Utility of the Alcohol Consumption Questions in the Alcohol Use Disorders Identification Test for Screening At-Risk Drinking and Alcohol Use Disorders among Korean College Students
Article information
Abstract
Background
This study evaluated the utility of the Alcohol Use Disorders Identification Test Alcohol Consumption Questions (AUDIT-C) in screening at-risk drinking and alcohol use disorders among Korean college students.
Methods
For the 387 students who visited Chungnam National University student health center, drinking state and alcohol use disorders were assessed through diagnostic interviews. In addition, Alcohol Use Disorders Identification Test (AUDIT), AUDIT-C, and cut down, annoyed, guilty, eye-opener (CAGE) were applied. The utility of the questionnaires for the interview results were compared.
Results
The areas under the receiver operating characteristic curves (AUROCs) of AUDIT-C for screening at-risk drinking were 0.927 in the male and 0.921 in the female participants. The AUROCs of AUDIT and CAGE were 0.906 and 0.643, respectively, in the male, and 0.898 and 0.657, respectively, in the female participants. The optimal screening scores of at-risk drinking in AUDIT-C were ≥6 in the male and ≥4 in the female participants; and in AUDIT and CAGE, ≥8 and ≥1, respectively, in the male, and ≥5 and ≥1 in the female participants. The AUROCs of AUDIT-C in screening alcohol use disorders were 0.902 in the male and 0.939 in the female participants. In the AUDIT and CAGE, the AUROCs were 0.936 and 0.712, respectively, in the male, and 0.960 and 0.844, respectively, in the female participants. The optimal screening scores of alcohol use disorders in AUDIT-C were ≥7 in the male and ≥6 in the female participants; and in AUDIT and CAGE, ≥10 and ≥1, respectively, in the male, and ≥8 and ≥1 in the female participants.
Conclusion
AUDIT-C is considered useful in screening at-risk drinking and alcohol use disorders among college students.
INTRODUCTION
Korean students are legally allowed to drink alcohol when they reach college-entry age. During their college life, they have many opportunities to drink with classmates or club members, and accordingly, their drinking quantity increases. In 2003, the ratio of drinking among Korean college students was 93.6%,1) which is higher than the 86.9% and 80.9% of Canadian and American students, respectively.2) Korean college students have high frequencies of drinking and binge drinking, and consequently, have high rates of alcohol use disorder.1)
College students have been recognized as having a high risk of problem drinking.3) Since they have a higher risk of binge drinking than the general adult population, they are easily exposed to alcohol-associated accidents, smoking, sexually transmitted diseases, problems with managing their college life, and legal problems.4) Since drinking patterns in early adulthood usually continue into later life, it is very important to evaluate the drinking problems of college students, and to intervene the early stages of drinking problem development. According to previous studies, early and accurate screening tests and brief interventions for college students with problem drinking were proven effective for reducing not only alcohol consumption but also alcohol-associated problems.5,6)
The screening tests that are frequently used for college students problem drinking include cut down, annoyed, guilty, eye-opener (CAGE) and Alcohol Use Disorders Identification Test (AUDIT).7-9) The CAGE questionnaire is suitable for outpatients in primary care because it has only four questions and takes only about a minute to complete. However, in many studies that targeted college students, CAGE showed low sensitivity (range, 18% to 77%) and positive predictive value (range, 69% to 78%).10,11) The AUDIT is a 10-item questionnaire developed by the World Health Organization (WHO) that includes three questions on drinking frequency, drinking quantity and binge drinking frequency, and seven questions on drinking problems. In particular, questions on drinking quantity and frequency in the AUDIT measure binge drinking and heavy drinking, which may make the AUDIT suitable for assessing problem drinking in college students.
Nevertheless, the 10 questions of AUDIT are too many to allow it to be practically used in clinics or the emergency room. Thus, in the US and Europe, the utility of the first three questions in the AUDIT on alcohol intake and drinking frequency, which are called the Alcohol Use Disorders Identification Test Alcohol Consumption Questions (AUDIT-C), has been shown to be effective to screen problem drinking.12,13) In Korea, the usefulness of AUDIT-C in screening problem drinking cases has been also reported to be almost the same as that of AUDIT in adult males,14) but its utility for college students has not been evaluated yet. In this study, the validity of AUDIT-C was investigated in screening cases of at-risk drinking and alcohol use disorder among college students, whose drinking practices are considered different from that of the general adult population.
