Usefulness of Alcohol-screening Instruments in Detecting Problem Drinking among Elderly Male Drinkers
Article information
Abstract
Background
In Korea, few studies have been performed on screening instruments for the detection of at-risk drinking and alcohol use disorders in the elderly. This study evaluated the validity of three screening instruments in elderly male drinkers.
Methods
The subjects were 242 Korean men aged ≥ 65 years. Face-to-face interviews were used to identify at-risk drinking and alcohol use disorders. At-risk drinking was defined according to the criteria for heavy or binge drinking of the National Institute on Alcohol Abuse and Alcoholism. Alcohol use disorder was diagnosed using the criteria of the Diagnostic and Statistical Manual of Mental Disorders IV-text revision. The Alcohol Use Disorder Identification Test (AUDIT), Short Michigan Alcoholism Screening Test-geriatric version (SMAST-G), and cut down, annoyed, guilty, eye-opener (CAGE) questionnaire were used as the alcohol-screening instruments. Based on the diagnostic interview results, sensitivity, specificity, and area under the receiver operating characteristic curve (AUROC) of the instruments were compared.
Results
For identification of at-risk drinking, the AUDIT AUROC demonstrated greater diagnostic power than did those of SMAST-G and CAGE (both P < 0.001). In screening for alcohol use disorders, the AUDIT AUROC was also significantly higher than those of SMAST-G and CAGE (both P < 0.001). The sensitivity and specificity of screening for at-risk drinking with an AUDIT score ≥ 7 were 77.3% and 85.1%, respectively, whereas those for the alcohol use disorders with an AUDIT score ≥ 11 were 91.3% and 90.8%, respectively.
Conclusion
The results suggest that the AUDIT is the most effective tool in identifying problem drinkers among elderly male drinkers.
INTRODUCTION
Recent age-related domestic population demographics have shown significant growth in the elderly population, indicating that society is aging. In 2007, elderly people (aged ≥ 65) accounted for 9.9% of the total population in Korea, a 3.5% rise compared with 6.4% in 1997. Furthermore, the percentage of elderly individuals in Korea is expected to reach 14.3% in 2018, which is a definite sign of an aging population.1) The ever-growing aging population and the ensuing increase in elderly problem drinkers may lead to an increase in alcohol-induced physical, mental, and social problems.2)
Problem drinking is a comprehensive concept combining at-risk drinking and alcohol use disorders. Specifically, at-risk drinking in elderly males refers to heavy drinking, where a male consumes > 7 standard drinks of alcohol per week, and binge drinking, where a male consumes > 3 alcoholic drinks per drinking session.3) Alcohol use disorders are defined as alcohol abuse or dependence according to psychiatric diagnostic criteria.4) Problem drinking in elderly people raises mental and physical issues. Heavy drinking exacerbates diseases of the digestive system such as cirrhosis, liver cancer, oral cancer, esophageal cancer, and pancreatitis. It also elevates the morbidity rates of cardiovascular diseases, such as atrial fibrillation, hypertension, and stroke, and mental diseases, such as alcohol dependence, depression, anxiety disorders, and suicidal ideation.5,6)
Thus, to solve alcohol-related problems in elderly drinkers, clinicians need to identify problem drinking at its early stages. In clinical settings, however, few cases of alcohol-related problems in elderly drinkers are identified. A study at a university hospital in the Netherlands found that only 33% of elderly alcohol abuse patients were identified by clinicians.7) Likewise, a three-hospital study in Australia reported that just 33% of these patients were discovered by clinical professionals.8) The percentages are remarkably lower compared with the discovery rate (60%) of alcoholism in patients below 60 years of age. In short, 2/3 of elderly drinking problems are not discovered by clinicians.
