Sociodemographic Characteristics of Underweight Korean Adults: Korea National Health and Nutrition Examination Survey, 2007-2010
Article information
Abstract
Background
Underweight is associated with increased risk of mortality and morbidity. It is reported that the prevalence of underweight is increasing among Korean young women. However, there have been few studies on sociodemographic factors related to being underweight. This study was conducted to elucidate the sociodemographic characteristics of Korean underweight adults.
Methods
This study is a cross-sectional study of 7,776 adults aged 25 to 69 years using data from the Korea National Health and Nutrition Examination Survey, 2007-2010. Study subjects were composed of underweight and normal-weight adults excluding overweight adults. Body mass index was calculated from measured height and weight. Health behaviors such as smoking, drinking, and physical activity were surveyed through self-administered questionnaires, and socioeconomic status, marital status, and history of morbidity were surveyed through face-to-face interviews.
Results
Women had a higher frequency of underweight (10.4% vs. 7.0%, P < 0.001) than men. Among men, current smoking (odds ratio [OR], 1.62) and past history of cancer (OR, 2.55) were independently related to underweight. Among women, young age (OR, 2.06), former smoking (OR, 1.69), and being unmarried (OR, 1.56) were identified as independently related factors of underweight. In addition, among both men and women, alcohol drinking (men OR, 0.57; women OR, 0.77) and past history of chronic diseases (men OR, 0.55; women OR, 0.43) were independently related to a lower frequency of underweight.
Conclusion
We showed that various sociodemographic factors were associated with underweight. It was ascertained that there were differences in the sociodemographic factors related to underweight between Korean men and women.
INTRODUCTION
Healthy weight refers to a range of weight that is optimal for health, which is defined as a body mass index (BMI) of 18.5 to 24.9 kg/m2.1) Individuals whose weights are below or above this range are considered to have unhealthy weights because of increased health risks. Although both obesity and underweight are related to an increased risk of mortality2) and morbidity,3-5) health risks of underweight are less known than those of obesity.
Among Korean women aged 20 years and over, the age-adjusted prevalence of underweight insignificantly increased between 1998 and 2007 (5.5% → 6.7%, P for trend = 0.199), while the age-adjusted prevalence of underweight among Korean men decreased from 4.8% in 1998 to 2.8% in 2007 (P for trend = 0.020). Especially among women aged 20 to 39, the prevalence of underweight had a significant increasing tendency from 8.2% in 1998 to 13.2% in 2007 (P for trend = 0.003) unlike that among men.6) Khang and Yun6) emphasized that more national studies regarding the increasing tendency of underweight prevalence among young Korean women are warranted.
In a previous study7) of a Canadian population using the National Population Health Survey, underweight people were more likely to be females, youth under 25 years of age, singles, current smokers and individuals with poor self-perceived health. In another study8) of female students in Poland, underweight was shown to be related to higher socioeconomic status (SES). Shin et al.9) showed that underweight prevalence varied significantly depending on maternal education level and residential district. However, there have been only few epidemiologic studies on the sociodemographic characteristics of Korean underweight adults. Furthermore, previous studies have limitations such as including only adolescent girls or college female students as study subjects. This study was conducted to elucidate the sociodemographic characteristics of underweight Korean adults using data from Korea National Health and Nutrition Examination Survey (KNHANES), 2007-2010.
METHODS
1. Study Population
We used data from KNHANES, 2007-2010 for this study. The design of KNHANES was introduced in a previous study10) in detail; it was a nationwide representative survey with a complex, stratified, multistage, cluster-sampling design used to assess the health and nutritional status of the non-institutionalized civilian population in Korea. A total of 20,063 individuals who were 25 to 69-years-of-age participated in KNHANES, 2007-2010. Among them, pregnant women (n = 150), individuals who did not conduct a measure of height or weight (n = 1,236), and those who failed to complete the questionnaires (n = 159) were excluded, leaving 18,518 individuals. Because the aim of this study was to reveal the sociodemographic characteristics of underweight adults compared with normal-weight adults, we did additional exclusion of overweight adults who had a BMI ≥ 23.0 kg/m2. Finally, data of 7,776 individuals (2,772 men and 5,004 women) who were assessed to be underweight (BMI ≤ 18.4 kg/m2) or normal weight (BMI, 18.5 to 22.9 kg/m2) were available for the final analysis.
