INTRODUCTION
With a rapid increase in the number of older adults in Korea, new concepts and approaches are emerging regarding the treatment of conditions in older patients; one such condition is sarcopenia. Sarcopenia is a syndrome of progressive skeletal muscle loss [1]. In 2010, the European Working Group on Sarcopenia in Older People first proposed a diagnostic algorithm for sarcopenia to foster advances in identifying and caring for people with sarcopenia [2]. However, to diagnose sarcopenia in Asian people, it is necessary to identify differences from their Western contemporaries in terms of anthropometric, cultural, and lifestylerelated factors, such as relatively smaller body sizes, higher adiposity, and less mechanized and more physically active lifestyles [3,4]. In 2014, the Asian Working Group for Sarcopenia (AWGS) consensus defined sarcopenia as ŌĆ£age-related loss of muscle mass, plus low muscle strength, and/or low physical performanceŌĆØ and specified cut-offs for each diagnostic component [3]. With advancements in research in Asia, AWGS updated their guidelines for diagnosing sarcopenia in 2019; they retained the previous definition of sarcopenia but revised the diagnostic algorithm, protocols, and some criteria [4]. AWGS 2019 also introduced the term ŌĆ£possible sarcopenia,ŌĆØ which is defined as low muscle strength with or without low physical performance, specifically for use in primary health care or community-based health promotion to enable early lifestyle interventions [4]. Muscle mass peaks in the age of 20s and 30s, and then it gradually decreases. During the age of 40ŌĆō70 years, muscle mass decreases by 8% every 10 years; after 70 years of age, it decreases by nearly 10% in 10 years. Additionally, muscle strength decreases faster than muscle mass. After 70 years of age, it decreases by 25%ŌĆō35% in 10 years, and both muscle mass and strength decrease faster in men than in women [5]. Based on the AWGS 2019 criteria, one study found that 21.3% and 13.8% of Korean men and women aged 70ŌĆō84 years had sarcopenia, respectively [6]. Additionally, the coronavirus disease 2019 was an extraordinary emergency, which became a pandemic. While quarantine and social distancing appeared essential at the time, the harmful physical and psychological health effects of such measures cannot be ignored [7]. Sedentary lifestyle and a lack of a healthy diet brought upon by these measures can significantly increase the prevalence of sarcopenia [8]. In fact, sarcopenia is strongly associated with adverse outcomes, such as falls, fractures, frailty, morbidity, mortality, and high healthcare utilization [1,9]. Despite its clinical importance, sarcopenia remains underrecognized and poorly managed in routine clinical practice. Furthermore, while many studies have evaluated the association between sarcopenia and physical health, there is a lack of studies that have evaluated the association between sarcopenia with mental health conditions, including depression.
Depression, a major mental health disorder, is a mood disorder with symptoms that include persistently depressive mood, loss of motivation or interest, and hopelessness about the future, which could lead to suicide [10]. Since 2001, epidemiological surveys on mental disorders in Korea have been conducted every 5 years with a gradually increasing reported lifetime prevalence of depression (2001, 4.0%; 2006, 5.6%; and 2011, 6.7%) [11]. Depression are closely associated with various health problems in older adults, such as chronic disease, disability, morbidity, and mortality [10,12]. Considering the various adverse outcomes associated with sarcopenia and depressive symptoms in older people, it is important to understand the association between these disorders. To our knowledge, some studies in Asia (e.g., China and Japan) have evaluated the association between sarcopenia and depressive symptoms; however, such studies are lacking in Korea [13,14]. Particularly, no studies have evaluated the relationship between possible sarcopenia and depressive symptoms in Korea. Additionally, the contribution of possible sarcopenia toward specific depressive symptoms remains unexplored. Therefore, we investigated the association between possible sarcopenia and specific depressive symptoms in Korean older adults. Using the nationally representative data from the 2018 Korea National Health and Nutrition Examination Survey (2018 KNHANES), we conducted cross-sectional analyses to estimate the association between possible sarcopenia and depressive symptoms in Korean community-dwelling older adults. If an association is identified, patients should be screened for possible sarcopenia using tests that can be performed quickly and easily in the clinic when they visit the primary health care centers. If possible sarcopenia is identified in them, they should also be screened for depressive symptoms. Consequently, primary care physicians can advise early lifestyle interventions for such patients. The purpose of this study was to examine the relationship between possible sarcopenia and depressive symptoms so that Korean older adults can receive early interventions for these disorders at primary health care centers.