METHODS
1. Study Subjects
College students who visited the student health center of Chungnam National University between March 2011 and May 2011 were targeted in this study. A total of 387 subjects (198 male and 189 female) who identified themselves as alcohol drinkers were selected for participation in this study. All subjects agreed to study enrollment prior to filling out the questionnaires, and participated based on informed consent.
2. Methods
1) Diagnostic interviews
Subjects' drinking habits were assessed for at-risk drinking or alcohol use disorder through diagnostic interviews. Their usual drinking quantity per session, weekly drinking frequency, and maximum drinking quantity in a single session were investigated.
According to guidelines issued by the National Institute Alcohol Abuse and Alcoholism (NIAAA),15) binge drinking and heavy drinking among male students was defined as maximum drinking quantity exceeding four standard drinks at a single session and consumption of 14 drinks a week; and in female students, three drinks and seven drinks, respectively. A standard drink was considered 14 g of alcohol, equal to a small bottle of beer, a glass of wine, a shot of hard liquor, 1/4 bottle of 20% soju, or a bowl of makgeolli. At-risk drinking was defined as heavy drinking or binge drinking. Using the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision,16) alcohol use disorders were diagnosed through 'structured interviews' with four items on alcohol abuse and seven items on alcohol dependence.
2) Questionnaire surveys
In addition to the diagnostic interviews, information on the subjects' gender, age, religion, club activity, smoking, and age when they started drinking were investigated using a self-administered questionnaire, including the 10-item AUDIT and the CAGE.
(1) Alcohol Use Disorders Identification Test and Alcohol Use Disorders Identification Test Alcohol Consumption Questions
The AUDIT is a self-reporting questionnaire that the WHO9) developed in 1989. It includes 10 items with four scores per item, for a total score of 40. The AUDIT assesses three domains: the drinking frequency and amount in the past year, alcohol dependence symptoms, and drinking-associated problems. Regarding the validity of the AUDIT in Korea, Kim et al.17) suggested that a score of ≥12 is suggestive of problem drinking; ≥15, alcohol use disorder; and ≥26, alcohol dependence, in Korean men.
In this study, the concept of a standard drink (equivalent to 14 g of pure alcohol) suggested by the NIAAA15) in 2005 were applied to items 2 and 3 of the AUDIT. One bottle of soju, the most popular type of alcohol in Korea, contains 4 standard drinks (≒56 g of alcohol). For ease of understanding, the drinking quantity on item 2 was modified as follows: ① 1-2 drinks (or "≤1/2 bottle of soju") ② 3-4 drinks (or "≤1 bottle of soju") ③ 5-6 drinks (or "≤1.5 bottles of soju") ④ 7-9 drinks (or "2 bottles of soju") and ⑤ ≥10 drinks (or "≥2.5 bottles of soju"). Additionally, item 3 was modified to "≥5 drinks (or >1 bottle of soju)."18)
For obtaining the AUDIT-C score, the score of items 1 to 3 of the AUDIT on drinking frequency, average drinking quantity, and binge drinking frequency were summed. The maximum total score of the AUDIT-C is 12.12)
(2) Cut down, annoyed, guilty, eye-opener
CAGE was developed in 1970 and asks the following four questions: "Have you ever felt that you should cut down on your drinking?"; "Have people annoyed you by criticizing your drinking?"; "Have you ever felt bad or guilty about your drinking?"; and "Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (eye opener)?" Each question has a score, and a total score of 1 or more means there is a possibility of alcohol use disorder.7)
3. Data Analyses
The differences in sociodemographic features and alcohol drinking history of the male and female student groups were compared using a t-test and chi-square test. The differences in their age, age when they started drinking, weekly drinking frequency, maximum drinking quantity at a single session, and AUDIT, AUDIT-C, and CAGE scores were investigated using independent t-tests, and the differences in their religion, smoking, club activities, at-risk drinking and alcohol use disorder were examined using a chi-square test. In the male and female groups, the receiver operating characteristic (ROC) curve and the area under the ROC curve (AUROC) for screening at-risk drinking and alcohol use disorders were obtained. The differences in the AUROC of the three tools were investigated using comparison of dependent ROC curves. In addition, the sensitivity, specificity, positive predictive values and negative predictive values of the screening tools according to the scores were investigated. For statistical analysis, SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) and Medcalc Statistical Software ver. 11.6 (MedCalc Software; Broekstraat 52, Mariakerke, Belgium) were used.
