively higher in the group with sarcopenia than in the group without sarcopenia (43.4% and 28.2% in the group with sarcopenia versus 30.7% and 27.1% in the group without sarcopenia, respectively). Furthermore, the ratios were relatively lower as daily coffee consumption increased to 2 cups and 3 or more cups (18.8% and 9.6% in the group with sarcopenia versus 24.4% and 17.9% in the group without sarcopenia).
2. Baseline Characteristics of the Subjects According to Coffee Consumption Frequency
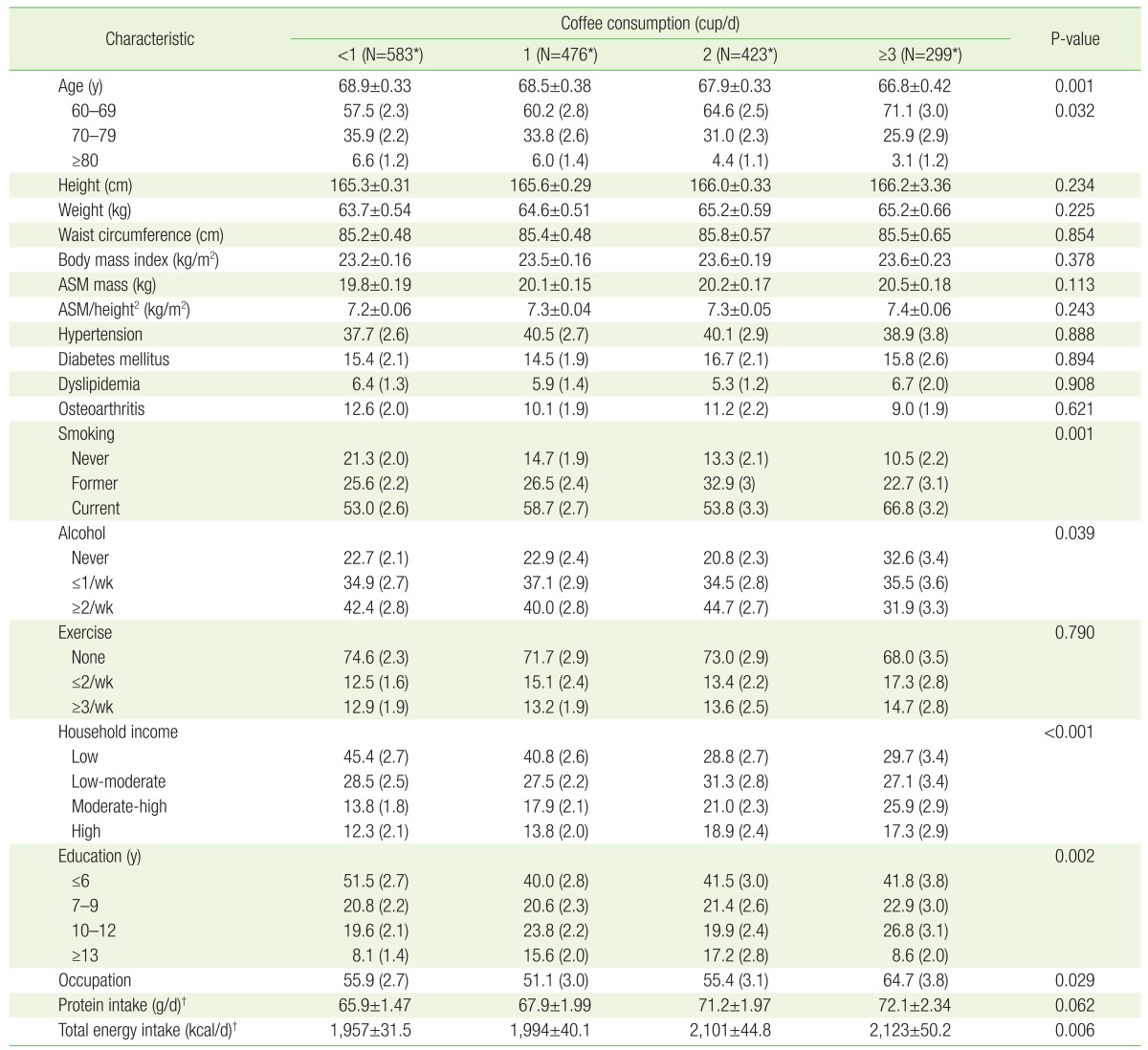
In the unweighted KNHANES data, there were 583 men who consumed less than 1 cup of coffee per day, 476 who drank 1 cup per day, 423 who drank 2 cups per day, and 299 who consumed 3 or more cups. The mean ages were lower as the daily coffee consumption amount increased (P=0.001), but there were no differences in mean height, weight, waist circumference, body mass index, amount of protein intake, or exercise frequency by coffee consumption. Additionally, we observed no significant differences between the means of ASM and SMI by each coffee consumption group (P=0.113, P=0.243, respectively). Among the factors we included in the regression model, smoking, alcohol consumption rate, household income, education, and total energy intake amount were significantly different by daily coffee consumption (Table 2).