METHODS
1. Study Population
KNHANES is a nationwide cross-sectional survey conducted by the Ministry of Health and Welfare with the aim of identifying and assessing the health and nutritional status of Koreans. The survey is performed annually using systematically stratified multistage clustered probability sampling methods based on the town units of dong, eup, and myun, as well as housing type and age group. All participants are assessed using a standardized questionnaire to collect data regarding sociodemographic, anthropometric, health-related, and lifestyle factors. The 3rd year of the seventh survey (KNHANES VII-3, namely 2018 KNHANES) was conducted between January and December, 2018. The present study used the data from 2018, and the latest data also included results of the hand-grip strength test.
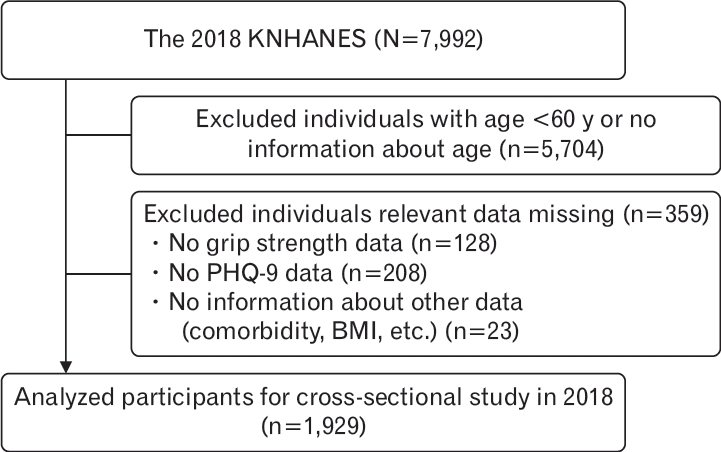
In the survey, 7,992 participants from 3,518 households were recruited from 192 districts in Korea. The data included individual weighted variables to ensure that the survey sample was representative of the nation. In our study, the inclusion criteria were the following: (1) age Ōēź60 years and (2) available scores of hand-grip strength test and Patient Health Questionnaire-9 (PHQ-9). The exclusion criteria were the following: (1) missing results of hand-grip strength test; (2) no PHQ-9 scores; (3) missing age; (4) age <60 years; and (5) no information about other data, including comorbidities and body mass index (BMI). Of the 7,992 participants who were screened, 128 individuals with missing results of the hand-grip strength test, 208 individuals without PHQ-9 scores, 5,704 individuals without age information or aged <60 years, and 23 individuals without additional information were excluded from the study. The remaining 1,929 participants were enrolled in this cross-sectional analysis. A flowchart depicting the selection of participants is presented in Figure 1. All participants provided written informed consent to participate in the study. Approval for this study was obtained from the Ethics Committee of the Catholic University of Korea (approval number: KC22ZASI0533).
2. Assessment of Possible Sarcopenia
Based on the AWGS 2019 criteria, the status of sarcopenia was classified into the following three types: no sarcopenia, possible sarcopenia, and sarcopenia. In our study, however, we included only possible sarcopenia as it can provide an opportunity for early interventions in primary healthcare settings without needing advanced diagnostic equipment. Possible sarcopenia includes the following two components: muscle strength and physical performance. Therefore, possible sarcopenia is diagnosed based on low muscle strength with or without low physical performance. In our study, we used only muscle strength to define possible sarcopenia. Almost all studies in Asia that focused on muscle strength and sarcopenia used hand-grip strength to represent skeletal muscle strength; therefore, AWGS 2019 recommends handgrip strength to represent muscle strength [4]. We measured hand-grip strength (kg) in both the dominant and non-dominant hands. The participants squeezed a digital grip strength dynamometer (TKK-5401; Takei, Niigata, Japan) as hard as possible thrice for each hand. The highest value (often in the dominant hand) was used to identify possible sarcopenia. The cut-off points for low grip strength were 28 kg for men and 18 kg for women.
