Effects of Having Usual Source of Care on Preventive Services and Chronic Disease Control: A Systematic Review
Article information
Abstract
Background
Having usual source of care has been associated with improved receipt of preventive services and control of chronic diseases (such as hypertension, diabetes, and hypercholesterolemia). The objective of this study was to examine whether having usual source of care is associated with improved receipt of preventive services and control of chronic diseases.
Methods
We searched MEDLINE, EMBASE, Cochrane, CINAHL, KMbase, KoreaMed, RiSS4U, National Assembly Library, and KISS for studies released through May 31st 2011. Two authors independently extracted the data. We manually searched the references and twenty recent related articles on PubMed. To assess the risk of bias RoBANS tool was used.
Results
We identified 10 studies. Most having usual source of care were associated with improved receipt of preventive services (cervical cancer screening, clinical breast exam, mammogram, prostate cancer screening, and flu shot) compared with no usual source of care. However, gastric cancer and colon cancer screening were difficult to conclude and blood pressure checkup showed mixed results. Overall there was no association between having usual source of care and smoking behaviors and the effect on chronic disease control was difficult to conclude.
Conclusion
Having usual source of care was associated with improved receipt of preventive services and overall the results were consistent. So, the results suggested that having usual source of care may help to receive preventive services. Hereafter, cohort studies are needed to evaluate casual relationships and more studies are needed in various countries and systems.
INTRODUCTION
Strengthening primary care has been one of the main agenda in family medicine as well as the entire medical profession for the past few decades. However, the lack of social consensus about the need for primary care has resulted in the diminishment of the status of primary care. One of the biggest causes of this lack of support for strengthening primary care is that healthcare experts have failed to provide convincing evidence that primary care is effective in achieving a substantial improvement of the overall level of health of the population In this regard, efforts are needed to create a foundation of primary care as well as improvement in the desirable characteristics of primary care, such as continuity of care, comprehensiveness, and access to usual sources of care, which help to improve medical results.
A usual source of care is a place where a person usually goes when he is sick, such as a physician's office or health center.1-3) Usual sources of care are associated with continuity of care which is one of the important factors influencing the quality of medical care.4) If there is no usual source of care, the continuity of care can be inhibited and can act as a significant obstacle to receiving high quality care.5) In a study of foreign countries, it has been shown that the provision of usual sources of care, increases accessibility to health care,6) increases satisfaction with health care,7) and reduces the frequency of emergency room visits.8,9) In addition, it was discovered that having a usual source of care increased the use of preventive services2,5) and had a large impact on the management of chronic diseases, such as hypertension, diabetes, and hyperlipidemia.10)
On the other hand, there are other studies with different results and there was no systematic review or meta-analysis of studies indicating that usual sources of care have an impact on disease prevention and management of chronic diseases. Therefore, the purpose of this study is to conduct a systematic review of the impact of the access to usual sources of care on prevention of disease and management of chronic diseases, such as hypertension and diabetes.
METHODS
A systematic review was conducted to investigate the impact of access to usual sources of care on prevention of disease and management of chronic diseases, such as hypertension, diabetes, etc.
1. Inclusion Criteria
1) Types of studies
Clinical trials, observational studies (cohort studies, case-control studies, and cross-sectional studies) were included. Studies without control groups were excluded.
2) Patients
This review included adults (20 years of age or older) regardless of age, sex, or status of health.
3) Intervention and comparison
We included studies compared between subjects having a usual source of care and those not having a usual source of care.
4) Outcomes
The included trials measured the impacts of usual sources of care on prevention of disease and management of chronic diseases, such as hypertension, diabetes, etc. However, studies that compared the results of the use of resources, such as the frequency of emergency room visits, hospitalization rates, and dental care, were excluded from the study.
2. Search Method
The last search was performed on May 31, 2011. All searches were made by professional librarians and search terms were selected in consultation between the authors and professional librarians. There were no language restrictions.
Foreign literature databases searched include: MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, and CINAHL. Our search was updated to May 2011. Domestic databases searched include: KoreaMed, KMbase, RISS4U, Library of Congress, and KISS. Our search was updated to May 2011.
