INTRODUCTION
The World Health Organization (WHO) recommends that all newborns be breastfed exclusively for the first 6 months of life and given nutritionally appropriate and safe supplemental foods, with breastfeeding continuing for up to 2 years of age or beyond [1,2]. Breastfeeding provides appropriate nourishment and contributes to newborn and maternal well-being, resulting in favorable health outcomes [3]. Despite global recommendations and the massive benefits of breastfeeding, its practice is not prevalent globally.
Breastfeeding is extremely popular in Jordan, as evidenced by the fact that 92% of the children in Jordan were nursed at some point in their lives [4]. Nonetheless, the rate of exclusive breastfeeding of 6-month-old babies is less than ideal and is gradually declining in Jordan [4].
Breastfeeding mothers who have newly given birth may face several medical conditions in which there is a need for the use of medications. More than 50% of postpartum women, either breastfeeding or not, use at least one medication [5]. Since contraindicated medications are few, most medications are safe to administer during breastfeeding [6]. However, breastfeeding women may discontinue breastfeeding based on a physician’s advice [7], even for medications that are known to be safe [8]. Although there are several resources for assessing medication safety during breastfeeding, they are frequently conflicting. For example, in the case of ciprofloxacin, the patient information leaflet (PIL) for Bactall (brand name for ciprofloxacin) recommends against its use during breastfeeding and includes the statement: “Do not take ciprofloxacin during breast-feeding” [9]; however, LactMed (Drugs and Lactation Database) reports the acceptance of it use by lactating mothers with monitoring of the infant for possible effects [10]. As a result, some may believe that it is preferable to discontinue breastfeeding rather than risk exposing the newborn to potentially dangerous medicines [11].
Community pharmacists have continuous contact with breastfeeding women and are easily accessible and trusted health consultants [12]. A Gold Coast study found that 78% of pharmacists saw mothers with infants at least once each day [13]. However, pharmacists are less confident than nurses and general practitioners in providing breastfeeding-related advice [13] even though other healthcare providers consider pharmacists reliable sources of medication-related information [14,15]. A study conducted by Ronai et al. [16] in the United States to determine the resources pharmacists use to guide medication recommendations to breastfeeding mothers highlighted the importance of a consistent approach when accessing resources to guide recommendations regarding the use of medications while breastfeeding. Therefore, pharmacists must be capable of providing accurate information from reliable sources. This study aimed to explore the approaches of Jordanian community pharmacists to identifying and counseling breastfeeding mothers regarding medication usage.
METHODS
1. Study Design and Participants
This study followed a descriptive cross-sectional design, and its objectives were addressed through an online survey. The study was conducted in Jordan between August 2021 and February 2022. Participants were recruited using convenience sampling. All approaches were through social media portals (Facebook and WhatsApp groups). The study targets adults aged over 23 years, specifically pharmacists holding at least a bachelor’s degree in pharmacy or Doctor of Pharmacy degree, and who are presently employed in community pharmacies across Jordan. The inclusion criteria were explained at the beginning of the survey. Participation was voluntary and the purpose of the study was explained before accessing the questionnaire. The respondents’ anonymity was preserved. A written consent statement, “Your participation in completing this questionnaire is highly appreciated,” was provided to the participants at the beginning of the survey. If the participants were willing to participate in the survey, their consent was obtained. If not, they selected “disagree to participate” and did not continue with the survey questions. Potential participants who completed the survey were considered to have provided informed consent to participate in the study.
2. Survey Development and Validation
An online survey was developed after reviewing related surveys in the literature [16] and a draft questionnaire was designed. Afterwards, the questions in the draft questionnaire were discussed separately, and all arising comments and concerns were recorded and transcribed. In addition, experts in pharmacy practice other than the research team reviewed the questionnaire for face and content validity. The relevance, specificity, and comprehensiveness of the questionnaires were assessed. The questionnaire was piloted with a small number of participants before the study (n=10) to improve its clarity. Pilot data were not included in the final analysis. The survey contained multiple-choice questions and was designed to be completed within 5–10 minutes. The final version of the survey consisted of three parts. Part one comprised questions assessing women’s sociodemographic information. Part two focused on the approaches used by pharmacists to identify breastfeeding women. Part three assessed pharmacist’s counseling practices in pharmacies with breastfeeding women and the different resources used while providing counseling. The online survey was prepared using Google Forms (Google LLC, Mountain View, CA, USA) and it was a self-administered survey presented in English.