3. Relationship between Coffee Consumption and Sarcopenia
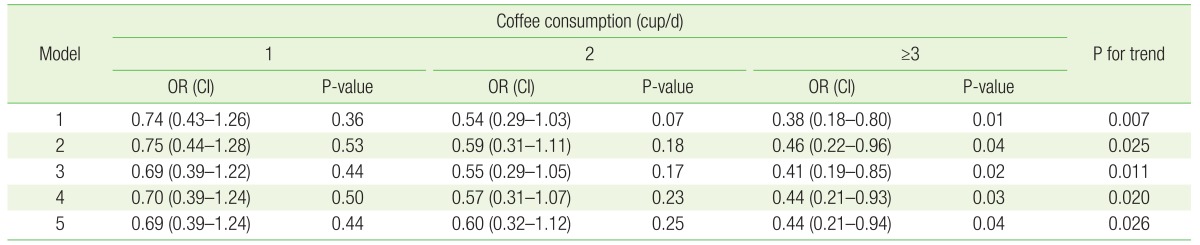
Compared to the reference group of individuals whose daily coffee consumption was <1 cup, sarcopenia was significantly lower in people whose daily consumption was at least 3 cups (odds ratio [OR], 0.38; 95% confidence interval [CI], 0.18 to 0.80), while the prevalence of sarcopenia was not significantly lower for persons who consumed 1 or 2 cups of coffee a day (1 cup: OR, 0.74; 95% CI, 0.43 to 1.26; 2 cups: OR, 0.54; 95% CI, 0.29 to 1.03) without any adjustment (model 1 in Table 3). This result was also observed after adjusting for covariates as shown in Table 3. Notably, the prevalence of sarcopenia was significantly lower in individuals who drank at least 3 cups of coffee per day, even after adjusting for age, smoking, alcohol, exercise, education, household income, occupational status, protein intake, and energy intake (adjusted OR, 0.44; 95% CI, 0.21 to 0.94) (model 5 in Table 3).
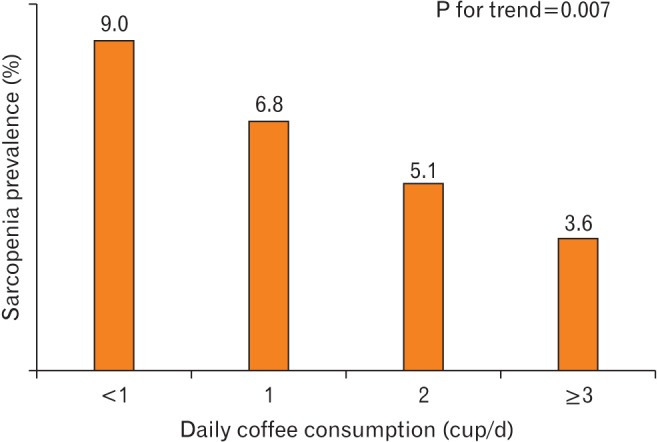
The prevalence of sarcopenia was 7% (n=125) in the unweighted study population, while the estimated rate of sarcopenia was 9.0% among people who drank less than one cup of coffee per day, 6.8% among individuals who drank 1 cup per day, 5.1% in persons who consumed 2 cups of coffee per day, and 3.6% among individuals who drank at least 3 cups of coffee per day, as shown in Figure 1 (P for trend=0.007). After adjustment for age (model 2), the estimated prevalence of sarcopenia still decreased significantly as daily coffee consumption increased (P for trend=0.025). This significant pattern continued in the multivariate-adjusted model 3, 4, and 5 as shown in Table 3 (P for trends=0.011, 0.020, and 0.026, respectively).
DISCUSSION
Because sarcopenia is mainly related to aging, we expected the mean age of the group of sarcopenia to be higher than the group without sarcopenia, and the analyzed results were in good accord with the expected results (72.0 years old in persons with sarcopenia versus 67.9 years old in individuals without sarcopenia). In the present study, coffee consumption was associated with a significantly decreased risk of sarcopenia. This observed association was independent of age, lifestyle (alcohol consumption, smoking, and exercise), degrees of education and household income, and nutrition status (protein and energy intake). Furthermore, a significant linear trend was observed across the levels of coffee consumption. Study participants who consumed 3 or more cups of coffee per day had a 62% lower risk of sarcopenia, compared with those who drank less than 1 cup of coffee per day in unadjusted analyses. In contrast, individuals who consumed at least 3 per day had a 57% lower risk of sarcopenia after adjustment for the covariates mentioned above.