RESULTS
1. Sociodemographic Features and Alcohol Drinking History
The mean age of the male students was 23.1 years (±2.8), and of the female students, 21.2 years (±1.9). The male group was significantly (P < 0.001) older than the female group. In terms of religion, there was no significant different between male and female participants, with 97 male (49.0%) and 93 female students (49.2%) having a religion. There was no significant difference in level of club participation of male students (43.9%) and female students (48.7%). There were 53 male smokers (27.7%) and only two female smokers (1.1%), which showed a significant difference (P < 0.001).
The mean age of the male students when they started drinking was 18.4 years (±2.2), and of the female students, 18.6 years (±1.7), which showed no significant difference. The mean weekly drinking frequency of the male students was 1.2 times (±0.8), and of the female students, 0.9 times (±0.9), which showed a significant difference (P < 0.001). The mean drinking quantity at one time of the male students was 4.1 drinks (±2.3), and of the female students, 2.8 drinks (±2.1), which showed a significant (P < 0.001) difference. The mean maximum drinking quantity at one time of the male students was 4.7 drinks (±2.3), and of the female students, 3.2 drinks (±2.1), which also showed a significant (P < 0.001) difference.
The mean AUDIT score of the male students was 6.7 (±4.1), and of the female students, 5.1 (±4.5), which showed a significant (P < 0.001) difference. The mean AUDIT-C score of the male students was 4.8 (±2.2), and of the female students, 3.3 (±2.2), which showed a significant (P < 0.001) difference. The mean CAGE score of the male students was 0.5 (±0.7), and of the female students, 0.4 (±0.8), which showed no significant difference. As described above, statistically significant differences between the male and female student groups were observed in their mean age, smoking, weekly drinking frequency, mean drinking quantity at one time, and maximum drinking quantity at one time (Table 1). There were 64 at-risk male drinkers (32.3%) and 79 at-risk female drinkers (41.8%), and 21 male students (10.6%) and 18 female students (9.5%) with alcohol use disorders (Table 2).
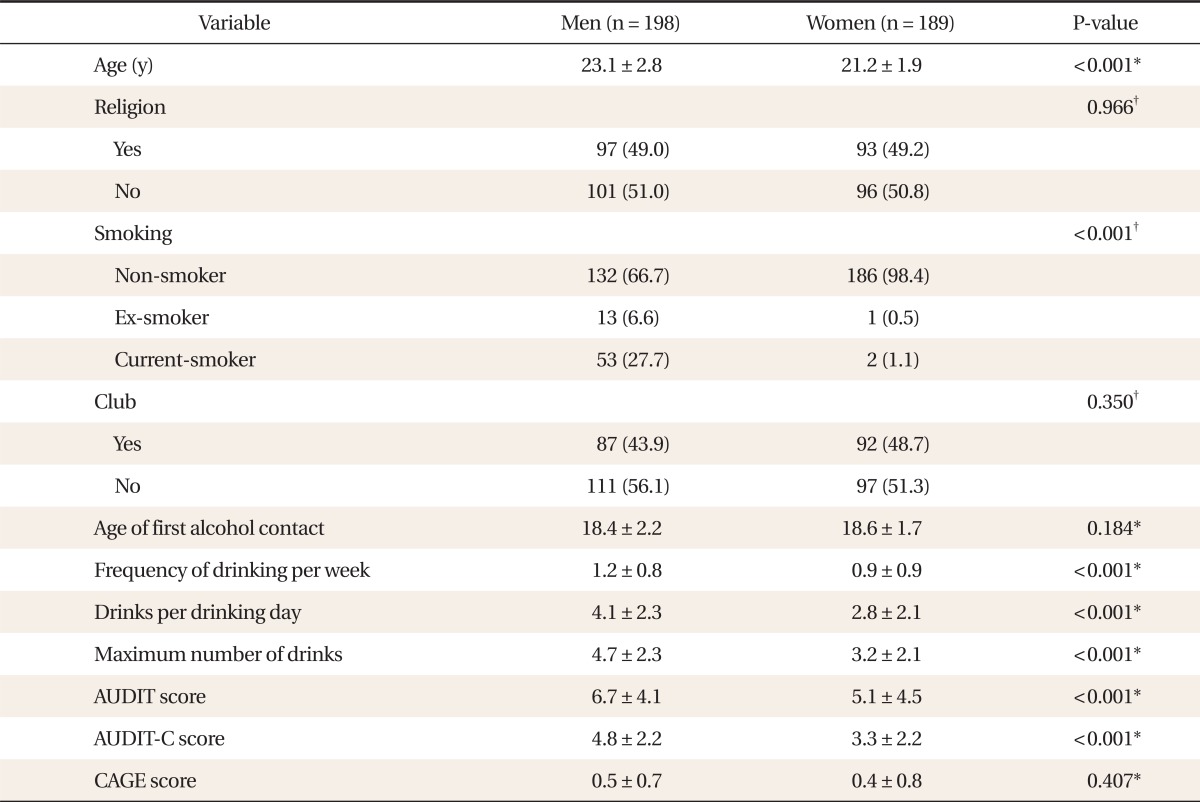
General & drinking characteristics of subjects
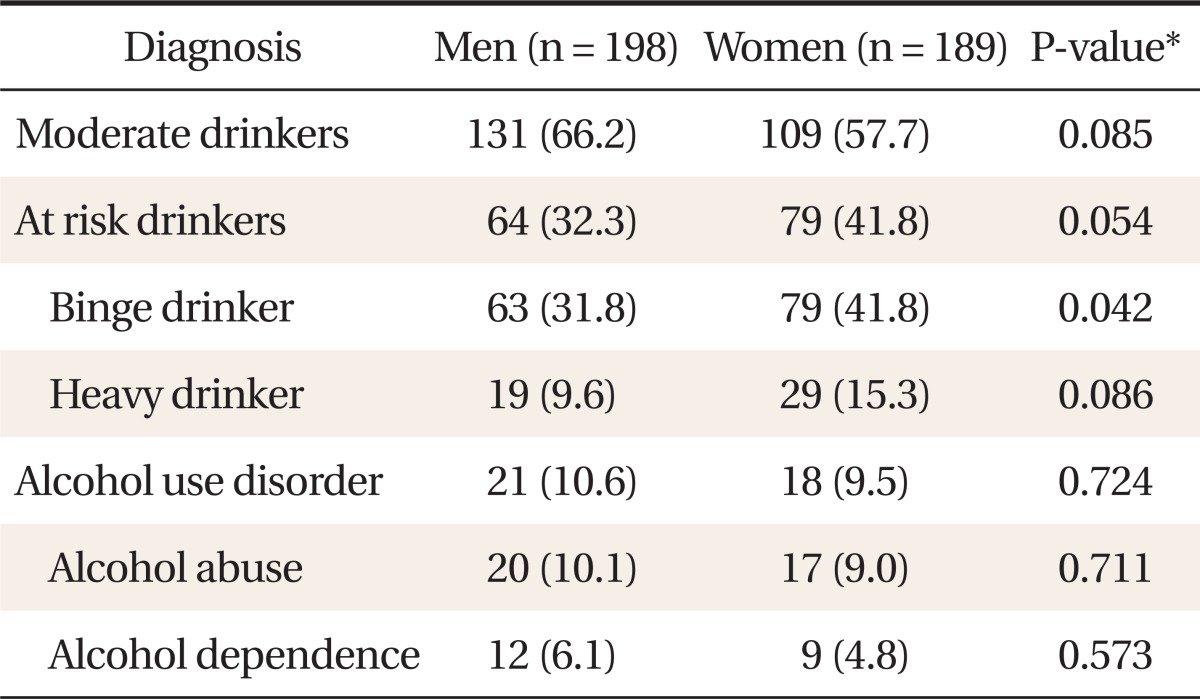
Diagnostic interview results
2. Validity of the Questionnaires for Screening At-risk Drinking
The AUROCs (95% confidence interval [CI]) of the three questionnaires for screening the male at-risk drinkers were as follows: AUDIT-C, 0.927 (0.881-0.959); AUDIT, 0.906 (0.856-0.943); and CAGE, 0.643 (0.572-0.709). The AUDIT-C showed the largest AUROC. The difference in the AUROCs of AUDIT-C and AUDIT was not statistically significant, and the AUROC of AUDIT-C was significantly (P < 0.001) larger than that of the CAGE (Figure 1).