2. Measurements
Anthropometric measurements were carried out wearing light clothing and no shoes by a trained professional research team at a mobile examination center. Height and weight were measured to one decimal place using a calibrated stadiometer (SECA 225; SECA Deutschland, Hamburg, Germany) and scale (GL-6000-20; CASKOREA, Seoul, Korea), respectively. BMI was calculated using the formula: weight (kg) ÷ (height [m])2.
Health behaviors such as smoking, drinking, and physical activity were investigated through self-administered questionnaires. Smoking status was classified into three groups (non-smokers, ex-smokers, and current smokers), and drinking status was classified into two groups (<1 times/mo and ≥1 times/mo). Physical activity was assessed by the Korean version of the International Physical Activity Questionnaire (IPAQ) short form. Physical activity level was calculated as a continuous score and was categorized into three groups (low, moderate, and high) in accordance with the guidelines for data processing and analysis of the IPAQ.11)
SES, marital status, and history of morbidity were investigated through face-to-face interviews. Education level, occupation, and household income were investigated as indicators of SES. Education level was classified into three groups (≥ college graduation, high school graduation, and ≤ middle school graduation). Occupation was also classified into three groups (non-manual workers, manual workers, and other [soldiers, students, homemakers, and unemployed]) by the Korean Standard Classification of Occupation revised in 2007. For classification of household income level, household equivalent income was calculated using the formula: total family income ÷ √the number of family members. After that, household equivalent income was categorized into tertiles (high, middle, and low) for each survey year. Marital status was classified into three groups (married, unmarried, and other [divorced, separated, and widowed]). Subjects were asked about their history of diagnosed chronic diseases such as hypertension, diabetes, dyslipidemia, stroke, ischemic heart disease, arthritis, asthma, renal failure, or liver cirrhosis and were considered as having a history of chronic disease if they had a history of a physician diagnosing any kind of chronic disease. Subjects were asked about their history of cancer of the stomach, liver, colon, breast, cervix, lung, and other organs, and were considered as having a history of cancer if they had a history of a physician diagnosing any kind of cancer.
3. Statistical Analysis
We performed all analyses by taking into account the KNHANES sampling data according to the instructions of raw data analysis of KNHANES. Data were expressed as mean ± standard error or percentage ± standard error. The simple relationship between underweight and each sociodemographic factor was assessed by the Chi-square test. Multiple logistic regression analyses were conducted to elucidate factors that were independently related to underweight. All statistical analyses were carried out with PASW SPSS ver. 18 (SPSS Inc., Chicago, IL, USA). A P-value of < 0.05 was considered statistically significant.
RESULTS
The sociodemographic characteristics of the study subjects are shown in Table 1. Men were older (43.6 ± 0.3 years vs. 41.0 ± 0.2 years, P < 0.001) and had a lower frequency of underweight (7.0% vs. 10.4%, P < 0.001) compared to women. Men had higher physical activity levels, were more likely to be current smokers and alcohol drinkers, had lower education levels and household incomes, and comprised a higher proportion of manual workers than women.
