INTRODUCTION
Dementia is defined by a disorder of the executive function of the frontal lobe including memory, attention, language function, spatial-temporal ability, or judgment, causing difficulty in daily life or social life. According to a regional epidemiological study in Korea, the prevalence rate of dementia in old people over the age of 65 is 9.5% to 13.0%, which is substantial when compared to other studies performed by the same diagnostic standards in other countries.1) Also, another epidemiological characteristic of dementia in Korea is that the prevalence rate is higher in females than males-a trend which becomes more intensified in older age. This is estimated to mostly result from the higher prevalence of Alzheimer's disease in elderly females. Also, it is known that less educated people have a higher occurrence rate of dementia, and this is considered to be one of the causes for the high prevalence rate of dementia of Korean old people, who generally have a lower education level compared to other countries.1) On the survey in 2008, the illiteracy rate was higher in females (2.7%) than in males (0.5%), and the difference was greater with age, reaching 6.0% in the 60s and 20.2% in the 70s.2)
Although the importance of early diagnosis is becoming more and more emphasized with the rapid increase in prevalence of dementia, it is not easy to diagnose. Actually, it is known that the false-negative diagnosis rate of dementia reaches 35% to 90% in primary medical institutions.3) For the diagnosis of dementia, an assessment on cognitive function should be performed by questionnaire, mental status examination, and neuropsychological test in order to understand the degree of degeneracy in cognitive function. The Mini-Mental State Examination (MMSE) has been the most widely used examination tool for dementia and cognitive function since its first use in 1975.4)
In a study on the normal criteria values of the Korean-MMSE (K-MMSE) which is now widely used, K-MMSE scores in the uneducated group and educated group (at least primary schooling) showed a significant difference. However, there was not a significant difference among participants in the highly educated group (over primary schooling).5) In various studies, the limitations of the K-MMSE included influence of age and education level, difficulty in discovering early decrease in cognitive function, and inability of the illiterate persons to take the test.6) Most of the uneducated people also found subtraction to be difficult. Therefore, the K-MMSE allows adding a score of 2 at maximum to the item 'serial subtraction from 100-7' when the patient is uneducated or illiterate. On the other hand, the MMSE-K, which was translated and modified by Yong-Cheol Gwon, Jong-Han Park, and others in 1989, is allowing those who cannot perform 'serial subtraction from 100-7' to replace it by pronouncing 'sam-cheon-ri-gang-san' in reverse order. However, this 'sam-cheon-ri-gang-san' has been modified from the 'world' in the MMSE by authors during translation7) and some pointed out that this is more difficult than 'serial subtraction from 100-7' for uneducated or illiterate patients.8) However, until now, there was no study which included other serial subtraction items to replace this one for uneducated or illiterate patients in or out of Korea. Therefore, this study was performed under the hypothesis that 'serial subtraction from 40-4,' 'serial subtraction from 20-2,' 'serial subtraction from 10-1,' and others may have better correlation to the global deterioration scale, which shows the severity of dementia, than 'serial subtraction from 100-7' in the K-MMSE for uneducated participants.
METHODS
1. Study Subjects
The study was performed on patients over 50 years old who had undergone MMSE, the Global Deterioration Scale (GDS),9) a questionnaire assessment, and general neuropsychiatric examinations for memory disorders in the neurological department and neuropsychiatric department of 4 university medical centers in Seoul and Gyeonggi province. The GDS is a tool used to assess not only cognitive function but also the ability to maintain daily life, participation in adverse activities. All participants in this study signed an informed consent form and were given an explanation of the study objectives, and those with severe auditory, visual, or speech disabilities were excluded (Appendix 1). A total of 184 patients participated in the study and the analysis was made on 169 subjects excluding 15 subjects with insufficient data.
2. Study Methods
After a survey of general demographic information about the patients, such as education level of the patient's guardian, an assessor had the patient perform the serial subtractions (5 times of serial 100-7s subtractions, 5 times of serial 40-4s subtractions, 5 times of serial 20-2s subtractions, and reverse-counting from 10 to 1) to write down the number of wrong answers. The assessor also calculated the GDS score of the subject by general clinical psychiatric assessment. The assessor was a clinical psychiatrist or well-trained nurse. The GDS, the representative grade scale to measure the severity of dementia, is a tool with proven reliability and validity in Korea with the advantage of not being greatly influenced by the education level of the patient.10) The cognitive function was assessed from 1 (no cognitive disorder) to 7 (late-phase severe cognitive disorder).
The existing MMSE takes the number of right answers from 5 times of serial 100-7s subtraction. We defined the one replaced by 5 times of serial 40-4s subtractions as MMSE4 and the one replaced by 5 times of serial 20-2s subtractions as MMSE2. MMSE1 was defined as the half of the total number of right answers in reverse-counting from 10 to 1, as it has a total score of 10. Permission to perform the study was obtained by the institutional review board at Kyung Hee University Hospital. The informants signed an informed consent as a proxy of the subjects.