Such low discovery rates may be due to several factors. First, elderly patients are more vulnerable to alcohol than are younger patients. That is, even when elderly people consume the same amount of alcohol as younger people do, their blood alcohol concentration is higher. Therefore, moderate drinking in young people may constitute heavy drinking in elderly people. This fact is often overlooked. Second, although 90% of elderly individuals with alcohol use disorders are treated for their physical problems, clinicians tend not to pay att ention to drinking problems, which are non-specific and hard to identify.9) Third, negative attitudes toward alcoholism get in the way of making an accurate diagnoses. The stigma of alcoholism often leads alcoholics to drink in solitude, thereby missing the chance to be seen by clinicians at the appropriate time.10)
Evaluating the validity of screening tools used for the assessment of problem drinking in the elderly population is very important in terms of patient care in primary medical care settings. It is most desirable to diagnose at-risk drinking or alcohol use disorders through face-to-face interviews conducted by doctors. When such interviews are impossible, screening questionnaires completed by patients play an important role. Doctors may review the results of screening tests, suspect at-risk drinking or alcohol use disorders, and conduct further interviews for confirmation. Previous Korean studies based on the utility of alcohol questionnaires have focused largely on younger and older adults. Few studies have examined whether the screening tools are suitable for assessing drinking problems in the elderly. Accordingly, the present study attempted to assess the validity of three screening tools commonly used in primary care sett ings to identify problem drinking (at-risk drinking and alcohol use disorders) in elderly male drinkers.
METHODS
1. Study Subjects
Study subjects were 242 male drinkers aged ≥ 65 years who visited the department of Family Medicine at Chungnam National University Hospital between March and August 2009. Subjects agreed to study enrollment prior to filling out the questionnaires, and all participated based on informed consent. Those who were suspected of dementia and cognitive disorders were excluded.
2. Method
1) Diagnostic interview
At-risk drinking and alcohol use disorders were assessed by means of diagnostic interviews conducted by family physicians. To assess at-risk drinking, the amount of alcohol consumption per drinking session and the average frequency of drinking per week were investigated. In this study, based on the criteria set forth by the National Institute on Alcohol Abuse and Alcoholism,3) heavy drinking of more than 7 standard drinks per week or binge drinking of more than 3 drinks per drinking session were defined as at-risk drinking. The standard drink refers to 14 grams of pure alcohol, equal to 1/4 of a bottle of 20% Soju, a small bottle of beer, a bowl of Makgeolli, a glass of wine, or a shot of hard liquor. To categorize alcohol use disorders into alcohol abuse and dependence, a structured interview was used based on the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV TR).4)
2) Questionnaire survey
Upon completing the family physician-led diagnostic interview, subjects were asked to fill out the questionnaires, which included items on socio-demographic characteristics as well as the Alcohol Use Disorder Identification Test (AUDIT), Short Michigan Alcoholism Screening Test-geriatric version (SMAST-G), and acronym referring to four questions (cut down, annoyed, guilty, eye-opener; CAGE) questionnaires. Socio-demographic data included patient's age, religion, residential status, occupation, medical history, smoking status, family history of alcoholism, and age at onset of drinking.
3) Screening instruments
(1) Alcohol Use Disorder Identification Test
The AUDIT was developed in 1989 by the World Health Organization11) and consists of a total of 10 items. Each item is rated on a 4-point scale, for a total of 40 points possible. Of the 10 items, three are related to the frequency of drinking, the amount of alcohol consumption, and the frequency of binge drinking. The AUDIT tool differs from other conventional tools in that it measures heavy drinking and binge drinking, and it does not include any items on withdrawal symptoms. Therefore, the AUDIT is useful to screen for problem drinkers rather than alcohol dependence and thus is suitable for primary care settings. Regarding the validity of the AUDIT in Korea, it was recommended that ≥ 12 points is suggestive of problem drinking, ≥ 15 points is considered 'alcohol use disorders', and ≥ 26 points is indicative of alcohol dependence; with sensitivity and specificity were 85.7% to 96.9% and 79.5% to 100.0%, respectively.12)
(2) Cut down, annoyed, guilty, eye-opener
The CAGE is a questionnaire developed in 1970 that is composed of 4 questions: 1) Have you ever felt that you should cut down on your drinking?, 2) Have people annoyed you by criticizing your drinking?, 3) Have you ever felt bad or guilty about your drinking?, and 4) Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (eye opener)?13) According to a Korean study that assessed the sensitivity and specificity of the questionnaire, a total of two or more positive responses on the questions is indicative of an alcohol use disorder.14)
(3) Short Michigan Alcoholism Screening Test-geriatric version
The SMAST-G consists of 10 questions and was developed by Blow et al.15) based on the 24-item Michigan Alcoholism Screening Test scale to assess drinking problems in the elderly. It is suggested that a score of ≥ 2 indicates problem drinking in an elderly individual. The present study used the SMAST-G as translated by Kim.16)
3. Data Analyses
Descriptive analysis was applied to subjects' socio-demographic characteristics including age, religion, smoking status, and medical history. In identifying the at-risk drinking and alcohol use disorders, receiver operating characteristic (ROC) curve and area under the ROC (AUROC) curve analyses for each screening tool were investigated. The differences between areas among the three screening tools were evaluated using comparisons of paired ROC curves. The sensitivity, specificity, positive predictive value, and negative predictive value of each screening tool were investigated for at-risk drinking and alcohol use disorders. SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA) and MedCalc Statistical Software ver. 10.0 (MedCalc Software, Mariakerke, Belgium) were used for statistical analysis. A P-value < 0.05 was deemed statistically significant.
