INTRODUCTION
One-third of the world's population is currently infected with tuberculosis (TB), and there are more than 8 million new TB cases worldwide each year.1) In terms of the morbidity and mortality of TB, Korea tops the Organization for Economic Cooperation and Development member countries. In 2010, there were 48,101 (98.4/105) new TB patients in Korea.2,3) According to data from Statistics Korea, 2,292 (4.6/105) Koreans died from TB in 2009, and pulmonary TB remains the tenth leading cause of death among Korean males in their 20s and 80s.4) TB in Korea still accounts for massive socio-economic spending, with an estimated 820 billion won spent to treat it yearly.2)
Due to the establishment of the national TB control program in 1962, the development of effective anti-TB drugs, and the introduction of standard TB treatment regimens, the prevalence rate of active pulmonary TB (revealed on the chest X-ray) fell from 5.1% in 1965 to 1.0% in 1995, and the number of sputum smear examination results positive for acid-fast bacilli decreased from 0.69% in 1965 to 0.09% in 1995, and by nearly 5% yearly.5) Since 2000, however, the decline in the number of new TB cases has slowed; and recently, the number of multidrug-resistant TB (MDR-TB) cases has risen and there have been massive TB outbreaks in schools.2)
Europe and the US, where TB prevalence is low, invest substantial social efforts into the early diagnosis and treatment of TB in vulnerable populations such as homeless people, alcoholics, people who abuse substances, migrants, and prisoners. In contrast, Korean society, which generally has a high TB rate, has had insufficient studies on TB among the homeless or vulnerable groups and little knowledge on early TB diagnosis and treatment. A marked increase in the number of homeless people in Korea has been reported since the financial crisis in the late 1990s, with an estimated 4,664 homeless people nationwide in 2009 (with 3,404 living in homeless shelters and 1,260 living outside or in subway stations) and 550 in Busan.6)
Homeless persons have a higher risk of developing TB when they are exposed to Mycobacterium tuberculosis (M. tuberculosis) due to their malnutrition, unstable living circumstances, and poverty. In particular, as they typically live in crowded areas such as railroad stations and subway stations or tend to live in homeless shelters or flophouses that are packed with people, they are more likely to develop active TB and become the source of infection, which will put the public health at risk. According to a recent study that took chest X-rays of homeless people in Seoul between October 2009 and March 2010, the prevalence rate of active TB among the homeless was 5.8%, 23 times higher than the 0.25% estimated TB rate of the general population in 2008.7)
This study was conducted to identify the status of homeless TB patients in Korea and to promote national TB control using factors of TB treatment success by evaluating the characteristics of the homeless with TB who had been admitted between January 2001 and December 2010 to Busan Medical Center.
METHODS
1. Study Population
Of the 2,073 patients who were registered as TB patients in the Korean TB surveillance program of Busan Medical Center between January 2001 and December 2010, the medical records of 158 homeless individuals who were living in homeless shelters, homeless drop-in centers, or health facilities, or were classified as homeless patients by the Medical Care Act, were examined. Of these, the study population consisted of 142 subjects after the exclusion of six with extrapulmonary TB, two who were foreigners, three whose treatment had not been completed, and five with insufficient medical records.
2. Data Collection
From the medical records at the time of the TB diagnosis, the age, gender, smoking history, history of previous TB treatment, length of hospital stay, drug susceptibility test (DST), location before the hospital admission, and type of residence at the time of the hospital visit were examined. The morbidity of underlying diseases with risk factors (diabetes, chronic kidney disease, malignancy, liver cirrhosis, alcoholism, chronic obstructive pulmonary disease [COPD], and human immunodeficiency virus [HIV] infection) that promote TB development by inhibiting the immune mechanism was detected from the medical records, and malnutrition was diagnosed when the albumin level was Ōēż3.0 g/dL from the blood test conducted at the time of the first visit.8) Cavities were detected from the chest X-ray at the first visit, and the treatment outcomes were assessed from the medical records and admission notes.