3. Sample Size
The most recent statistics released by the Jordanian Pharmacist’s Association showed that there were 22,667 registered pharmacists as of February 2019 [17]. Sample size was estimated using the Raosoft sample size calculator for online surveys (Raosoft Inc., Seattle, WA, USA). With a margin of error of 5%, confidence level at 95%, population size of 22,667, and response distribution of 50%, the recommended sample size was 378 participants. A decision was made to increase the number of pharmacists to approximately 380 to account for any unknown issues that may arise.
4. Ethical Considerations
Ethical approval for the study was obtained from the Institutional Review Board of King Abdullah University Hospital, University of Science & Technology, Jordan (reference no., 56/141/2021; date: July 29, 2021).
5. Data Analyses
The completed surveys were extracted from Google Forms (Google LLC) as Excel sheets (Microsoft Corp., Redmond, WA, USA) and exported to the IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA) for statistical analysis. Categorical variables were expressed as frequencies or percentages. Univariate analysis was performed using the chi-square test. Statistical significance was set at P<0.05.
RESULTS
1. Sociodemographic Characteristics of the Study Participants
After distributing the online questionnaires, a total of 381 completed questionnaires were included in the study. The majority of participants were female (n=329, 86.4%), with most between 23 and 30 years of age (n=300, 78.7%). Further details regarding participants’ demographic characteristics are presented in Table 1.
2. Pharmacists’ Approaches to Identifying Breastfeeding Women
Pharmacists were asked about their approach to identifying breastfeeding women (Figure 1). The results indicated that more than half of the pharmacists reported that they identified breastfeeding women by asking every woman (n=211, 55.4%), while 17.1% of them (n=65) identified breastfeeding women through their signature waiver, “Yes/no, I am pregnant or breastfeeding.” Very few pharmacists could identify breastfeeding women by relying on medical doctors to relay information (3.7%, n=14) or by relying on breastfeeding women to disclose this information (n=37, 9.7%).
3. Pharmacist’s Counseling Practice for Breastfeeding Women Regarding Medications
Pharmacists were asked about their current counseling practice for breastfeeding women (Table 2), and the results showed that approximately one-third of the pharmacists (n=128, 33.6%) reported that they currently got queries regarding medication use in breastfeeding (including multivitamins/nutritional supplements) on a daily basis; the same percentage of pharmacists also reported getting queries 1–2 times per week. More than a quarter of the pharmacists (n=114, 29.9%) reported that they consult hard copy resources including books, handbooks, or manuals for information regarding breastfeeding women, while approximately fifty percent indicated that they always or most often consult online resources (n=167, 46.4%). Furthermore, almost half of the pharmacists always asked all women if the dispensed medications were for breastfeeding ladies (45%, n=171). Additionally, over two-thirds (67.5%) of the respondents frequently received prescriptions for medications that were not recommended during breastfeeding.
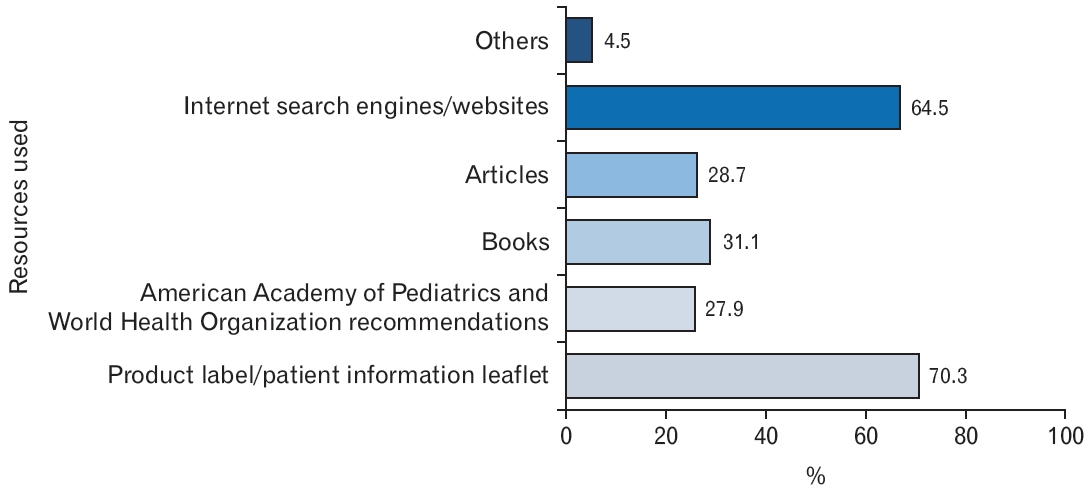
4. Resources Used by Pharmacists for Providing Counseling to Breastfeeding Women Regarding Medications
The surveyed pharmacists reported that they relied on different resources during their course of practice to answer queries related to medicine usage by breastfeeding mothers (Figure 2). More than two-thirds of pharmacists surveyed reported using the product label/PIL (n=267, 70.30%), followed by Internet search engines/websites (n=245, 64.5%) as the main resources. Less than one-third of the participating pharmacists relied on the WHO and American Academy of Pediatrics (AAP) recommendations (n=106, 27.9%). Additionally, 4.5% of the pharmacists (n=17) reported using other resources to approach queries related to medication use, such as using medical applications downloaded on their smartphones, such as Lexicomp and Medscape; obtaining the counsel of the obstetrician-gynecologist; asking the most experienced pharmacist; or asking the medical sales representative.