RESULTS
1. Socio-Demographic Characteristics and Drinking History of the Subjects
The mean age ± SD of the subjects was 71.8 ± 5.5 years. Of the subjects, 151 (62.4%) practiced a religion, 161 (66.5%) were living with guardians, 54 (22.3%) were employed, 73 (30.2%) had a smoking habit, and 115 (47.5%) were on medication due to chronic illness. Regarding educational background of the subjects, 78 (32.2%) had completed primary education, 65 (26.9%) had completed junior high school, 64 (26.4%) had completed senior high school, and 20 (8.3%) had a college degree or higher. A family history of alcoholism was found in 20 (8.3%) subjects.
The mean age at first drinking was 21.1 ± 5.5 years. The frequency of drinking per week was 2.2 ± 1.7 times. The mean amount of alcohol consumed per drinking session was 3.5 ± 2.2 drinks. The mean scores on each tool were 8.0 ± 5.8 points on the AUDIT, 2.7 ± 2.0 points on the SMAST-G, and 1.5 ± 1.2 on the CAGE questionnaire. A total of 95 (39.3%) subjects were found to be heavy drinkers, consuming > 7 drinks per week, 102 (42.1%) were found to be binge drinkers consuming > 3 drinks per drinking session, and 128 (52.9%) were found to be at-risk drinkers. Alcohol dependence was found in 38 (15.7%), alcohol abuse in eight (3.3%), alcohol use disorders in 46 (19.0%), and problem drinking in 131 (54.1%) subjects (Table 1).
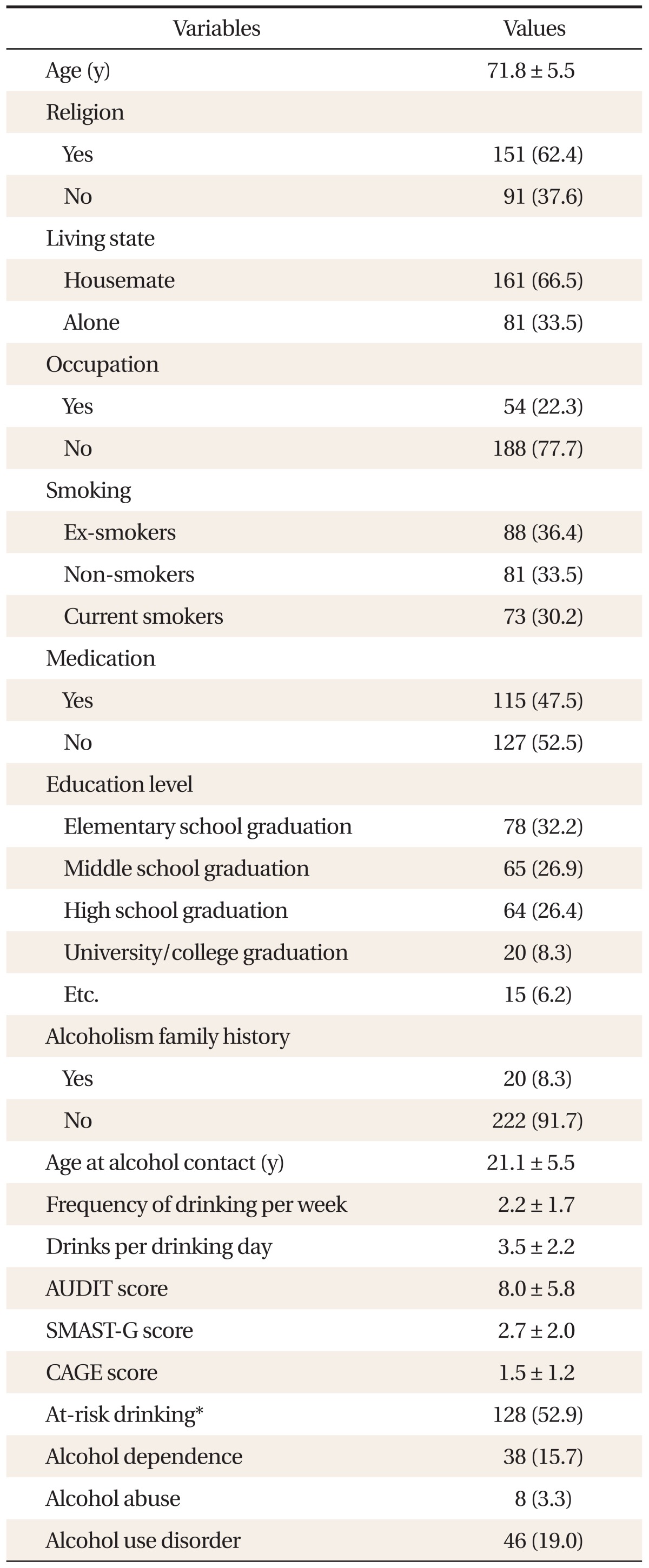
Characteristics of subjects.