3. Definitions
Definitions are as follows. 1) New case: a patient who had never undergone TB treatment or who had taken anti-TB drugs for less than 1 month, including those transferred in as new cases from other medical institutions. 2) Treatment after failure: a patient who remain sputum smear-positive at month 5 of treatment or culture-positive at month 4 during treatment, and who needs a new prescription to initiate re-treatment. 3) Relapse: a patient who had successfully completed TB treatment but whose TB had relapsed and who meets the criteria for TB diagnosis. 4) Treatment after default: a patient whose TB treatment had been interrupted for two months or more after completion of at least one month of treatment. 5) Transferredout: a patient who had been treated for more than a month and whose treatment had not been discontinued for more than two months, but who had been transferred to a different healthcare facility.9-11)
The treatment outcomes are defined as follows. 1) Cured: a patient who is smear-negative after the treatment completion (in the last month of the treatment) and on at least one previous occasion. 2) Treatment failure: a smear-positive patient after four months of treatment or whose DST shows multidrugresistant TB. 3) Died: a patient who died for any reason during the course of the TB treatment. 4) Treatment default: a patient whose treatment was interrupted before the completion of the pre-arranged treatment by the doctor, including one who was lost during the follow-up after his/her discharge or who escaped from the hospital. 5) Transferred-out: a patient who had been transferred to another medical facility and whose treatment outcome was not known.9-11)
MDR-TB is defined as TB that is resistant to both isoniazid (INH) and rifampin (RFP),12-14) and extensively drug-resistant TB (XDR-TB) is defined as a situation in which there is resistance to INH, RFP, any of the fluoroquinolones, and one or more injectible drugs (capreomycin, amikacin, or kanamycin).15-17)
4. Factors of Treatment Success