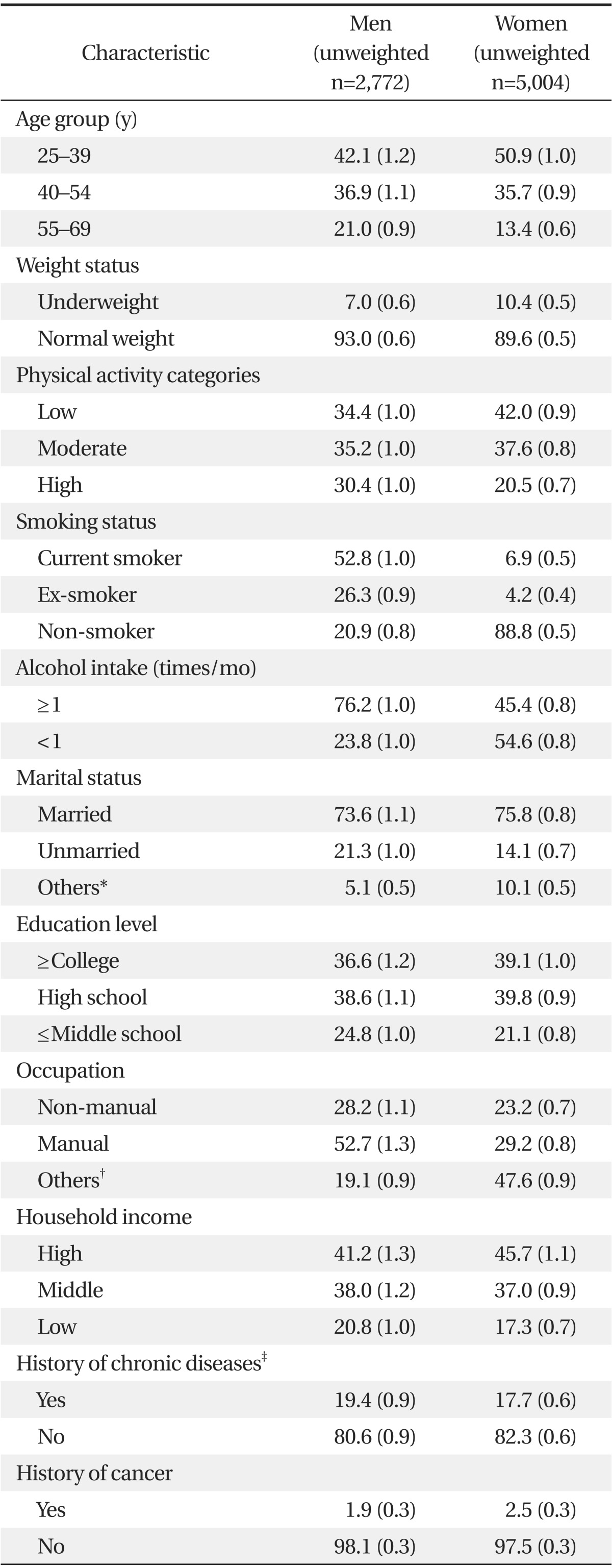
General characteristics of study subjects
We obtained the frequency of underweight in each group stratified by sociodemographic factors. Variables whose P-values were <0.200 from the chi-square tests on either men or women were included as independent variables in logistic regression models (data not shown). After stratification by sex, we performed multiple logistic regression analyses to elucidate the sociodemographic factors that were independently related to underweight. Among men, current smokers (odds ratio [OR], 1.62; 95% confidence interval [CI], 1.01 to 2.62) and those with a history of diagnosis of cancer by a physician (OR, 2.55; 95% CI, 1.10 to 5.90) had a higher likelihood of underweight than non-smokers and those without a history of diagnosis of cancer by a physician, respectively (Table 2). In contrast, among women, subjects aged 25 to 39 years (OR, 2.06; 95% CI, 1.20 to 3.53), ex-smokers (OR, 1.69; 95% CI, 1.03 to 2.78), and unmarried subjects (OR, 1.56; 95% CI, 1.12 to 2.17) had a higher likelihood of underweight than subjects aged 55 to 69 years, non-smokers, and married subjects, respectively (Table 3). In addition, among both men and women, subjects with alcohol intake ≥ 1 times/mo (men OR, 0.57; 95% CI, 0.39 to 0.84; women OR, 0.77; 95% CI, 0.60 to 0.99) and subjects with a history of diagnosis of chronic diseases by a physician (men OR, 0.55; 95% CI, 0.32 to 0.94; women OR, 0.43; 95% CI, 0.28 to 0.66) had a lower frequency of underweight compared to subjects with alcohol intake < 1 time/mo and those without a history of diagnosis of chronic diseases by a physician.