2. Validity of Screening Tools for at-Risk Drinking
Regarding the AUROC of the three screening tools used for identifying at-risk drinking in elderly male drinkers aged ≥ 65 years, the AUDIT produced the greatest AUROC (0.903), followed by the SMAST-G (0.742) and CAGE (0.726). The AUROC was significantly greater for the AUDIT than for the SMAST-G (P < 0.001) and the CAGE (P < 0.001). There was no statistically significant difference in AUROC between the CAGE and the SMAST-G (Figure 1).
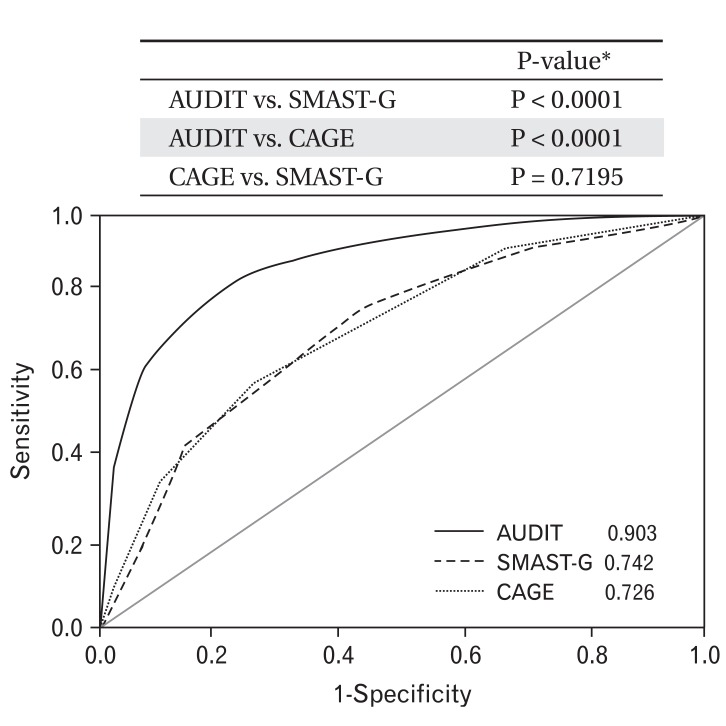
Area under the receiver operating characteristic curves (AUROCs) of screening instruments for identifying at-risk drinking. AUDIT: Alcohol Use Disorder Identification Test, SMAST-G: Short Michigan Alcoholism Screening Test-geriatric version, CAGE: cut down, annoyed, guilty, eye-opener. *Statistical difference between AUROCs by comparison of paired receiver operating characteristic curves.
The optimal cut-off score for the AUDIT in screening for at-risk drinking (where the sum of sensitivity and specificity values was maximal) was 7 points, with sensitivity of 77.3%, specificity of 85.1%, positive predictive value of 85.3%, and negative predictive value of 77.0%. The optimal cut-off score for the SMAST-G in screening for at-risk drinking was 2 points, with sensitivity of 82.0%, specificity of 45.6%, positive predictive value of 62.9%, and negative predictive value of 69.3%. The optimal cut-off score for the CAGE questionnaire in screening for at-risk drinking was 2 points, with sensitivity of 59.4%, specificity of 68.4%, positive predictive value of 67.9%, and negative predictive value of 60.0% (Table 2).