The following search terms were used for the foreign material and KoreaMed searches:
"usual source of care" OR ("regular source" AND care) OR "regular doctor" OR "regular site"
The data search term for domestic databases except KoreaMed was the Korean translation of "usual source of care". For health service research, a search with such search terms is likely to be incomplete. In order to compensate for this, reference search of included studies was conducted and the search was expanded by using the 'related articles' menu of PubMed.
3. Study Selection
Two independent authors reviewed the results of the searches and the studies that met the criteria for inclusion were selected. In the case of disagreement, decision was made by discussion and consensus. If consensus was not possible, a final decision was made by the third author.
4. Assessment of Risk of Bias
Two independent authors assessed risk of bias using the RoBANS tool11,12) in order to evaluate the method quality of the selected studies. Each criteria was assessed as one of: yes, no, and unclear, with 'yes' indicating a low risk of bias, 'no' indicating a high risk of bias, and 'unclear' indicating a lack of information. The evaluation was done by two independent authors, and discrepancies were resolved by discussion and consensus.
5. Data Extraction
Relevant data, such as the study design, subject and characteristics, the definition of usual source of care, and outcome variables were abstracted independently by two review authors. Discrepancies were resolved by discussion and consensus.
RESULTS
Seventy hundred and fifty-seven abstracts out of 1,715 records identified through database search were examined, not counting 958 abstracts appearing twice. Fourteen studies were screened. After assessing full text articles for eligibility, ten studies (Spatz,13) Winters,10) Blewett,14) Kim,2) Rhee,15) Doescher,16) Mendoza-Sassi,17) Ahluwalia,18) Kiefe,19) and Ettner20)) were selected and included in the analysis. We excluded two studies which did not provide the appropriate data, another two studies which compared usual sources of medical institutions and usual sources doctors (Figure 1).

Flow sheet of study selection.
A total of 128,559 participants were included: 92,646 participants were in the group having a usual source of care and 35,913 were in the group not having a usual source of care. Nine were cross-sectional studies and 1 was a cohort study. Eight of the selected studies were conducted in the US, one in Korea, and one in Brazil. The selected studies were published between 1996 and 2010 (Table 1).

Characteristics of included studies.
The survey items for determining access to a usual source of care in all studies were, "where can you get counseling or therapy, or see a doctor when you are sick?" or "if so, where (or who)?" The choices available were: university hospital, doctor's office, clinic, health center, health clinic, emergency room, and other. However, there were differences between the studies in questions about the category of usual sources of care. Questions were asked about medical institutions in seven studies,2,10,13,15,18-20) and doctors in one study.17) In two studies, questions were asked about doctors after questions asking about medical institutions.14,16)
The risk of bias for the included studies was evaluated by using the RoBANS tool11,12) for assessing the risk of bias. Six studies were assessed to be well conducted and four studies were evaluated as unclear. Eight studies were evaluated as appropriate for consideration with respect to confounding variables and two studies were evaluated as unclear. Seven studies were assessed as inadequate with respect to appropriate intervention measures and three studies were evaluated as unclear. Blinding of outcome was adequately described for all studies. Incomplete outcome data and selective results reporting were adequately addressed in five studies and were evaluated as unclear in five studies. The overall research quality was relatively high (Figure 2).