Except for those who were transferred out, the cured patients were assigned to the successfully treated group, and those who failed, died, or defaulted were assigned to the incompletely treated group. The age, sex ratio, and type of residence at the time of admission, drug resistance in the DST, a history of TB treatment, cavities in the chest X-ray, a smoking history, and the incidence of underlying diseases in both groups were compared, statistically significant differences were assessed, and independent factors of treatment success were evaluated by analyzing the variables that showed significant differences.
5. Microbiological Examination
The Ziehl-Neelson method and the direct fluorescent technique were used for the sputum smear microscopy. For the sputum culture, the sputum specimens were inoculated onto an Ogawa medium and then inspected in the hospital laboratory for 8 weeks to check the appearance of colonies. The drug susceptibility tests were performed at the Green Cross Reference Laboratory using the absolute concentration method.
6. Statistical Methods
The mean ┬▒ SD was presented for the continuous variables, and the frequency and ratio for the categorical variables. Chi-square tests were used for the sex ratio, smoking history, type of residence, location before admission, history of TB treatment, and drug resistance between the successfully treated group and the incompletely treated group; a Student t-test, for the age and the length of stay (LOS); and a Fisher's exact test, for incidence of underlying disease and cavities on chest X-ray. A multiple logistic regression model that can predict the treatment success using significantly correlated variables was set up. The statistical analysis was conducted using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA), and the statistical significance was set at P < 0.05.
RESULTS
1. Demographic Characteristics
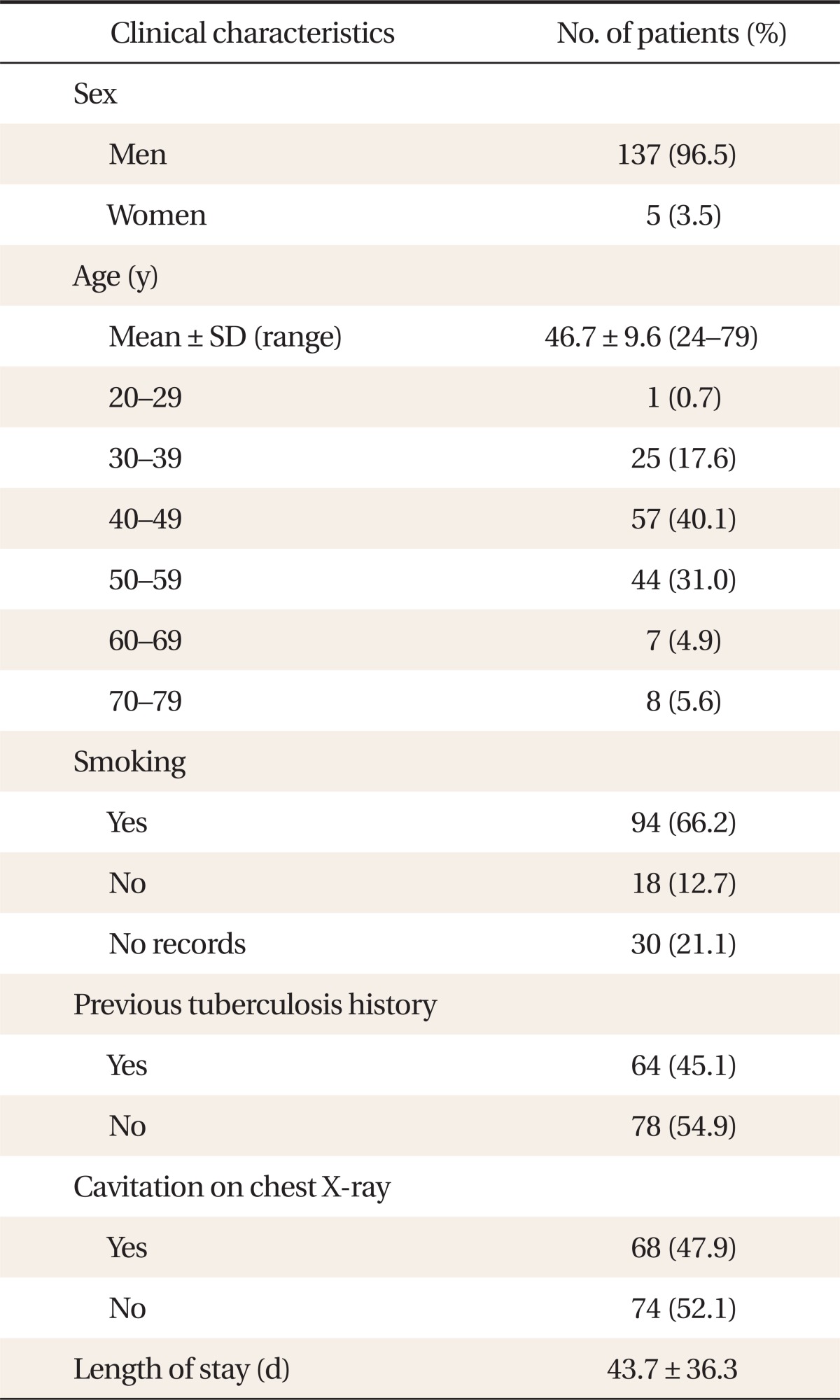
Of the 142 recruited patients, 137 (96.5%) were male and five (3.5%) were female, and their mean age was 46.7 ┬▒ 9.6 years (range, 24 to 79 years). Fifty-seven (40.1%) patients in their 40s constituted the majority, followed by 44 patients (31%) in their 50s. Excluding 30 patients whose smoking history was unknown from their medical records, 94 (66.2%) had smoked before and 18 (12.7%) had not. Sixty-four (45%) patients had a history of TB treatment, of whom 19 (13.4%) were declared to have been cured but had a relapse and 34 (24.0%) had arbitrarily interrupted treatments. Sixty-eight (47.9%) had cavities on their chest X-ray, and the mean length of their hospital stay was 43.7 ┬▒ 36.3 days (Table 1).