5. Pharmacists’ Comfort and Confidence Level While Counseling Breastfeeding Women Regarding Their Medications
Pharmacists were asked about their comfort and confidence levels while counseling breastfeeding women regarding their medications (Table 3). The results showed that nearly half the pharmacists reported feeling very comfortable (n=167, 43.8%,) followed by 23.4% of them (n=89) feeling somewhat comfortable while giving advice about medication to breastfeeding women. Moreover, more than one-third of the pharmacists reported feeling very confident (n=150, 39.4%), followed by almost half of pharmacists feeling somewhat confident (n=175, 45.9%) while giving advice to breastfeeding women.
6. Factors Influencing the Comfort and Confidence Levels of Pharmacists
The independent chi-square analysis (Table 4), revealed statistically significant associations between pharmacists’ confidence levels and various factors. Specifically, a significant association was observed between confidence levels and marital status (P=0.026), the frequency of inquiring about dispensed medications for breastfeeding women (P=0.000), and frequency of consulting hardcopy resources for breastfeeding women (P=0.005).
Regarding comfort levels, the findings presented in Table 5 indicate statistically significant associations among three key factors: the frequency of getting queries regarding medication use during breastfeeding (including multivitamins/nutritional supplements) (P=0.034), frequency of asking women if dispensed medications are intended for breastfeeding women (P=0.000), and frequency of consulting a hardcopy resource for breastfeeding women (P=0.038).
DISCUSSION
The study evaluated, for the first time in Jordan, community pharmacists’ counseling practice with breastfeeding women. The results revealed three main findings. First, community pharmacists have continuously interacted with breastfeeding women, and the majority of them had a high level of confidence and comfort while giving advice regarding medication to breastfeeding women. Second, asking every woman is the Jordanian pharmacists’ preferred approach to identifying breastfeeding mothers. Third, pharmacists relied on various resources to answer women’s queries related to medication use during breastfeeding. Finally, additional significant associations were found between pharmacists’ confidence and comfort levels and key factors, such as marital status, frequency of encountering queries on medication use during breastfeeding, asking women whether the dispensed medications were for breastfeeding women, and frequency of consulting hard-copy resources.
These frequent interactions could be attributed to the fact that breastfeeding women are frequently required to take medications [5,18]. Additionally, this could be attributed to the accessibility of community pharmacists, who are seen as easily accessible and trusted health consultants [12,19]. This finding is in line with the findings reported by Ronai et al. [16] in the United States, who reported that nearly half of the pharmacists receive inquiries about medication safety from breastfeeding mothers on a weekly or daily basis.
Almost two-thirds of pharmacists reported frequently receiving prescriptions for medications that are not recommended for breastfeeding mothers. One possible explanation for this result is the low level of knowledge among healthcare providers regarding the safe use of medications during breastfeeding [14]. Inadequate knowledge of drug use during breastfeeding may also lead to insufficient medical history-taking, where essential information is not obtained from lactating mothers. Moreover, some general practitioners have been documented prescribing pregnancy medications for lactation [20], implying that their recommendations to continue or discontinue breastfeeding may be inappropriate. This raises the need to develop a reliable database of medication that are safe for lactating women.