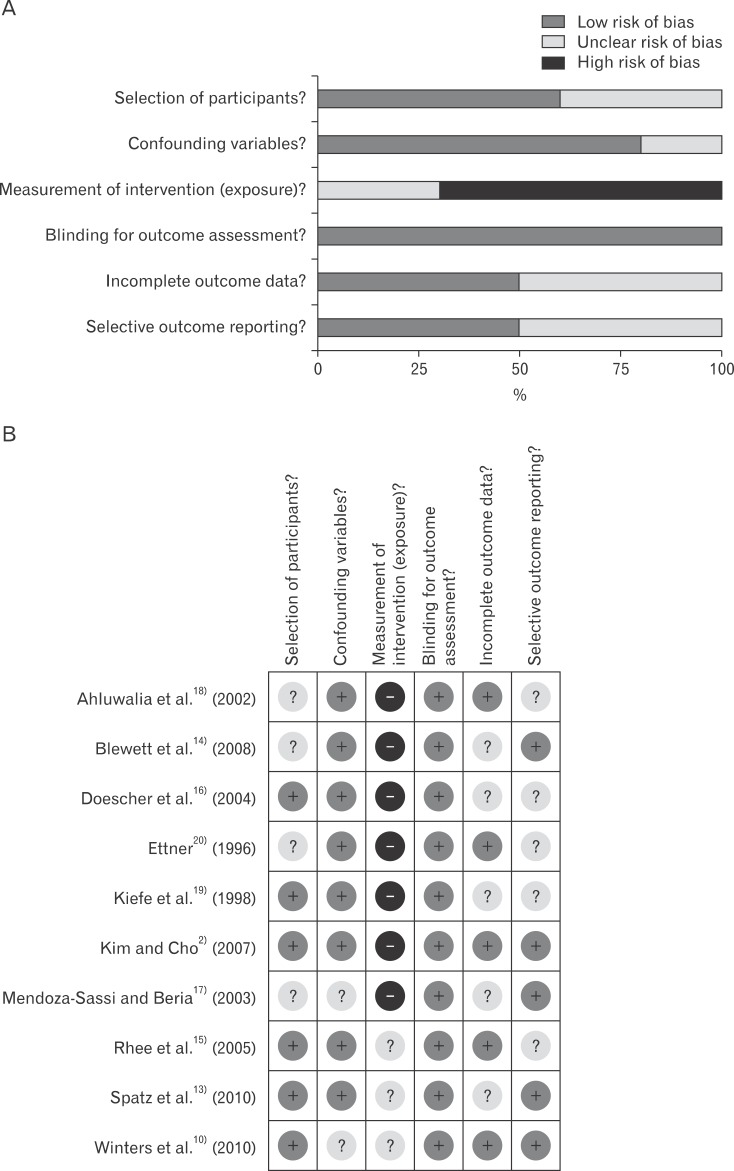
Risk of bias. (A) Risk of bias graph. (B) Risk of bias summary.
Seven studies measured the percentage of preventive services used according to groups. Studied preventive services were gastric cancer screening, colorectal cancer screening, cervical cancer screening, clinical breast examinations, prostate cancer screening, mammography, blood pressure measurement, influenza vaccination, and programs for quitting smoking, including success rate, and starting smoking rate. There was one study measuring the percentage of hypertension treatment, two studies measuring the percentage of hyperlipidemia treatment, one study measuring the percentage of hypertension control, and two studies measuring the percentage of diabetes control.
The effects of having a usual source of care for cancer screening with the exception of gastric cancer and colorectal cancer are shown in Table 2. All of the studies covering cervical cancer screening, clinical breast examination and prostate cancer screening tests, reported that people having a usual source of care are more likely to be tested than those not having it.2,14,16,17,20) People having a usual source of care were more likely to receive mammograms in four studies.2,14,16,20) In one study, there was no statistically significant difference.17) Gastric cancer screening and colorectal cancer screening were reported only in one study. More people having a usual source of care underwent gastric cancer screening and colorectal cancer screening than those without having a usual source of care, but only the gastric cancer screening difference was statistically significant.2) More people had blood pressure tested when