2. Risk Factors and Underlying Diseases
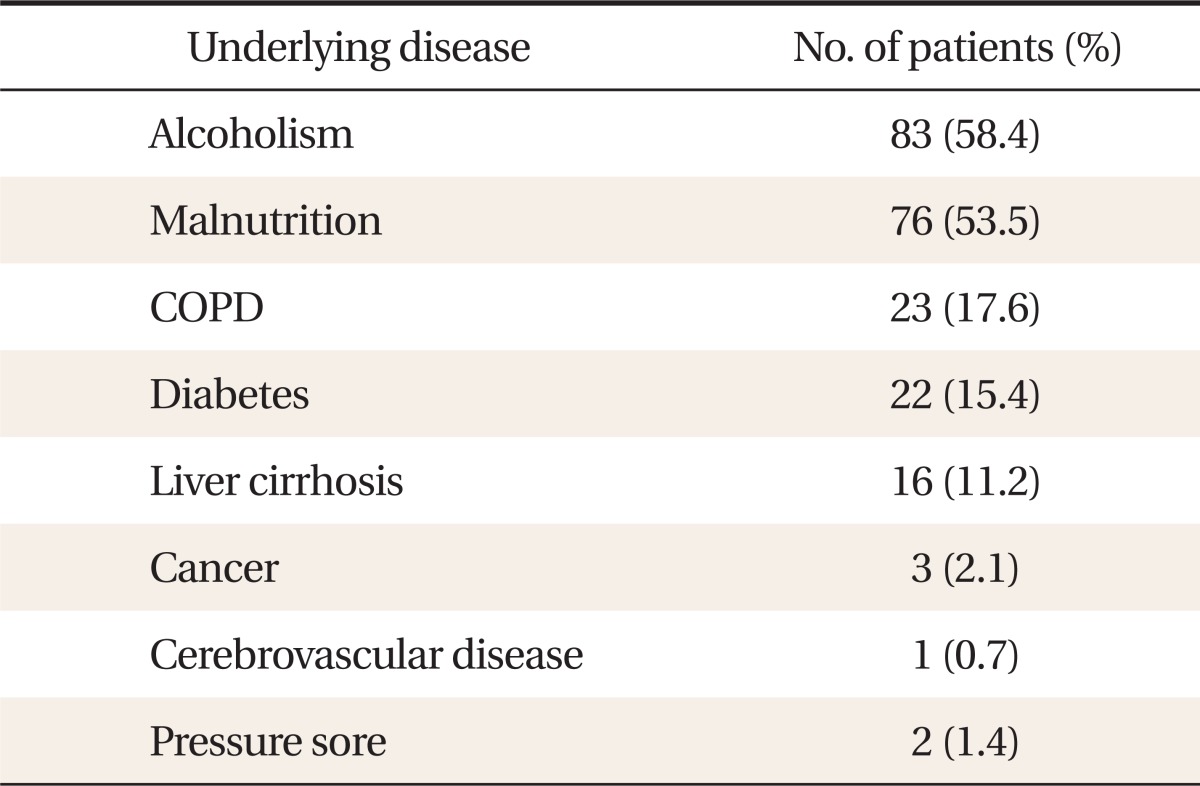
The morbidity of the underlying diseases (diabetes, chronic renal failure, malignancy, liver cirrhosis, alcohol dependence, COPD, HIV infection, and malnutrition) that posed a high risk of active TB development after exposure to M. tuberculosis was detected from the medical records, and 89 (62.7%) of all the 142 patients developed one or more diseases, including 83 (58.4%) with alcohol dependence and 76 (53.5%) with malnutrition. The underlying diseases included COPD in 23 (17.6%) patients, diabetes in 22 (15.4%), liver cirrhosis in 16 (11.2%), malignancy in 3 (2.1%), pressure sore in 2 (1.4%), and cerebrovascular disease in 1 (0.7%) (Table 2). In addition, three patients had late syphilis; 13, chronic hepatitis B; nine, hepatitis C; 16, schizophrenia; 24, pancreatitis; 24, peptic ulcer; and 12, hypertension.