3. Statistical Analysis
The difference between two groups was tested by independent t-test and chi-square test. In order to find the relationship between serial subtraction and GDS score, a Pearson's correlation coefficient was obtained. Also, receiver operating characteristic (ROC) curve analysis was performed to compare the ability to diagnose dementia with a score over 3 among MMSE, MMSE4, MMSE2, MMSE1, and GDS. The Stata SE ver. 10.0 (Stata Co., College Station, TX, USA) was used in data processing and all significance levels were defined by P < 0.05.
RESULTS
1. Demographics of Study Subjects
Total subjects included 62 males (36.7%) and 107 females (63.3%). Thirty-six of them were included in the uneducated group and 133 in the educated group (at least primary schooling). Ninety-one point-seven percent of the uneducated group were females while 55.6% of educated group were females (P < 0.001). The average age in the uneducated group was 76.6, and in the educated group was 73.8, with a statistically significant difference (P = 0.040). The average MMSE score in the uneducated group was 16.8 and the score in the educated group was 21.3 (P < 0.001) (Table 1). In all kinds of serial subtractions, the uneducated group had a larger number of wrong answers (P < 0.001). On the other hand, scores in MMSE, MMSE4, MMSE2, and MMSE1 which were the sum of the right answers in serial subtractions were higher in the educated group (P < 0.001) (Table 1).
2. Relationship between Global Deterioration Scale Scores and Serial Subtractions by Education Level
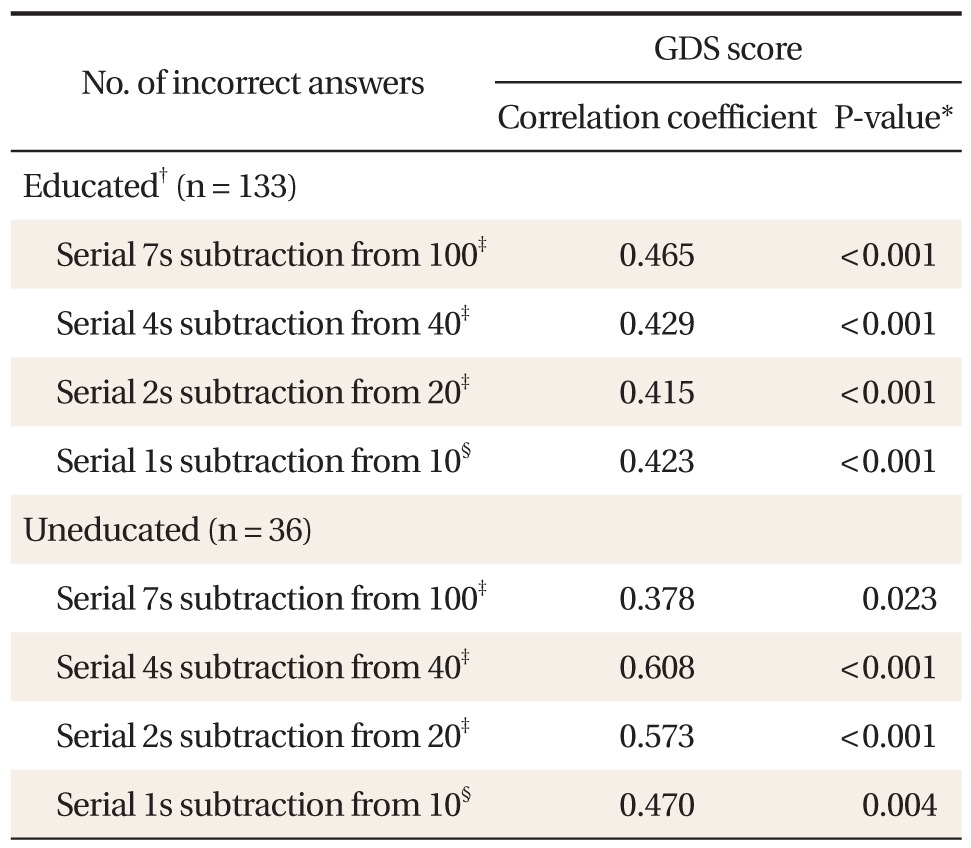
In the educated group, serial 100-7s subtraction showed the highest correlation coefficient with GDS score (correlation coefficient of 0.465, P < 0.001) without much difference with the scores in serial 40-4s subtraction, serial 20-2s subtraction, and serial 10-1s subtraction. In the uneducated group, serial 40-4s subtraction showed the highest correlation coefficient with GDS score (correlation coefficient of 0.608, P < 0.001) and serial 100-7s subtraction had the lowest coefficient (correlation coefficient of 0.378, P = 0.023) (Table 2).