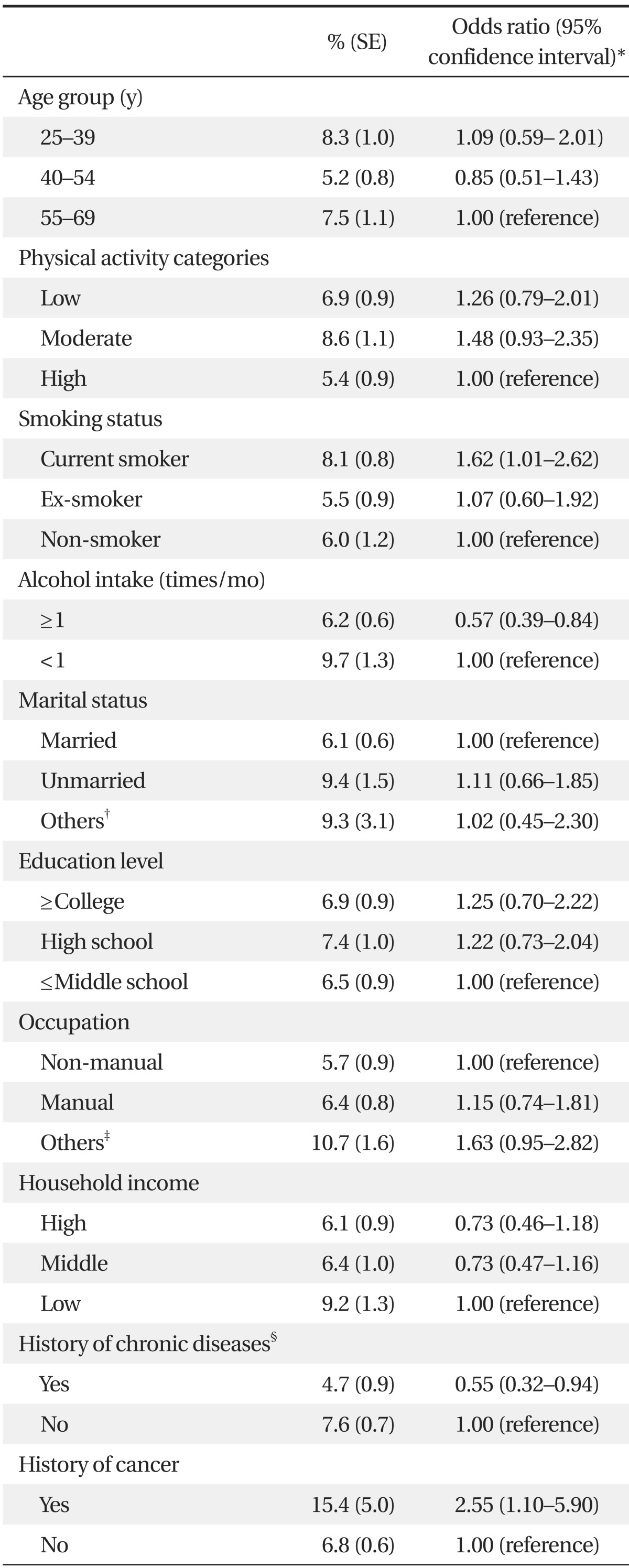
Result of multiple logistic regression analysis on underweight in men
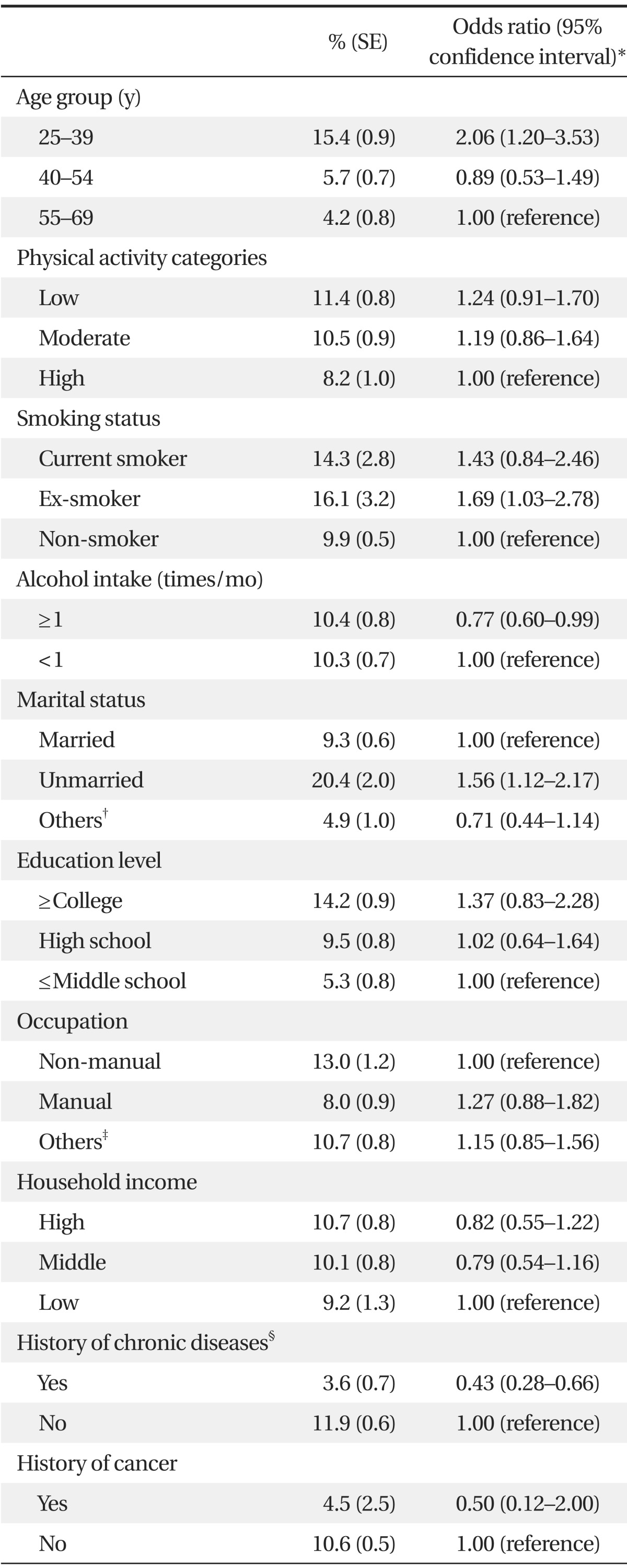
Result of multiple logistic regression analysis on underweight in women
DISCUSSION
The causes of underweight are multifarious and include smoking and underlying diseases, diet and excessive exercise, and eating disorders.12) Different sociodemographic factors can contribute to being underweight between men and women. We ascertained that various sociodemographic factors were associated with underweight depending on sex. Among Korean women, young age, being unmarried, and former smoking were determined as specially related factors of underweight. On the other hand, among Korean men, current smoking and history of cancer were related to underweight. In addition, alcohol drinking and history of chronic diseases were related to a lower frequency of underweight among both men and women. This is the first study, to the best of our knowledge, to investigate sociodemographic factors related to underweight among Korean adults after sex stratification.
Young age and being unmarried were found to be related to underweight only among Korean women. Khang and Yun6) showed that the prevalence of underweight was the highest in women aged 20 to 39 and showed a significant increasing tendency with year between 1998 and 2007 in the same age group of women. Marital status is an important sociodemographic factor that has a strong influence on body weight.13) Vogeltanz-Holm et al.14) reported that being unmarried predicted intense dieting among American women. Jeffery and Rick15) presented that being married was related to increased BMI among both men and women, but the extent of BMI increase was greater in women compared to men (men, +0.70; women, +0.96). Young unmarried persons might expect themselves to appear attractive to potential partners by attaining their ideal body shape. However, ideal body shape is differently perceived between men and women. Women tend to perceive a leaner body shape as ideal compared to men. On the other hand, a good proportion of men want to have a stronger and muscular body.16) This difference in ideal