3. Assessment of Depressive Symptoms
In the 2018 KNHANES, depressive symptoms were assessed using the PHQ-9, which is a screening tool for criteria-based diagnoses of depression and other mental disorders that are commonly encountered in primary care with comparable sensitivity and specificity in older Korean individuals [15,16]. The PHQ-9 consists of the following nine items: (1) little interest or pleasure in doing things; (2) feeling down, depressed, or hopeless; (3) trouble falling or staying asleep or sleeping too much; (4) feeling tired or having little energy; (5) poor appetite or overeating; (6) feeling bad about yourself or that you are a failure; (7) trouble concentrating on things, such as reading the newspaper or watching television; (8) moving or speaking so slowly that other people could have noticed or the oppositeŌĆöbeing so fidgety or restless that you have been moving around a lot more than usual; and (9) thoughts that you would be better off dead or of hurting yourself in some way. Each of the items is scored from 0 (not at all) to 3 (nearly every day) over the past 2 weeks. The total sum of scores ranges between 0 and 27. Depressive symptoms were identified if the score was at least 10 [15,16].
4. Assessment of Covariates
The covariates evaluated included individual sociodemographic characteristics and health-related factors. Individual sociodemographic variables included age, sex, marital status (ever married or never married), education (elementary school or lower, middle or high school, and college or higher), and socioeconomic status. We defined three socioeconomic groups based on the household income quintile (lower class: quintile 1; middle class: quintiles 2ŌĆō4; and upper class: quintile 5) [17]. Health-related factors included smoking (yes: currently smoking or no: ex-smoking or never smoked); drinking (yes: was recommended cessation of alcohol or concerned about drinking by a doctor or family or no: never received such recommendations or concerns); BMI; chewing problems (yes or no); physical activity (yes: 3 or more times a week or no: less than 3 times a week); and 18 physician-diagnosed chronic conditions (hypertension, dyslipidemia, diabetes, stroke, myocardial infarction, angina, arthritis [including osteoarthritis], rheumatism, osteoporosis, asthma, thyroid disease, cancer, anemia, depressive disorder, renal failure, hepatitis B, hepatitis C, and liver cirrhosis). The levels of physical activity were evaluated using the number of walking exercises or strength exercises per week and divided into two categories: yes, 3 or more times a week; no, less than 3 times a week [18]. BMI was calculated as weight (kg) divided by height (m2) and was divided into the following three categories: underweight (BMI <18.5 kg/m2), normal weight (18.5Ōēż BMI <25.0 kg/m2), and overweight or obese (BMI Ōēź25.0 kg/m2) [19].
5. Statistical Analysis
Since the KNHANES survey used a complex sampling design, a complex sampling design analysis was performed using weighted variables. Continuous variables in the current study were expressed as mean┬▒standard error, and categorical variables were expressed as number (percentage). First, the baseline characteristics (sociodemographic and health-related characteristics) were summarized according to the sarcopenia status (possible sarcopenia versus no sarcopenia). Comparisons between continuous variables were performed using Student t-test, and comparisons between categorical variables were performed using chi-square test. Second, logistic regression analysis was used to estimate any association between possible sarcopenia and depressive symptoms after adjusting for potential covariates. Third, we also examined the associations between possible sarcopenia and depressive symptoms after adjusting for age (participants in their 60s versus participants over 70 years of age) using logistic regression analysis. Similar analyses were performed for associations between possible sarcopenia and specific depressive symptoms by coding the questionnaire items as dichotomous variables. Dichotomous variables were used to define the responses (each score Ōēź1 for the 9 items of the PHQ) as having the specific depressive symptoms. Logistic regression analysis was used to calculate the odds ratio (OR) and 95% confidence intervals (CI). All statistical analyses were performed using the IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA). For all tests, P<0.05 was considered statistically significant.
RESULTS
1. Characteristics of Participants
Overall, 1,929 participants (mean age, 69.7┬▒6.5 years) were enrolled in this study. Of them, 861 (44.6%) were men, and 1,068 (55.4%) were women. The baseline characteristics of the participants are summarized in Table 1. The prevalence of possible sarcopenia was 27.9% (538/1,929). Possible sarcopenia was significantly associated with older age, male sex, lower socioeconomic status, lower educational level, chewing problems, consumption of alcohol, smoking, lower BMI, lower physical activity, and chronic comorbidities (including hypertension, diabetes, stroke, arthritis [including osteoarthritis], rheumatism, osteoporosis, anemia, and depressive disorders) (all P<0.05).