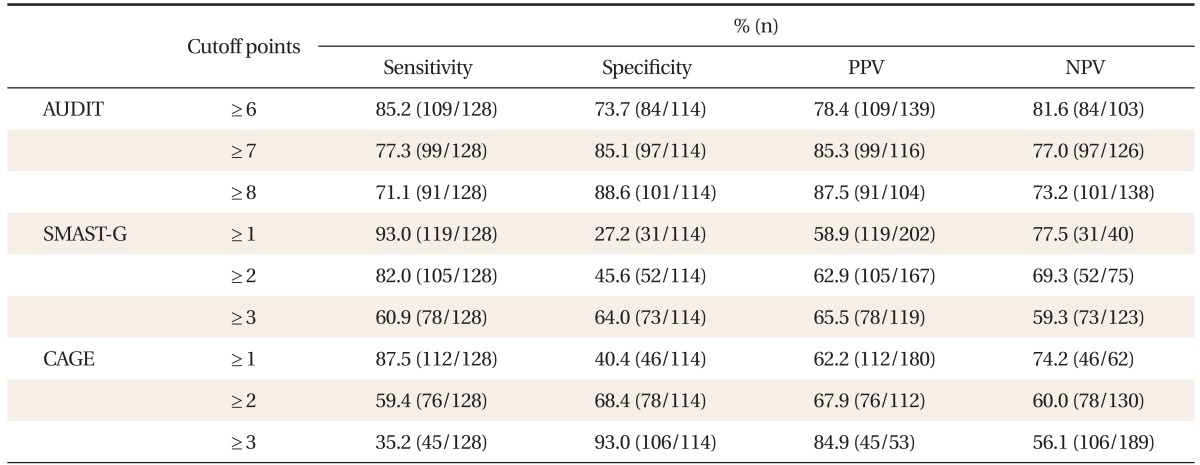
Cutoff points and performance of screening instruments for identifying at-risk drinking.
3. Validity of Screening Tools for Alcohol Use Disorders
Regarding the AUROC values of the three tools for screening alcohol use disorders in elderly male drinkers aged ≥ 65 years, the AUDIT again showed the greatest AUROC (0.954), followed by the SMAST-G (0.815) and the CAGE (0.833). The AUROC was significantly greater for the AUDIT than for the SMAST-G (P < 0.001) and the CAGE (P < 0.001). Meanwhile, there was no statistically significant difference in AUROC values between the SMAST-G and the CAGE questionnaire (Figure 2).
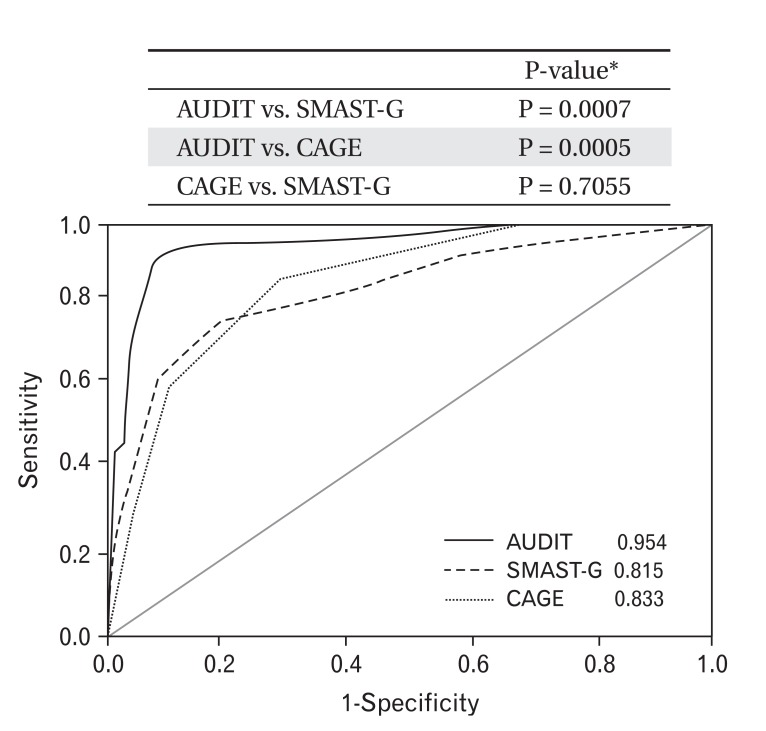
Area under the receiver operating characteristic curves (AUROCs) of screening instruments for identifying alcohol use disorder. AUDIT: Alcohol Use Disorder Identification Test, SMAST-G: Short Michigan Alcoholism Screening Test-geriatric version, CAGE: cut down, annoyed, guilty, eye-opener. *Statistical difference between AUROCs by comparison of paired receiver operating characteristic curves.