3. Relationship between Global Deterioration Scale Scores and Mini-Mental State Examination Scores by Education Level
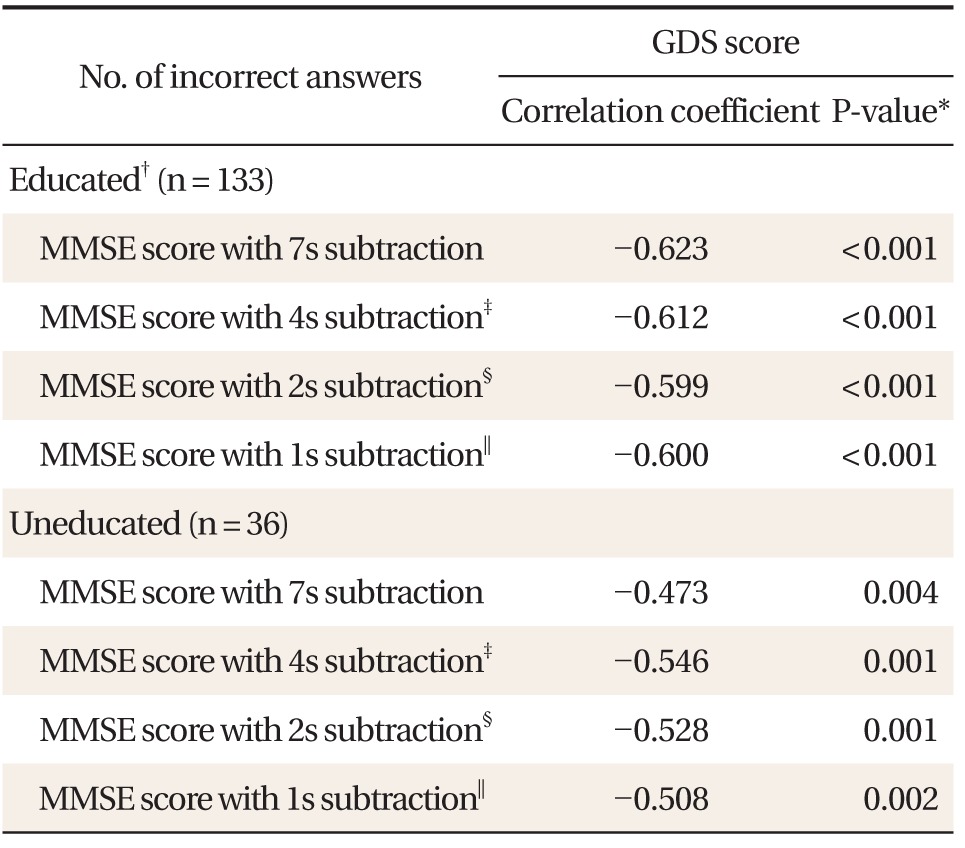
In the educated group, the MMSE score including serial 100-7s subtraction showed the highest correlation coefficient with the GDS score (correlation coefficient, -0.623; P < 0.001) without showing much difference with those in serial 40-4s subtraction, serial 20-2s subtraction, and serial 10-1s subtraction. In the uneducated group, the MMSE score including serial 40-4s subtraction showed the highest correlation coefficient with the GDS score (correlation coefficient, -0.546; P < 0.001), and the score including serial 100-7s subtraction had the lowest coefficient (correlation coefficient, -0.473; P = 0.023) (Table 3).