3. Type of Residence and Location before Hospital Admission
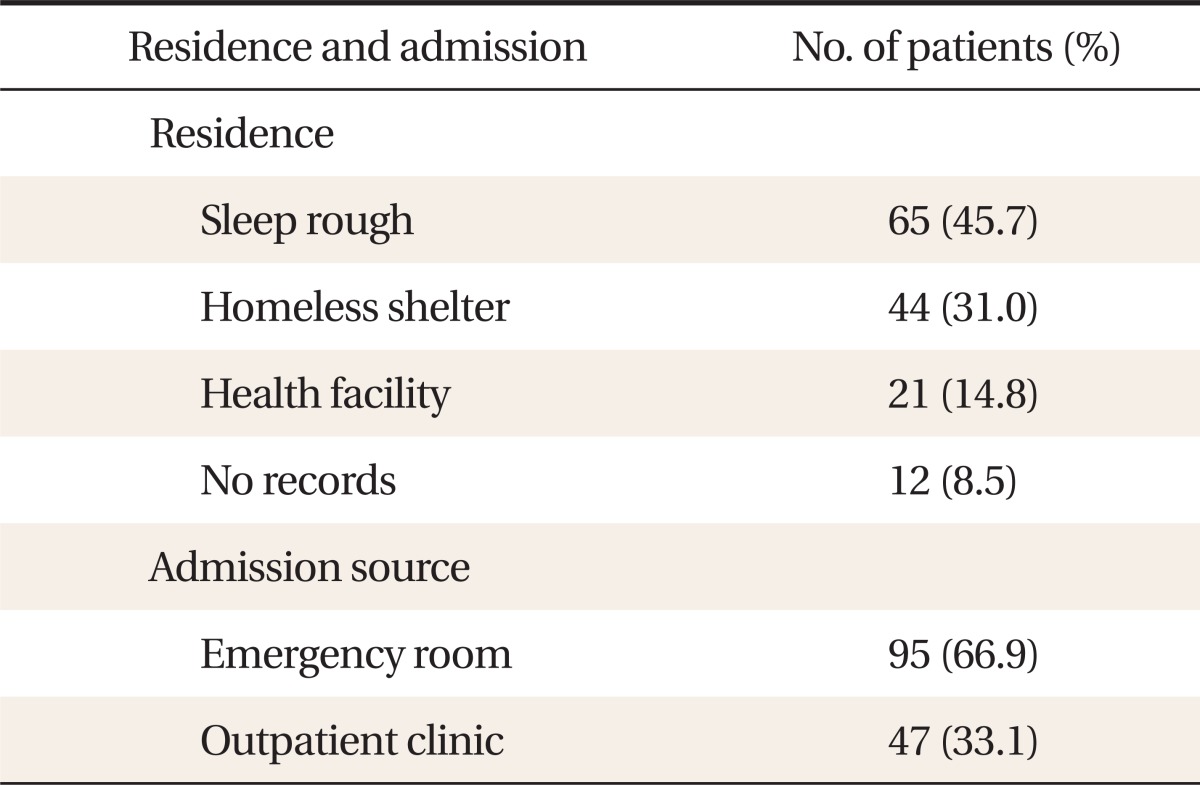
At the time of the patients' admission, 65 of them (45.7%)-the majority-on the streets; 44 (31%) in homeless shelters; and 21 (14.8%) in health facilities. Twelve patients (8.5%) had no records. Ninety-five (66.9%) were admitted through the emergency room, and most were homeless patients whose identities were unknown and who visited the hospital with the help of the police and the 119 rescue service. Forty-seven patients (33.1%) were admitted after an outpatient visit, and most were required to be isolated and treated after they were suspected of TB infection at free clinics for the homeless, subway clinics of the Korean National Tuberculosis Association, or public health centers (Table 3).
4. Drug Susceptibility Test
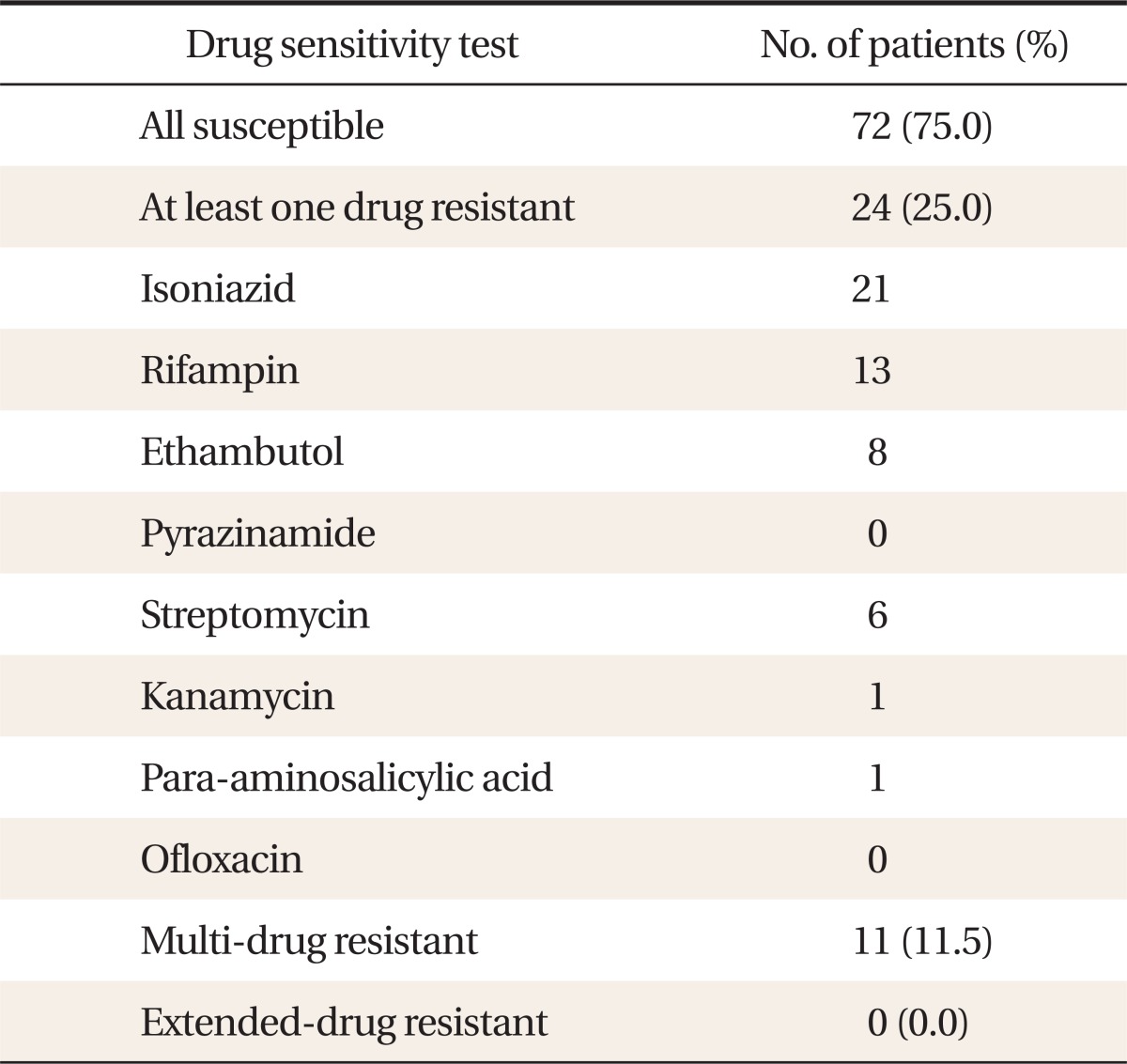
A DST was conducted among 96 (67.6%) smear-positive patients, whereas 46 (32.4%) did not undergo DST or their test outcomes were unknown. Seventy-two patients (75%) were resistant to all anti-TB drugs, and 24 (25%) were resistant to one or more drugs, including eight to isoniazid and two to rifampin. One patient who was resistant to the most drugs was resistant to five drugs, and there were 11 cases of MDR-TB (11.5%) but none of XDR-TB (Table 4).
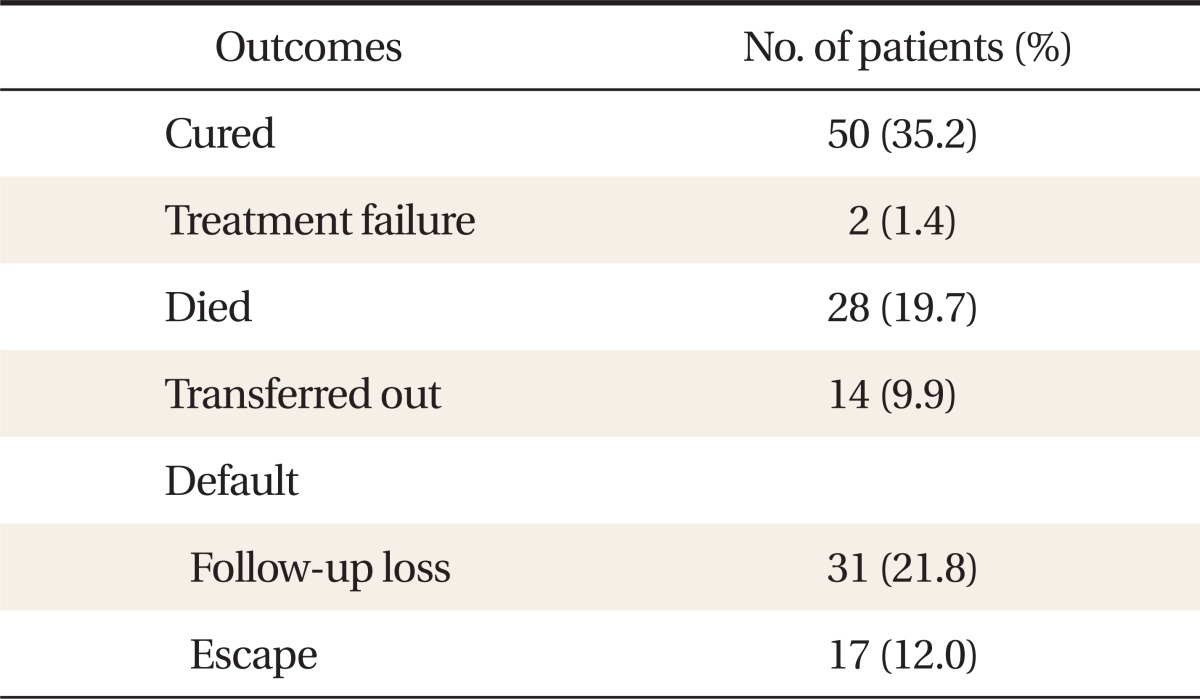
5. Treatment Outcomes
Fifty patients (35.2%) were declared cured after they emerged smear-negative following the completion of their treatment through regular visits to a doctor subsequent to their discharge. Fourteen patients (9.9%) were transferred to another medical facility and their treatment outcomes were unknown; two (1.4%) experienced treatment failure; 28 (19.7%) died; and 48 (33.8%) defaulted, including 31 (21.8%) who were lost during the follow-up after their discharge and 17 (12%) whose treatment was interrupted arbitrarily and who escaped from the hospital (Table 5).