Receiver operating characteristic (ROC) curves for identifying at-risk drinking. Area under the ROC curve (AUROC) (95% confidence interval) of Alcohol Use Disorders Identification Test Alcohol Consumption Questions (AUDIT-C) was 0.927 (0.881-0.959) in the male students and 0.921 (0.873-0.956) in the female students, and AUROC of Alcohol Use Disorders Identification Test (AUDIT) was 0.906 (0.856-0.943) in the male students and 0.898 (0.846-0.937) in the female students. AUROC of cut down, annoyed, guilty, eye-opener (CAGE) was 0.643 (0.572-0.709) in the male students and 0.657 (0.585-0.724) in the female students.
In the male students, the most appropriate cutoff score of AUDIT-C for screening at-risk drinking was 6 with sensitivity of 81.3%; specificity, 88.8%; positive predictive value, 77.6%; and negative predictive value, 90.8%. The most appropriate cutoff score of AUDIT for screening at-risk drinking was 8 with sensitivity of 82.8%; specificity, 88.1%; positive predictive value, 76.8%; and negative predictive value, 91.5%. In the CAGE, the most appropriate cutoff score for screening at-risk drinking was 1 with sensitivity of 57.8%; specificity, 69.4%; positive predictive value, 47.4%; and negative predictive value, 77.5% (Table 3).
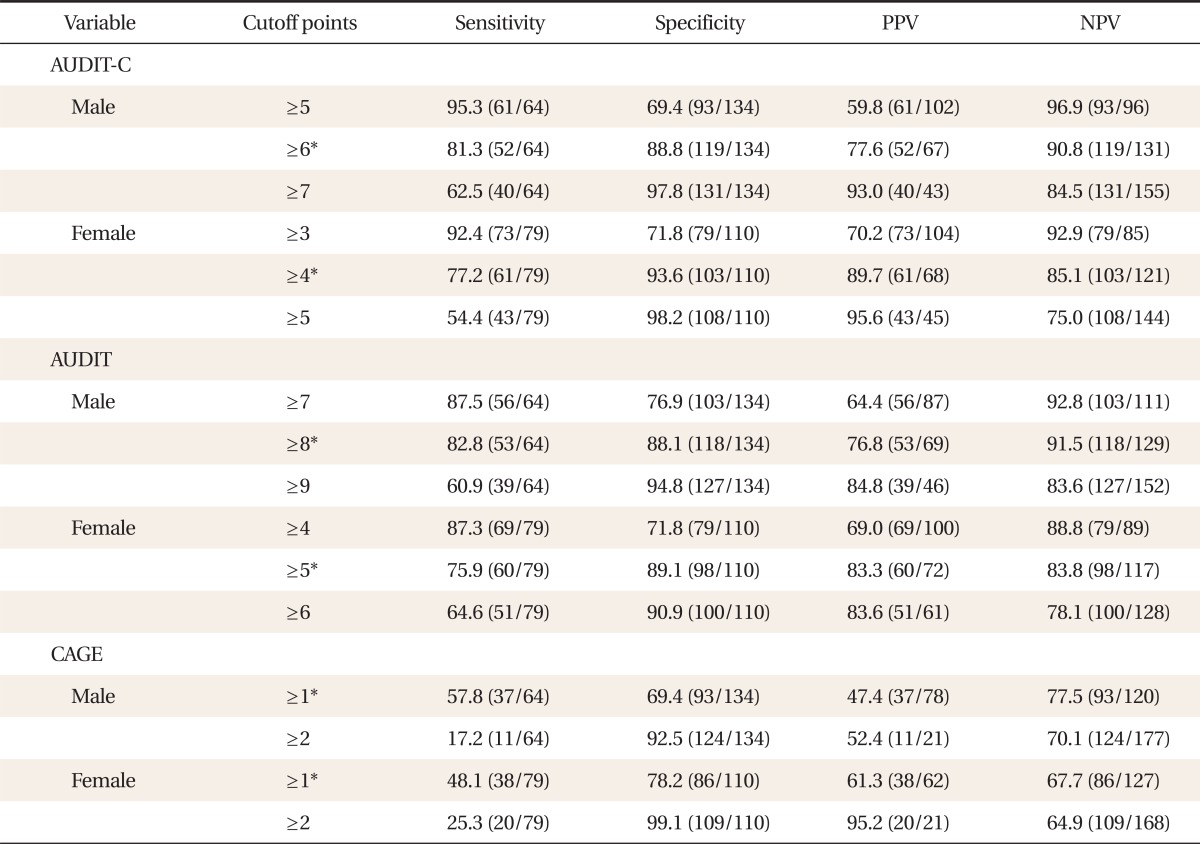
Performance of screening instruments for identifying at-risk drinking according to cutoff points
The AUROCs (95% CI) of the three questionnaires for screening female at-risk drinkers were as follows: AUDIT-C, 0.921 (0.873-0.956); AUDIT, 0.898 (0.846-0.937); and CAGE, 0.657 (0.585-0.724). The AUDIT-C showed the largest AUROC. However, the AUROC of AUDIT-C did not significantly differ from that of the AUDIT and was significantly (P < 0.001) larger than that of the CAGE. The AUROC of the AUDIT was significantly (P < 0.001) larger than that of the CAGE (Figure 1).