body shape between men and women may be an important cause explaining the finding that young age and being unmarried were related to being underweight only among women in our study. Another idea that could explain the relationship between marriage and weight is that being married may increase the opportunities and cues for eating because married people are likely to eat together.15) In Korean society in which women are mainly responsible for preparation and cooking meals for the family, we think women are more likely to have increased weight after marriage compared to men.
Smoking is considered to be one of the important causes of underweight. It is generally regarded that smoking and relative body weight have an inverse relationship among both men and women.17) In our study, although current smoking was related to underweight among Korean men, ex-smokers had a higher likelihood of underweight than non-smokers among Korean women. In a previous study7) of a Canadian population, the likelihood of current smoking was 33% higher in underweight individuals than in those with acceptable weight. However, the study did not perform sex stratification. We think that more frequent under-reporting of smoking status in Korean women can partly explain the finding that non-current smoking but former smoking is related to underweight. Jung-Choi et al.18) showed that 58.9% of cotinine-verified Korean female smokers responded that they currently do not smoke compared to 12.1% of cotinine-verified Korean male smokers. Women's under-reporting of smoking status in Korean society is related to a cultural background in which women's smoking is stigmatized. The tradition of Confucianism in Korean society is considered a major cause which has brought about social repression of women's smoking. Also, self-reported current female smokers might be less affected by the social pressure than underreporting female smokers. This indicates that self-reported current female smokers remaining in the current smoker category could also be relatively less influenced by other social pressures to be thin compared to under-reporting female smokers who are misclassified as ex-smokers or non-smokers.