2. Association between Possible Sarcopenia and Depressive Symptoms
In this study, people with possible sarcopenia had higher PHQ-9 scores than those without sarcopenia. The prevalence of depressive symptoms in the overall population and those with possible sarcopenia and no sarcopenia was 5.0% (97/1,929), 7.8% (42/538), and 4.0% (55/1,391), respectively (P<0.001) (Table 1). Participants with possible sarcopenia had significantly higher odds of depressive symptoms than those without sarcopenia (OR, 2.06; 95% CI, 1.36ŌĆō3.11; P<0.001) (Table 2). Table 2 summarizes the association between possible sarcopenia and depressive symptoms according to the age group. Compared with participants without sarcopenia, possible sarcopenia was positively associated with depressive symptoms in participants in their 60s (OR, 2.41; 95% CI, 1.16ŌĆō5.02; P<0.05) and those over 70 years of age (OR, 1.91; 95% CI, 1.09ŌĆō3.37; P<0.05).
Table 3 summarizes the association between possible sarcopenia and specific depressive symptoms. Of the nine depressive symptoms in PHQ-9, possible sarcopenia was significantly associated with the following four symptoms (all P<0.05) (Table 3): thoughts that you would be better off dead or of hurting yourself in some way (OR, 2.74; 95% CI, 1.89ŌĆō3.97); moving or speaking so slowly that other people could have noticed or the oppositeŌĆöbeing so fidgety or restless that you have been moving around a lot more than usual (OR, 2.13; 95% CI, 1.37ŌĆō3.29); poor appetite or overeating (OR, 1.48; 95% CI, 1.10ŌĆō1.98); and trouble concentrating on things, such as reading the newspaper or watching television (OR, 1.48; 95% CI, 1.01ŌĆō2.16).
DISCUSSION
In the present study, we used the data from 2018 KNHANES. To our knowledge, our study was the first attempt to identify associations between possible sarcopenia and depressive symptoms in Korean older adults using a large nationally representative survey of the Korean population. We found that possible sarcopenia, assessed using the AWGS 2019 algorithm, was positively associated with higher odds of depressive symptoms. Individuals with low hand-grip strength were more likely to have a higher PHQ-9 score than those without sarcopenia. These findings are consistent with those of many other cross-sectional studies, suggesting that sarcopenia is closely correlated with higher odds of depressive symptoms. A meta-analysis of 15 observational studies indicated that sarcopenia was independently and positively associated with depression both in the narrative review and quantitative analysis with and without adjustments for covariates [20]. Furthermore, China Health And Retirement Longitudinal Study 2015 reported that possible sarcopenia was associated with higher odds of depressive symptoms in 2,627 Chinese older people [14]. The Toyota Prevention Intervention for Cognitive Decline and Sarcopenia study reported that both low physical performance and muscle strength were significantly associated with depressive mood in 432 Japanese older adults; however, no association was noted with decreased muscle mass [13]. Other than studies from Asia, several other studies have evaluated the association between sarcopenia and depressive symptoms. For example, the Brazilian Longitudinal Study of Adult Health suggested that depression was associated with sarcopenia as defined by the National Institutes of Health criteria in 5,927 middle-aged and older Brazilian adults; this association was mainly due to low muscle strength [21]. Few studies have been conducted in Korea on this subject [22,23]. However, none of the them have evaluated the association between possible sarcopenia and depressive symptoms in Korea using the AWGS 2019 algorithm. Byeon et al. [22] in 2016 evaluated the association between sarcopenia and depression; they defined sarcopenia as a decrease in muscle mass only. They reported no association between sarcopenia and depression in 7,364 Korean adults aged Ōēź20 years [22]. However, decreased muscle strength is the most important diagnostic parameter in guidelines for diagnosing sarcopenia since it mainly predicts adverse outcomes [9]. Therefore, we assumed that muscle strength is more important than muscle mass in the present study. This assumption led us to find that possible sarcopenia was positively associated with higher odds of depressive symptoms. Furthermore, we found the association between possible sarcopenia and depressive symptoms based on age cut-off, as well as possible sarcopenia and specific depressive symptoms. Compared with participants with no sarcopenia, possible sarcopenia in participants in their 60s and those over 70 years of age was positively associated with depressive symptoms. Possible sarcopenia was significantly associated with four of the nine depressive symptoms on PHQ-9.