For the female students, the most appropriate cutoff score of the AUDIT-C for screening at-risk drinking was 4 with sensitivity of 77.2%; specificity, 93.6%; positive predictive value, 89.7%; and negative predictive value, 85.1%. The most appropriate cutoff score of the AUDIT for screening at-risk drinking was 5 with sensitivity of 75.9%; specificity, 89.1%; positive predictive value, 83.3%; and negative predictive value, 83.8%. Finally, the most appropriate cutoff score of the CAGE for screening at-risk drinking was 1 with sensitivity of 48.1%; specificity, 78.2%; positive predictive value, 61.3%; and negative predictive value, 67.7% (Table 3).
3. Validity of the Questionnaires for Screening Alcohol Use Disorders
The AUROCs (95% CI) of the three questionnaires for screening male alcohol use disorders were: AUDIT-C, 0.902 (0.852-0.940); AUDIT, 0.936 (0.892-0.966); and CAGE, 0.712 (0.643-0.774), which showed the largest AUROC in the AUDIT. The difference in the AUROCs of the AUDIT-C and AUDIT was not significant, but the AUROCs of the AUDIT-C and AUDIT were much (P < 0.001) larger than the AUROC of CAGE (Figure 2).

Receiver operating characteristic (ROC) curves for identifying alcohol use disorders. Area under the ROC curve (AUROC) (95% confidence interval) of Alcohol Use Disorders Identification Test Alcohol Consumption Questions (AUDIT-C) was 0.902 (0.852-0.940) in the male students and 0.939 (0.895-0.969) in the female students. Alcohol Use Disorders Identification Test (AUDIT) was 0.936 (0.892-0.966) in the male students. and 0.960 (0.921-0.983) in the female students. Cut down, annoyed, guilty, eye-opener (CAGE) was 0.712 (0.643-0.774) in the male students and 0.844 (0.784-0.892) in the female students.