The optimal cut-off score of the AUDIT in screening for alcohol use disorders was 11 points (where the sum of sensitivity and specificity values was maximal) with sensitivity of 91.3%, specificity of 90.8%, positive predictive value of 70.0%, and negative predictive value of 97.8%. The optimal cut-off value of the SMAST-G in screening for alcohol use disorders was 4 points, with sensitivity of 73.9%, specificity of 76.5%, positive predictive value of 42.5%, and negative predictive value of 92.6%. The cutoff score of the CAGE in screening for alcohol-use disorders was 2 points, with sensitivity of 87.0%, specificity of 63.3%, positive predictive value of 35.7%, and negative predictive value of 95.4% (Table 3).
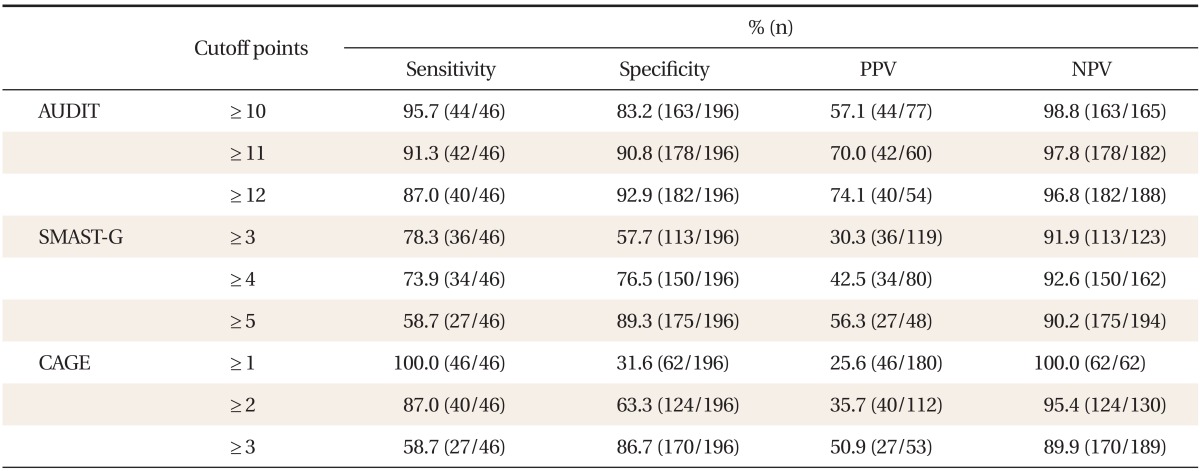
Cutoff points and performance of screening instruments for identifying alcohol use disorder.
DISCUSSION
It is important to identify patients with alcoholism in primary care settings so that they can receive proper treatment. However, it would be better to screen problem-drinking patients at earlier stages to foster prevention. As at-risk drinking in the form of continuous drinking rather than developed alcoholism is often found in elderly people, screening tools that effectively identify drinking problems are required.17) The present study chose the AUDIT, CAGE, and SMAST-G questionnaires as screening tools for at-risk drinking and alcohol use disorders and investigated each tool's AUROC and optimal cut-off score.