More than two-thirds of pharmacists expressed a high level of confidence and comfort while giving advice to breastfeeding women regarding medication. These findings are similar to those of previous study that reported that most pharmacists felt comfortable advising breastfeeding women [16] and were confident in providing advice to breastfeeding mothers [21,22]. Furthermore, significant associations were revealed between pharmacists’ confidence and comfort levels and key factors such as marital status, frequency of encountering queries on medication use in breastfeeding, asking women whether the dispensed medications were for breastfeeding women, and frequency of consulting hardcopy resources. Regular involvement in queries regarding medication use during nursing is expected to improve pharmacists’ knowledge and expertise, leading to increased comfort in delivering advice. Furthermore, frequent questioning may expose pharmacists to a range of experiences, making them more comfortable and confident in providing advice on medication use during breastfeeding. Moreover, the frequent use of hardcopy resources may help to better understand breastfeeding-related medical information, enhancing confidence and comfort levels.
Because pregnant and breastfeeding women are ethically precluded from clinical trials [23], questions about the consequences of maternal medication use during breastfeeding on newborns are considered to be frequently insufficiently answered. Consequently, there is limited experience regarding the impact of these medications on breastfeeding women at the time of their introduction and marketing, which may prompt medical professionals to advise mothers against nursing [7], even though the drug is safe for use during breastfeeding. This issue is a fundamental obstacle to successful breastfeeding support.
The surveyed pharmacists reported that they relied on different resources during their course of practice to answer queries related to medicine usage in breastfeeding mothers. Both the AAP and WHO issued recommendations on the safe use of medications during breastfeeding. Less than one-third of the participating pharmacists relied on the WHO and AAP recommendations. This may be attributed to the fact that pharmacists are less familiar with these recommendations than physicians are, as reported by Al-Sawalha et al. [14]. Additionally, more than two-thirds of the pharmacists reported relying on the product label/PIL, followed by Internet search engines and websites as the main resources. Pharmacists also rely on printed materials that have a limited shelf life. However, caution should be exercised when using Internet resources, as conflicting advice may be found, and a critical review of the available data is required to derive reliable conclusions. According to Amir and Pirotta [20] in 2009, most general practitioners rely on the Internet, books, or prescription software. A previous study conducted in Australia showed that community pharmacists used a variety of resources and references to assist them, including medicine handbooks, Internet databases or websites, and product manufacturers [24]. This highlights the importance of having reliable and up-to-date data access that pharmacists can access. In addition to the recommendations offered by competent institutions, including the WHO and the AAP, which are frequently regarded as highly reliable sources because of their evidence-based content and conformity to established guidelines, LactMed is a peer-reviewed Toxicology Data Network (TOXNET) database that contains details on the safety of medicines during breastfeeding, encompassing both conventional and alternative medicines [25]. However, none of the pharmacists in our survey had reported the use of this database. This finding emphasizes the necessity of educating pharmacists regarding reliable and accessible resources, especially not just where to obtain them but also how to understand the information that is available. This could include attending workshops or programs that focus on comprehending and assessing the data provided in these resources critically and keeping up with the most recent recommendations and findings in research.
One of the most frequently mentioned challenges in the provision of pharmaceutical care throughout preconception, pregnancy, and breastfeeding is the difficulty in determining a woman’s lactation status [26]. Approximately half of the participants always asked a woman to dispense medications if she was breastfeeding. This could be attributed to the fact that the majority of pharmacists working in Jordanian pharmacies are female [17], which may make it easier for them to ask about women’s lactation status. This finding was consistent when they were asked to determine how they could identify breastfeeding women, and more than half of them could identify breastfeeding women by asking every woman. This finding is inconsistent with the findings reported by Ronai et al. [16] in the United States, who reported that over half of the surveyed pharmacists never asked women whether they were breastfeeding. Furthermore, with regards to identifying breastfeeding women, nearly half of pharmacists believed that such information could be included on a signature waiver in the form of the sentence, “Please check here if you are pregnant or breastfeeding.” [16] These differences in results may be attributed to cultural differences.
A limitation of this study is the participants’ self-selection process. All information was obtained using a self-reported method. There may be inaccurate “social desirability” responses or recall difficulties. However, it is hoped that the anonymity of the questionnaire encourages honesty. Further research is needed to boost the role of pharmacists as someone providing interventions to improve global breastfeeding rates.
In conclusion, this study showed that community pharmacists continuously interacted with breastfeeding women, and the majority had a high level of confidence and comfort while giving advice about medication to breastfeeding women. Asking every woman is the Jordanian pharmacist’s preferred approach to identifying breastfeeding mothers who are mostly concerned about the impact of medication on newborns. Pharmacists require reliable and updated data access to answer queries related to medication use while breastfeeding.