having a usual source of care in one study,2) but in another study, blood pressure measurements and having a usual source of care were not related.20) In two studies, more people received the influenza vaccine when they had a usual source of care,14,16) while trying to stop smoking, success rate of quitting smoking, and the rate of starting to smoke were not associated with having a usual source of care (Table 3). There were not many studies examining the impact of having a usual source of care on the management of chronic diseases. For the treatment of hypertension and hyperlipidemia, people having a usual source of care received better treatment than those not having a usual source of care.10,13) Hypertension control was reported only in one study and there was no relationship between hypertension control and having a usual source of care.2) In addition, in one study, having a usual source of care contributed to better adjustment of diabetes control,15) but in another study, there was no relationship between diabetes control and having a usual source of care (Table 4).2)
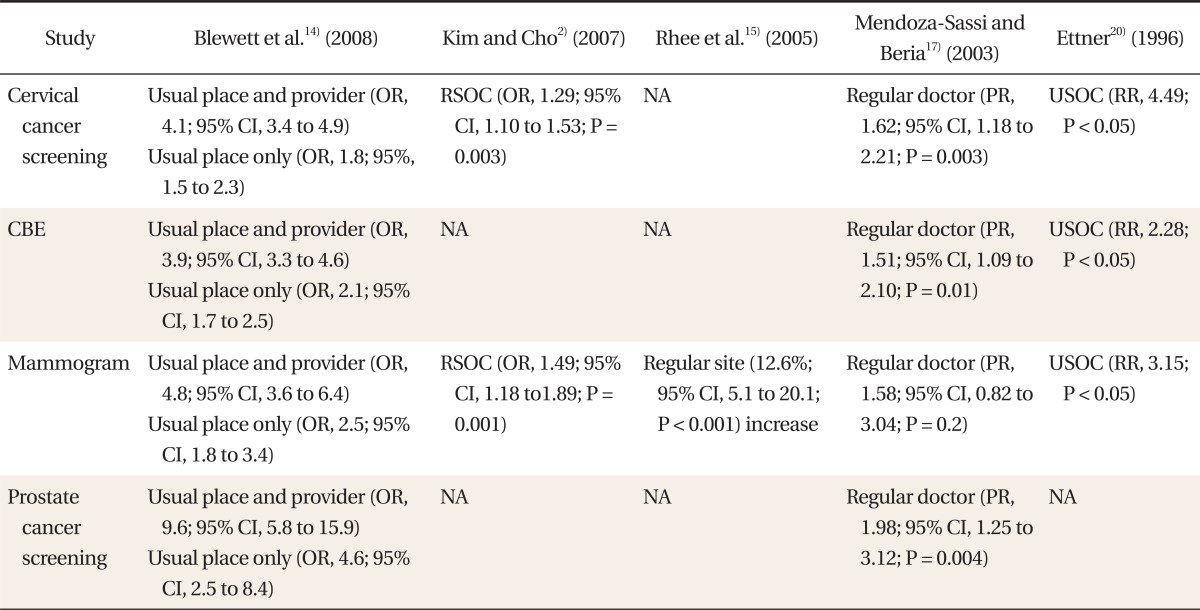
USOC effect in the receipt of preventive services (cancer screening except gastric and colon cancer).*
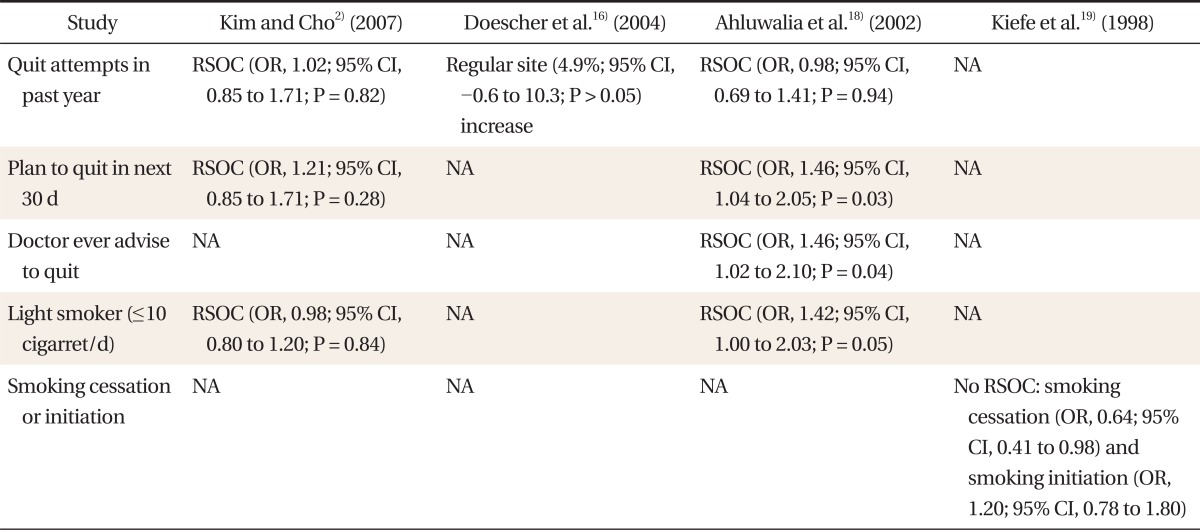
Usual source of care effect in the receipt of preventive services (smoking cessation-related predictors, smoking cessation, and initiation).*

USOC effect in the treatment and control of chronic disease.*
DISCUSSION
The purpose of this study is to conduct a systematic review of literature relating access to usual sources of care to prevention of disease and management of chronic diseases, such as hypertension, diabetes, etc.