In the present study, the AUDIT showed the greatest AUROC value in screening for at-risk drinking in the elderly. This may be attributed to the fact that, in contrast to the SMAST-G and CAGE questionnaires, the AUDIT contains items assessing the frequency of drinking and the amount of alcohol consumed as a means of assessing heavy drinking or binge drinking. Based on the results of this study, the cut-off score for the AUDIT for screening at-risk drinking in males aged ≥ 65 years, was 7 points and higher. This score differs from 12 points, the cut-off point identified by Kim et al.12) and presented in their study on adult Korean males. The difference in cut-off scores likely reflects the drinking habits of elderly problem drinkers, who tend to consume a certain amount of alcohol on a continuing basis rather than engaging in occasional binge drinking.17) Additionally, the difference in cut-off scores may have been resulted from the modified AUDIT questions used in the current study. More specifically, due to the changes in the concentration of Soju, consuming a bottle of Soju was scored as 3 points (7 standard drinks) for AUDIT question number 2 in the previous study, whereas it was scored as 1 point (4 standard drinks) in the current study. Similarly, consuming a bottle of Soju (7 units in Soju cups) was considered to be binge drinking on question number 3 in the previous study but not in the current study, resulting in an overall decrease in respondents' drinking scores. Also, regarding the cut-off score of the AUDIT in screening for alcohol use disorders, the present study found 11 points to be an optimal cut-off score in elderly men. This was lower than the score of 15 points presented in the previous study12) based on adult males of all ages. This may be attributable to the same phenomenon as the cut-off score in screening for at-risk drinking. In short, it seems necessary to set lower cut-off scores on the AUDIT in elderly men than those used for the general adult male population.
The validity of the SMAST-G questionnaire has never been studied in Korea to the best of our knowledge. Regarding screening for alcohol use disorders in elderly men, the results of the present study fit well with those of the earlier study by Morton et al.,18) which reported that the SMAST-G exhibited 69.8% sensitivity, 80.5% specificity, and an AUROC of 0.84 based on 120 veterans aged ≥ 65 years. However, Morton et al.18) concluded that the SMAST-G was the best tool among the AUDIT, CAGE, and SMAST-G, based on their subjects. The present study, in contrast, found that the AUDIT was more useful than the SMAST-G. This difference may be partly due to items included in the DSM-IV criteria for alcohol abuse, such as repeated problems in social relationships and legal issues, which were not stressed in the DSM-III criteria. The cut-off score of 2 points for the SMAST-G for use in screening for at-risk drinking in elderly men in the current study is consistent with cut-off scores reported previously.15,19) Also, 4 points, identified as the optimal cut-off score for use in screening for alcohol use disorders in our study, is thought to be similar to 5 points presented by previous studies.20-22)
The CAGE questionnaire has a small number of items and is simple and easy to use in outpatient settings, although it proved less applicable to the elderly population in the current study. In this study, the CAGE questionnaire was found to have 60% sensitivity and 68% specificity in screening for at-risk drinking and 87% sensitivity and 63% specificity in screening for alcohol use disorders in this elderly population. A previous domestic study by Park et al.14) on the validity of the CAGE in adult male drinkers found 76.1% sensitivity and 90.0% specificity in screening for alcohol use disorders. Compared with the previous study, the sensitivity was higher and the specificity was lower in the present study, which seems attributable to demographic differences in the subjects. In the study by Park et al.,14) subjects aged ≥ 60 years accounted for 5% of the entire sample, whereas the present study dealt entirely with men aged ≥ 65 years only. The cut-off score of 2 points for the CAGE questionnaire in the current study as the reference score in screening for alcohol use disorders in elderly men fits well with the cut-off score suggested by Park et al.;14) however, this score is 1 point higher than that presented by Jones et al.23) This seems partly attributable to the fact that people in the East tend to hold more liberal viewpoints on drinking, especially drinking by elderly people, than do those in the West.
Some limitations of the present study should be addressed. First, the authors' efforts to include drinkers as subjects may have resulted in a bias toward heavy and binge drinkers. This may have led to the improper representation of general socio-demographic characteristics. Second, eight subjects (3.3%) were patients with alcohol abuse, and 38 subjects (15.7%) had alcohol dependence. Thus, fewer subjects abused alcohol than were alcohol dependent. In interpreting the results, it should be noted that the DSM-IVTR criteria for alcohol abuse that emphasizes "drinking even in cases of role-fulfillment disorder including absence and failure in duty and in physically dangerous situations such as drunken driving and operating machines" may not be applicable to elderly people, who are socially and occupationally less interactive. The fact that the subjects were elderly people (71.8 years old mean age) and 77.7% of the subjects were unemployed in this study also supports the above-mentioned points.
In conclusion, the present study investigated the utility of three alcohol-screening tools, the AUDIT, SMAST-G, and CAGE questionnaires, in screening for drinking problems in elderly men and found that the AUDIT proved the most useful in screening for at-risk drinking and alcohol-use disorders in elderly Korean men.
Notes
No potential conflict of interest relevant to this article was reported.