6. Comparison of the Treatment Success Group and the Incomplete Treatment Group and Independent Factors of Treatment Success
Except for the transferred-out patients, the cured patients were assigned to the successfully treated group, and those who failed, died, or defaulted, to the incompletely treated group. The male/female ratio, age, smoking history, type of residence, location before admission, diseases with risk factors, history of TB treatment, anti-TB drug resistance in the DST, a cavity on the chest X-ray, and LOS were examined and compared between the groups. The type of residence at the time of the hospital visit (P < 0.001), diseases with risk factors (P = 0.003), and history of TB treatment (P = 0.009) showed significant differences between the two groups.
In the successfully treated group, 13 patients (27.7%) lived on the streets and 26 (55.3%), in shelters. In the incompletely treated group, 47 patients (67.1%) lived on the streets and only 19 (27.1%), in shelters (P < 0.001). Twenty-six patients (52.0%) in the successfully treated group and 61 (78.2%) in the incompletely treated group developed underlying diseases with risk factors of TB (P = 0.003). Fourteen patients (28.0%) in the successfully treated group and 40 (51.3%) in the incompletely treated group had a history of TB treatment (P = 0.009) (Table 6).
A multiple logistic regression analysis was performed on significant variables by independently evaluating the risk factors of treatment failure. Though a history of TB treatment did not influence the treatment failure, people who lived on the streets had a 4.77 times higher risk of treatment failure than those who lived in facilities such as homeless shelters or rehabilitation centers (95% confidence interval [CI], 2.05 to 11.10; P < 0.001), and patients who developed diseases with risk factors had 2.72 times higher risks of treatment failure than those who did not (95% CI, 1.13 to 6.53; P = 0.025) (Table 7).
DISCUSSION
Even with the higher TB incidence and prevalence rate of the homeless compared to those of the general population, elements of their lifestyle, such as alcohol abuse or unstable living conditions, made it difficult for them to persist with the treatment.
According to the tuberculosis statistics of World Health Organization for the 30 richest countries, the treatment success rate for new smear-positive TB cases in Korea was 84%; according to public health centers, 79% in 2010;2) and in this study, 35.2%. If the factors of TB treatment success are predictable, they will help control the rise in the number of TB patients by improving their treatment compliance. Some studies on the risk factors that lower the treatment compliance of TB patients showed no significant differences in the clinical manifestations (e.g., age, gender, adverse events of anti-TB drugs, pulmonary symptom, and smear-positive TB) of pulmonary and extrapulmonary TB,18) and in underlying diseases.19)
This study independently evaluated the risk factors of treatment failure by comparing the clinical characteristics of homeless TB patients in the successfully treated group and the incompletely treated group.