For the male students, the most appropriate cutoff score of the AUDIT-C for screening alcohol use disorders was 7 with sensitivity of 85.7%; specificity, 85.9%; positive predictive value, 41.9%; and negative predictive value, 98.1%. The most appropriate cutoff score of the AUDIT for screening alcohol use disorders was 10 with sensitivity of 81.0%; specificity, 91.0%; positive predictive value, 51.5%; and negative predictive value, 97.6%. Finally, the most appropriate cutoff score of the CAGE for screening alcohol use disorders was 1; sensitivity, 71.4%; specificity, 64.4%; positive predictive value, 19.2%; and negative predictive value, 95.0% (Table 4).
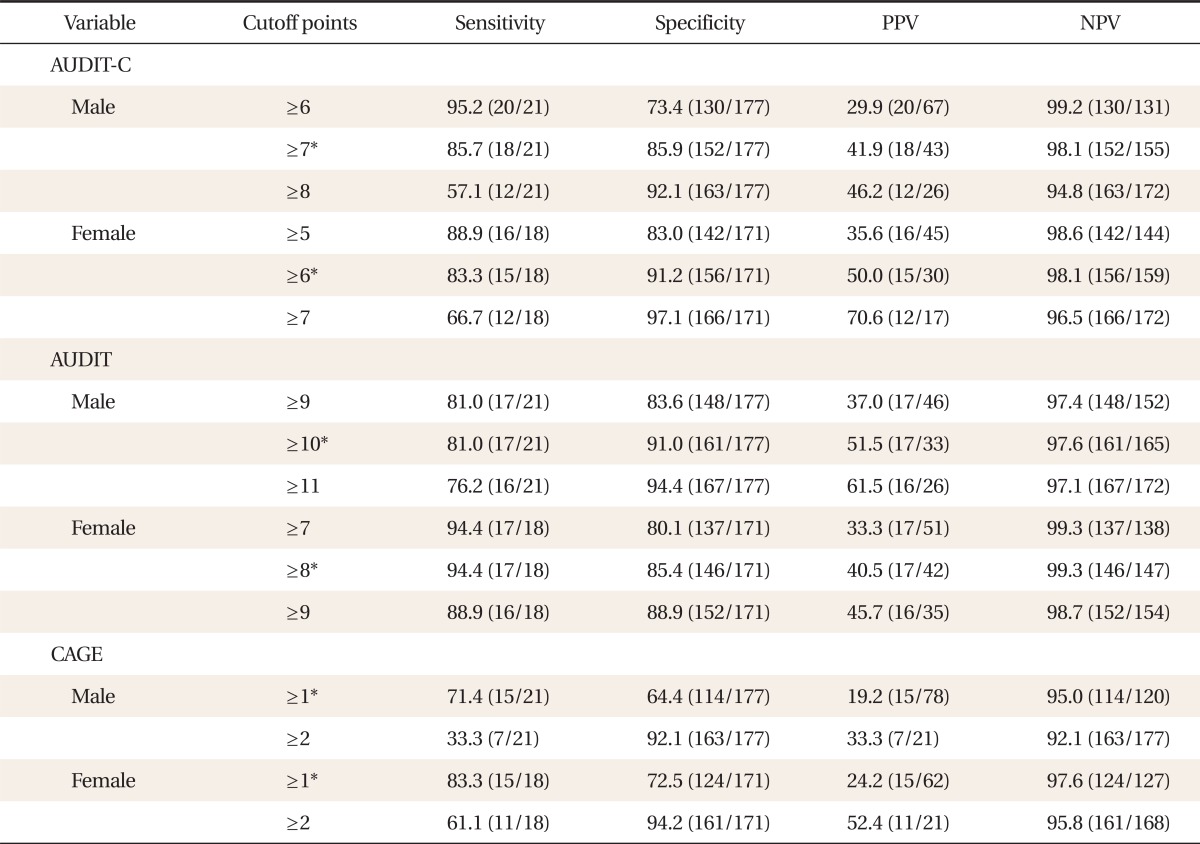
Performance of screening instruments for identifying alcohol use disorders according to cutoff points
The AUROCs (95% CI) of the three questionnaires for screening female alcohol use disorders were: AUDIT-C, 0.939 (0.895-0.969); AUDIT, 0.960 (0.921-0.983); and CAGE, 0.844 (0.784-0.892), which showed the largest AUROC in the AUDIT. The difference in the AUROCs of the AUDIT-C and AUDIT was not significant, and the AUROC of the AUDIT was much larger than that of the CAGE (P = 0.021). No significant difference in the AUROCs of the AUDIT-C and CAGE was observed (Figure 2).