There are some supporting explanations about the preventive effect of coffee on sarcopenia. According to the mitochondrial free radical theory of aging, mitochondrial dysfunction due to oxidative damage to mitochondrial DNA is a major mechanism in the aging process.19) Autophagy is essential for proper renewal of mitochondria and maintenance of muscle mass. As a result, the autophagy rate should be increased by various stresses on muscle cells like exercise or starvation.20) It has also been shown that autophagy is deficient in aged muscle and may affect to mitochondrial dysfunction, enhanced oxidative stress, and the decline of muscle homeostasis which occurs during the aging process.16) According to Pietrocola et al.,4) chronic consumption of coffee diluted in the drinking water of female mice stimulated autophagy in the liver, heart, and skeletal muscle in a dose-dependent manner. Additionally, polyphenols, the main antioxidant component of coffee, have been shown to induce autophagy.21) Because of its antioxidant properties, it is conceivable that coffee may lower the risk of sarcopenia by reducing oxidative stress of mitochondria of muscle cells.
For the definition of sarcopenia, SMI could be calculated in 2 methods representatively; ASM divided by height squared (ASM/height2) or by weight (ASM/weight).11,22) In addition to various definition of SMI, the cutoff values could be chosen differently: (1) less than 1 SD below the mean values of healthy adults, (2) less than 2 SDs below the mean values of healthy adults, or (3) the lowest quintile of study populations.23,24) In our study, the overall prevalence of sarcopenia was 7.5% in Korean men aged 60 years or older. We used ASM/height2 index with 2 SDs below the mean values of healthy adults as the cutoff value. There have been many investigations about sarcopenia in Korea and the prevalence of sarcopenia and its effects on various health conditions are different according to the methods used to define sarcopenia.25) In an observational study by Kim et al.26) on the association of sarcopenia with cardiometabolic risk factors in elderly aged 65 years or older, the prevalence of sarcopenia was 35.5% in men and 13.4% in women using the ASM/height2 index. In contrast, when they used ASM/weight index, the prevalence estimates rose to 37.3% for men and 62.6% for women. In another study, sarcopenia was defined as an ASM-adjusted weight index less than 2 SDs below the mean of healthy adults (20–39 years), and the prevalence of sarcopenia in participants older than 50 years was 7.8%.27) The difference of sarcopenia prevalence was due to different cutoff values of SMI and the difference in age and sex in the study population.
Several published studies offer insight into the role of dietary factors, including coffee, to prevent sarcopenia. According to Kim et al.,28) Korean men at least 65 years of age who consumed the highest quintile of vegetables, fruits and vegetables, and fruits consumption had 52%, 70%, and 68% lower risk of sarcopenia compared with those in the lowest quintile of vegetable, fruit, and vegetables and fruit consumption. These results were hypothesized to be related to the antioxidant effects of vegetables and fruits on sarcopenia. Kim et al.27) also demonstrated that vitamin D levels were significantly lower in subjects with sarcopenia compared with those without sarcopenia.
In this study, we hypothesized that coffee might be associated with a reduced risk of sarcopenia in humans through its antioxidant, anti-inflammatory, and pro-autophagy effects described in previous animal trials.21) Our results support this hypothesis. To our knowledge, this is the first human study to examine the correlation between coffee consumption and sarcopenia. These data support the potential role of coffee in helping prevent sarcopenia18) via the theoretical mechanism of coffee on sarcopenia.29) Another strong point of this study is that the study sample was obtained from a reliable nationally representative population database, lending credence to the generalizability of the findings, which were statistically significant even after adjustment for covariates including demographic and health-related variables.
This study has some limitations. First, coffee consumption was estimated by asking individuals to recall the amounts of coffee they drank daily on average over the preceding year. The data did not take into account any changes of consumption over the person's lifetime. Second, because the study was performed using a cross-sectional design, there is limitation to detect the causal relations or mechanism of action. Third, we cannot completely exclude the possibility that confounding due to consumption of herb tea, green tea, vegetables, fruits, or other substances that provide antioxidants.
In conclusion, this study is a large population-based study to examine the association between coffee consumption and sarcopenia. High consumption of coffee was associated with a lower risk of sarcopenia in elderly Korean men.