Several possible mechanisms might help explain the association between sarcopenia and depressive symptoms. First, chronic inflammation is common to both sarcopenia and depressive symptoms. Agerelated chronic low-grade inflammation characterized by proinflammatory cytokines, such as tumor necrosis factor-╬▒ and interleukin-6, has been reported as an important biological event in the pathogenesis of sarcopenia and depressive symptoms [24,25]. Second, excessive oxidative stress related to chronic diseases might also cause sarcopenia [24]. Excessive oxidative stress might also possible mediators of known environmental risk factors in depressive symptoms [25]. Third, people with sarcopenia or depressive symptoms are more likely to have similar lifestyle factors, such as malnutrition and physical inactivity [1,10]. Among essential amino acids, branched-chain amino acids (BCAAs) are the most involved in the direct stimulation of muscle protein synthesis, and the mammalian target of rapamycin (mTOR) regulates cell growth, cell proliferation, cell survival, cell motility, protein synthesis, autophagy, and transcription [26]. These facts suggest that BCAA deficiency and dysregulated mTOR pathway might be involved in the pathogenesis of sarcopenia. Reduced activation of mTOR due to BCAA deficiency could play a crucial and unrecognized role in the etiology of depressive symptoms and lower energy metabolism in patients with major depression [26]. Therefore, good nutrition (especially proteins and amino acids) is important for the resolution of depressive symptoms and sarcopenia. Particularly, intake of leucine alone can activate several intracellular signaling proteins involved in the initiation of mRNA translation, including mTOR, which is associated with a decrease in depressive symptomatology while stimulating muscle protein synthesis [26,27]. Physical activity can reduce the permeability and function of the blood-brain barrier as it reinforces antioxidative capacity, reduces oxidative stress, and produces antiinflammatory effects [25,28,29]. Exercise improves sarcopenia and depressive symptoms [1,25,29]. Upregulation of mRNA translation is an important regulator of acute increase in exercise-induced muscle protein synthesis [27]. The activation of the mTOR signaling pathway through exercise is associated with an increased rate of muscle protein synthesis and a decrease in depressive symptomatology [26,27].
However, there were limitations to this study. First, there was no information about muscle mass in 2018 KNHANES. Muscle mass is needed to diagnose sarcopenia according to the AWGS 2019 algorithm; therefore, we could not investigate any association between sarcopenia and depressive symptoms. Second, according to the AWGS 2019 guidelines, possible sarcopenia could be diagnosed based on low muscle strength or physical performance. However, in the data from 2018 KNHANES, there was no information about physical performance as proposed by the AWGS 2019 guidelines. Although several studies have proven that low muscle strength, a component of possible sarcopenia, is independently associated with depressive symptoms, the diagnosis of possible sarcopenia based only on low muscle strength might have resulted in errors in identifying participants with possible sarcopenia [13,14,21]. Third, the study used a cross-sectional design; therefore, we could not determine causality. Fourth, this study used observational data, which might include biases due to confounding factors. To reduce such biases, we considered as many factors as possible in the analysis. However, other potential confounding factors, such as nutritional status, food habits, and sleep behavior, could not be ruled out. Finally, Koreans tend to respond subconsciously and negatively to mental health-related questions due to sociocultural factors [30]. Therefore, the prevalence of depressive symptoms might have been underestimated.
Despite these limitations, there were several strengths of this study. First, we used a large and nationally representative sample, thereby enabling the generalizability of our findings to the overall Korean older population. Second, the study was the first one to examine associations between possible sarcopenia and items of depressive symptoms in PHQ-9 in Korean older adults. Third, the scarcity of studies on the topic makes the findings of this study important in determining criteria for associations between possible sarcopenia and other diseases. More importantly, the AWGS 2019 guidelines recommend a new entity ŌĆ£possible sarcopeniaŌĆØ to facilitate early lifestyle interventions. Our findings support the validity of the current major algorithm of possible sarcopenia proposed by AWGS 2019. Therefore, maintaining sufficient muscle strength might be important in combating depressive symptoms in older adults. Additionally, screening for possible sarcopenia and depressive symptoms in routine clinical practice could promote healthy aging.
In conclusion, possible sarcopenia was significantly associated with depressive symptoms in Korean community-dwelling older adults. The results of this study demonstrated that early interventions for possible sarcopenia and depressive symptoms in routine clinical practice could enable Korean older adults to have healthy aging. Additionally, future longitudinal studies, including large-scale cohort studies, are needed to explore any causal relationship between possible sarcopenia and depressive symptoms in Korean community-dwelling older adults.