For the female students, the most appropriate cutoff score of the AUDIT-C for screening alcohol use disorders was 6; sensitivity, 83.3%; specificity, 91.2%; positive predictive value, 50.0%; and negative predictive value, 98.1%. The most appropriate cutoff score of the AUDIT for screening alcohol use disorders was 8; sensitivity, 94.4%; specificity, 85.4%; positive predictive value, 40.5%; and negative predictive value, 99.3%. Finally, the most appropriate cutoff score of the CAGE score for screening alcohol use disorders was 1; sensitivity, 83.3%; specificity, 72.5%; positive predictive value, 24.2%; and negative predictive value, 97.6% (Table 4).
DISCUSSION
The present study is thought to be meaningful in that it suggests that AUDIT-C may be valid for screening at-risk drinking and alcohol use disorders among college students.
In many studies conducted in Korea and other countries, AUDIT-C was confirmed to be useful for screening at-risk drinking and alcohol use disorders. In the US, the AUROCs of AUDIT and AUDIT-C for screening problem drinking, which included at-risk drinking and alcohol use disorders, in men were the same at 0.88/0.8812) as they were in women, at 0.87/0.91.19) The above results indicate that the 10-item AUDIT and the three-item AUDIT-C have almost the same capability to screen at-risk drinking and alcohol use disorders. These results were verified in a study conducted in European countries such as Belgium and Spain.20) In an American study, the score for screening problem drinking among men was suggested as an AUDIT-C score of 4 or more with a sensitivity and specificity of 86% and 72%, respectively;12) and among women, an AUDIT-C score of 2 or more with a sensitivity and specificity of 92% and 78%, respectively.19) In a Spanish study, the score for screening at-risk drinking and alcohol use disorders among men was suggested as 5 or more with a sensitivity and specificity of 92% and 74%, respectively; and among women, a score of 4 or more with a sensitivity and specificity of 92% and 68%, respectively.21)
In Korea, Seong et al.14) reported the validity of AUDIT-C for screening adult male at-risk drinkers. In the study, the sensitivity and specificity of AUDIT-C were reported as 82% and 76%, respectively, with a cutoff score of 8 or more, for screening cases of at-risk drinking. According to the present study, an optimal cutoff score of the AUDIT-C that could be applied to screen atrisk drinking among college students was suggested as 6 or more for men and 4 or more for women. In addition, Seong et al.14) suggested an AUDIT-C score of 9 or more for screening alcohol use disorders with a sensitivity and specificity of 76% and 79%, respectively. In comparison, in the current study, the score for alcohol use disorders among male students was suggested as 7 or more, and among female students, 6 or more. Consequently, the cutoff scores suggested by our study were higher than those in foreign studies but lower than those in other Korean studies that targeted Korean adults. In interpretation of these differences, the differences in the characteristics of the subjects targeted in the studies should be considered. That is, the differences in the suggested scores may have been due to the differences in the drinking cultures between Korea and other countries, and between adults and college students. In addition, a straight forward comparison of our study with Seong et al.'s study may not be appropriate because no diagnostic interviews were conducted in Seong et al.'s study. Seong et al.14) classified their subjects with problem drinking and alcohol use disorders based on the total score of the 10-item AUDIT according to the study of Kim et al.17) instead of diagnostic interviews.
The limitations of the current study are as follows. First, all the subjects were from only one university, so they may not represent all Korean college students. Diversified sample sources with a larger sample size may be needed in future studies. Second, there might have been memory distortions that could have affected the results of the questionnaire, particularly in the items of the alcohol intake and the frequency of such intake. However, this limitation may be common in most self-administered questionnaires.
In conclusion, AUDIT-C is considered a useful, convenient and time-saving tool for screening at-risk drinking and alcohol use disorders among Korean college students.
Notes
No potential conflict of interest relevant to this article was reported.