In the successfully treated group, there were more patients who lived in facilities (55.3%) such as shelters than those who lived on the streets (27.7%); whereas in the incompletely treated group, there were more street homeless patients (67.1%) (P < 0.001) and the treatment failure rate was 4.77 times higher (95% CI, 2.05 to 11.10; P < 0.001) than that for those who lived in homeless shelters and facilities. TB patients are required to complete their treatment by visiting a clinic regularly and taking anti-TB drugs. As the homeless who lived normal lives in shelters and facilities showed higher compliance to the treatment than the street homeless,17) stable housing and socio-economic support for homeless patients are deemed to be key factors of treatment success.
Of the patients in the successfully treated group, 48% developed diseases with risk factors; whereas in the incompletely treated group, 78.2% did (P = 0.003), and the treatment failure rate was 2.72 times higher (95% CI, 1.13 to 6.53; P = 0.025). Of all the 142 patients, 89 developed underlying diseases with risk factors. In many studies, a low albumin level was the independent risk factor that was associated with the death of a TB patient;20,21) and in this study, more than half of the subjects had a poor nutritional status, with a low albumin level and anemia, including 83 with alcohol dependence and 16 with liver cirrhosis. These became risk factors of TB by increasing the frequency of adverse events of anti-TB drugs, delaying the use of anti-TB drugs, and finally lowering the TB treatment success rate. Most homeless people have a low level of awareness of health management and lack regular access to medical checkups. Through regular checkups, early diagnosis and treatment of TB among the homeless who are at high risk of infection should reduce public spending on TB treatment.
A history of TB treatment is not a risk factor of treatment failure, though the percentage of the patients with such history in the incompletely treated group (51.3%) was significantly higher than that in the successfully treated group (28%) (P = 0.009). A study by Park19) reported that the high treatment default rate led to the low treatment success rate; in this study, 33.8% of the patients did not adhere to the treatment after their discharge or experienced treatment interruption after they escaped from the hospital. In particular, of the 40 patients with a history of TB treatment in the incompletely treated group, 30 had an interruption in their taking of anti-TB drugs, 20 had two or more interruptions, and five, three or more. It has been reported that the TB treatment success rate significantly increased to 69.9% and 85.4% since the implementation of the public-private mix for TB care and control in 2009.19) The socio-economic characteristics of the homeless make it difficult to control them, compared to those of general patients, whereas comprehensive care by TB nurses or medical staff will raise the effectiveness of TB treatment through education and counseling for the promotion of adherence to the treatment after discharge.
In this study, no significant difference in drug resistance between the successfully treated group and the incompletely treated group was seen, but 25% of the study population was resistant to one or more drugs and 11.5% was multidrug-resistant. These figures are higher than the drug resistance rate (14.9%) and the multidrug resistance rate (4.9%) of public health centers, and the drug resistance rate (19.8%) and the multidrug resistance rate (9.5%) of the private health sector based on the data released by Centers for Disease Control and Prevention.22) The default rate of the homeless in this study was high and may lead to a high treatment failure rate. As a result, there may be a rise in acquired resistance, which occurs due to inappropriate regimens or use of drugs, and it may be followed by primary resistance. To prevent the spread of drug-resistant TB to the general population, active surveillance of high-risk populations is very important, and particularly, the drug resistance rate of the homeless who have a high risk of TB should be identified, followed by proper TB control.
This study assessed the clinical characteristics of 142 homeless patients with pulmonary TB at Busan Medical Center, which provide public health services in the Busan region, and evaluated the independent risk factors of the treatment success of homeless TB patients by comparing the successfully treated group and the incompletely treated group. This study had an insufficient sample size (142 patients), however, and the clinical characteristics of the subjects were based merely on their medical records.
Due to the poor nutritional status, unstable living circumstances, and crowded living conditions of homeless people, they have a higher risk of developing TB than the general population once they are exposed to M. tuberculosis, and of becoming active sources of TB infection. Therefore, identifying the current status of homeless TB patients, followed by their early treatment and successful treatment, is very important in lowering the prevalence of TB in Korea. Moreover, more extensive studies on homeless TB patients are needed.