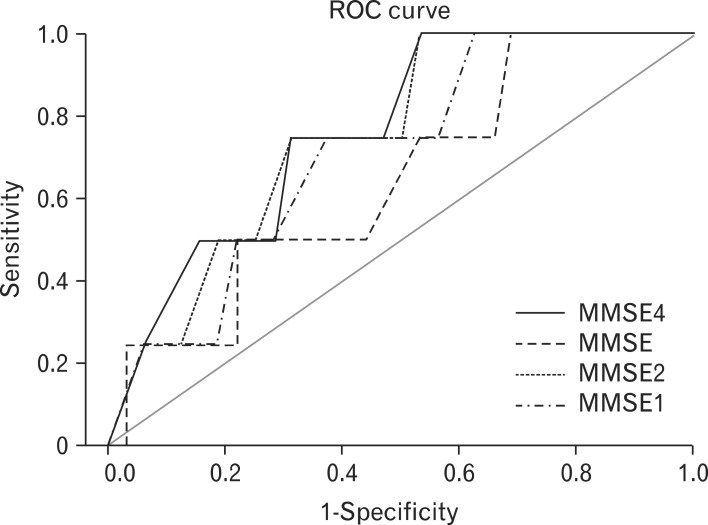
4. Receiver Operating Characteristic Curve Analysis on Mini-Mental State Examination for Diagnosis of Dementia (Global Deterioration Scale Score over 3) by Education Level
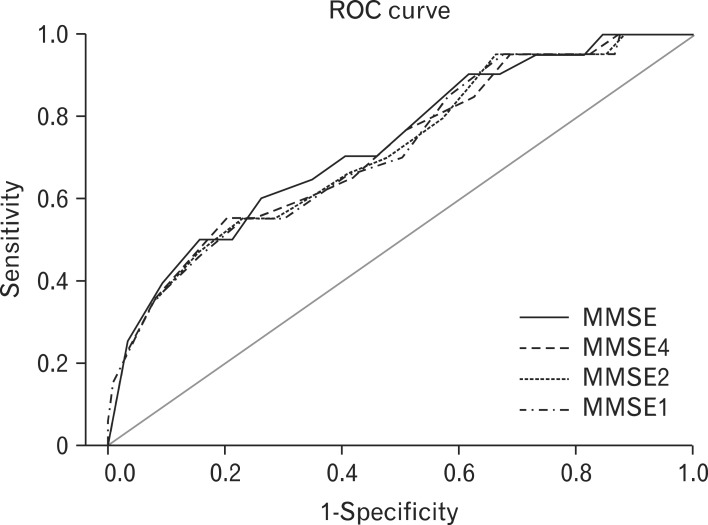
ROC curve analysis on the diagnosis of dementia patients with GDS score over 3 was performed. The areas under the curve (AUCs) on the MMSE including serial 100-7s subtraction, MMSE4 including serial 40-4s subtraction, MMSE2 including serial 20-2s subtraction, and MMSE1 including serial 10-1s subtraction for the diagnosis of dementia were 0.648 (95% confidence interval [CI], 0.382 to 0.915), 0.770 (95% CI, 0.559 to 0.980), 0.758 (95% CI, 0.547 to 0.968), and 0.711 (95% CI, 0.479 to 0.943), respectively (Figure 1). In the educated group, the AUCs on the MMSE, MMSE4, MMSE2, and MMSE1 for the diagnosis of dementia were 0.729 (95% CI, 0.609 to 0.850), 0.719 (95% CI, 0.595 to 0.842), 0.716 (95% CI, 0.592 to 0.840), and 0.714, respectively (Figure 2).
DISCUSSION
Low education level is one of the well-known risk factors for dementia.11) Illiteracy in particular is relatively high compared to western countries, so more attention is needed when examining for and diagnosing dimentia. In Korea, the K-MMSE (MMSE-K) and Korean version of the revised Hasegawa Dementia Scale are the most widely used examinations for the diagnosis of dementia.3) These two examinations both include 'serial 100-7s subtraction,' which leaves the constant questions on these two examination methods from the limitation of accurate assessment of uneducated old people.6) It has also been revealed in a study performed on old African-American people that 'serial 100-7s subtraction' is more difficult than 'pronouncing a word of a few syllables over the left' and that education level is a very important factor in determining MMSE.12)
In this study, we tried to investigate whether 'serial 100-7s subtraction' is appropriate as an assessment item on the MMSE for uneducated old people (the uneducated group). As a result, though serial 100-7s subtraction presented the highest correlation coefficient to the GDS score in the educated group, serial 40-4s subtraction showed the highest correlation to the GDS score in the uneducated group, while serial 100-7s subtraction showed the lowest correlation. Therefore, 'serial 100-7s subtraction' should be considered for replacement with 'serial 40-4s subtraction' when MMSE assessment is made for the uneducated group.
This study has a few limitations. First, the number of subjects in the uneducated group was relatively small (n = 36). However, in spite of this limitation, 'serial 100-7s subtraction' showed no significant correlation to the GDS score in the uneducated group. Therefore, it can be said that 'serial 100-7s subtraction' is no better an assessment item than any other serial subtractions for the uneducated group. Second, there is another method to assess the severity of dementia other than GDS, which is clinical dementia rating (CDR). Thus a correlation analysis with CDR is also needed. Third, it is hard to completely eliminate the variance among different assessors since this study was based on patient assessments performed in 4 different medical centers. However, the differences are not expected to be great since neuropsychiatric experts or skilled nurses performed the examinations in all 4 hospitals.
Although we analyzed whether serial subtractions have significant correlation to the GDS scores in the uneducated group and educated group (at least primary schooling), we didn't compare this between these two groups. This is because the sample sizes in these two groups were largely different and the hypothesis of this study was that 'serial 100-7s subtraction would not be appropriate for the uneducated group as an assessment method for dementia.'
In conclusion, 'serial 100-7s subtraction' used in the assessment for dementia is considered to be appropriate for the educated group (at least primary schooling); however, it is not appropriate for the uneducated group. Instead, other serial subtractions such as the 'serial 40-4s subtraction' are recommended.