In this systematic review, seven studies2,14,16-20) showed people who have access to a usual source of care received more preventive services than those without. This is presumably because people who have a usual source of care may have a chance to receive preventive health counseling. Patients who had access to a usual source of care received more preventative services, such as cervical cancer screening, prostate cancer screening, clinical breast examination and influenza vaccines. Four studies2,14,15,20) covering breast cancer screening reported that people having a usual source of care are more likely to receive a mamography than those not having it. Only one study2) reported on gastric cancer screening and colorectal cancer screening. In that study, people who had access to a usual source of care received more gastric cancer screening and colorectal cancer screening. However, having a usual source of care made a statistically significant difference only in the case of gastric cancer screening. Having a usual source of care made no statistically significant difference in colorectal cancer screening because since the screening interval of sigmoidoscopy or colonoscopy is at least five years, it would be difficult to determine the effectiveness with questions about the recent 2 years of experience. There was no consistent result concerning blood pressure measurement. More blood pressure measurements were made for those having a usual source of care in one study,2) but in another study,20) blood pressure measurements and having a usual source of care were not related, which might be due to the fact that blood pressure measurements become routine practice.
The reason why quitting-smoking-success rate and starting-smoking rate were not related with having a usual source of care is not clear. It may be due to the small size of the sample, or usual practice pattern. Since there was not enough research, it was difficult to draw any conclusion whether usual sources of care have an impact on management of chronic diseases or not. The reason behind this might be that chronic disease management actually has a high association with continuity of care, but studies on the continuity of care do not usually examine access to usual sources of care as an indicator of continuity of care.
The limitations of this study are: first, 9 out of the total 10 studies are cross-sectional studies. Thus, an exact causal relationship could not be confirmed between usual sources of care and prevention of disease. Second, the terms for usual source of care are not unified and an official search term was not yet set, which could lead to missing studies appropriate to the topic in the process of searching studies. For that reason, the references in each study were examined and we made an effort not to miss any appropriate study by performing additional searches using the "related-article" option in PubMed. Third, in all studies, the odds ratio was presented to compare the group having a usual source of care and the group not having a usual source of care. But the number of each usual source of care in preventive services was not listed. We tried to obtain the data from the original author, but no response has been received. Thus, we could not perform a meta-analysis. Fourth, the differences in every study about the proportion of access to usual sources of care in different countries (US, 79%; Brazil, 37%; Korea, 30%) may cause a risk of bias. However, since the results in different studies were similar, there is no problem of interpretation. Fifth, the studies have been performed only in three countries: South Korea, US, and Brazil. Each country's health care system has different characteristics such as method of payment, type of health care system, health insurance, etc., but differences in the size of the effect of access to usual sources of care are not significant. Effects of the type of health care system on access to usual sources of care are not likely to occur.
In conclusion, more preventive services were received by those with a usual source of care in general and the results support that. Therefore, it may helpful to have a usual source of care for the prevention and early detection of disease. In this regard, institutional and administrative support is needed in order to increase the percentage of Koreans having a usual source of care and it may be necessary to make efforts to associate access to usual sources of care with the management of the chronic diseases.
In addition, additional further research is needed to see how the family doctor system has an effect on providing a usual source of care. Furthermore, a study on barriers in securing a usual source of care is needed. Also, cohort studies are needed in order to be able to explain the causal relationships and more research is necessary on how helpful it is to have a usual source of care in various institutions and in various countries.
Notes
No potential conflict of interest relevant to this article was reported.