Cancer is also considered to be one of the important causes of underweight since cancer is one of the major chronic wasting diseases and can incur weight loss in affected persons. In our study, a past history of cancer was found to be related to underweight only among Korean men. Among Korean women, only 4.5% of women with cancer history were diagnosed as being underweight compared to 10.6% of women without cancer history. Underweight people are a mix of persons who have lost weight because of underlying diseases or smoking, persons who have reduced weight by diet and excessive exercise, and persons with body image distortion because of eating disorders.12) The major underlying cause of underweight could be different between men and women. Underlying diseases like cancer may be chiefly involved in underweight Korean men, but other causes like diet and excessive exercise may have more significant effects on being underweight in Korean women. Presently, a major portion of underweight women were included in the youngest group with the lowest cancer risk. It is also thought that the incidence of each type of cancer is different depending on sex. For example, gastric cancer is known to cause intense weight loss after gastrectomy19) and the incidence of gastric cancer in Korean men is more than twice as high as that in Korean women.20) Thus, different distributions of cancer depending on sex could be implicated in the finding which revealed that the relationship between past history of cancer and being underweight are different between men and women.
It was found in our study that alcohol drinkers and subjects with chronic diseases had a lower frequency of underweight among both men and women. The relationship between alcohol consumption and body weight has not been made clear in previous studies. However, most studies have shown that alcohol drinkers are likely to consume more energy than non-drinkers because alcohol energy is not compensated by decreasing the intake of non-alcohol food energy.21) Son et al.22) presented that alcohol drinkers had a higher intake of total energy and macronutrients except carbohydrates among both Korean men and women. They described that this is related to the fact that alcohol is commonly consumed with fat-rich side dishes such as roasted beef, pork, or eel in Korea. In addition, Sung et al.23) reported that BMI and the prevalence of overweight increased linearly with alcohol intake in Korean men. Furthermore, Sunwoo et al.24) reported that underweight was significantly associated with a low prevalence of alcohol use disorder in Korean adults. The results of our study are congruent with the results of these previous studies in Korea. Excessive adiposity is widely recognized as one of the major risk factors of chronic non-communicable diseases such as hypertension, type 2 diabetes, and cardiovascular diseases.25) However, there has been little epidemiologic research on the possible association between underweight and chronic diseases. It was observed in our study that underweight adults had a less frequent past history of chronic diseases compared to normal-weight adults. It is possible that underweight has a different relationship with each specific chronic disease. Negri et al.26) showed that the prevalence of diabetes, hypertension, and arthritis increased linearly with BMI from underweight to obesity, but chronic respiratory disorders had a U-shaped relationship with BMI. However, we did not evaluate the separate relationship between underweight and each specific chronic disease, which will have to be examined in further studies.
There are several limitations to be considered in our study. Although we used data from a nationwide representative survey, it is difficult to establish causal and sequential relationships because of the nature of the cross-sectional design of this study. Since health behaviors and history of morbidity were assessed only by questionnaires, this study can have problems related to reporting bias. For example, we think that under-reporting of smoking in women affected the results of this study. We did not evaluate the relationship of underweight with a past history of each specific cancer or chronic disease. A further study is required to determine how underweight is related to each specific cancer or chronic disease. In spite of these limitations, we presented the sociodemographic factors that are independently related to being underweight among Korean adults after sex stratification.
Underweight people are composed of heterogeneous groups including persons who have lost weight because of underlying diseases or smoking, persons who have reduced weight by diet and excessive exercise, and persons who have body image distortion because of an eating disorder. Underweight people may have different characteristics depending on the underlying causes. We observed that young age, being unmarried, and former smoking were related to underweight among Korean women, whereas current smoking and past history of cancer were related factors of underweight among Korean men. In addition, alcohol drinking and past history of chronic disease were factors related to a lower frequency of underweight among both men and women in this study. It was ascertained that the sociodemographic factors related to underweight differed between Korean men and women.
Notes
No potential conflict of interest relevant to this article was reported.