INTRODUCTION
Metabolic syndrome is a combination of metabolic risk factors and increases the risk of heart attack or stroke and the mortality from related diseases such as diabetes and hypertension.1,2) The prevalence of metabolic syndrome has been increasing worldwide over the past few years.3) According to the Korea National Health and Nutrition Examination Survey, the prevalence of metabolic syndrome in Korea was 24.1% in 2005.4)
There have been many studies on the relationship between drinking and metabolic syndrome. It was reported that heavy drinking increases the risk of metabolic syndrome.5) On the other hand, moderate drinking is reported to lower the risk of metabolic syndrome.6) But there have been few studies on the relationship between the intensity of drinking and metabolic syndrome. In terms of the distinction between frequent drinking of smaller quantities of alcohol versus occasional drinking of large quantities of alcohol, it has not been reported which increases the risk of metabolic syndrome more.
The level of alcohol consumption per person in Korea was 8.1 L per year in 2005, lower than Organization for Economic Cooperation and Development average of 9.5 L per year.7) However, Korea has the highest rate of binge drinking (defined as drinking more than five glasses at once) among the countries that provided data on global alcohol drinking patterns published by the World Health Organization (WHO) in 2005.8) Therefore, the authors aimed to investigate the relationship between the quantity of alcohol consumed per drinking episode and metabolic syndrome in Korean adult men.
METHODS
1. Subjects
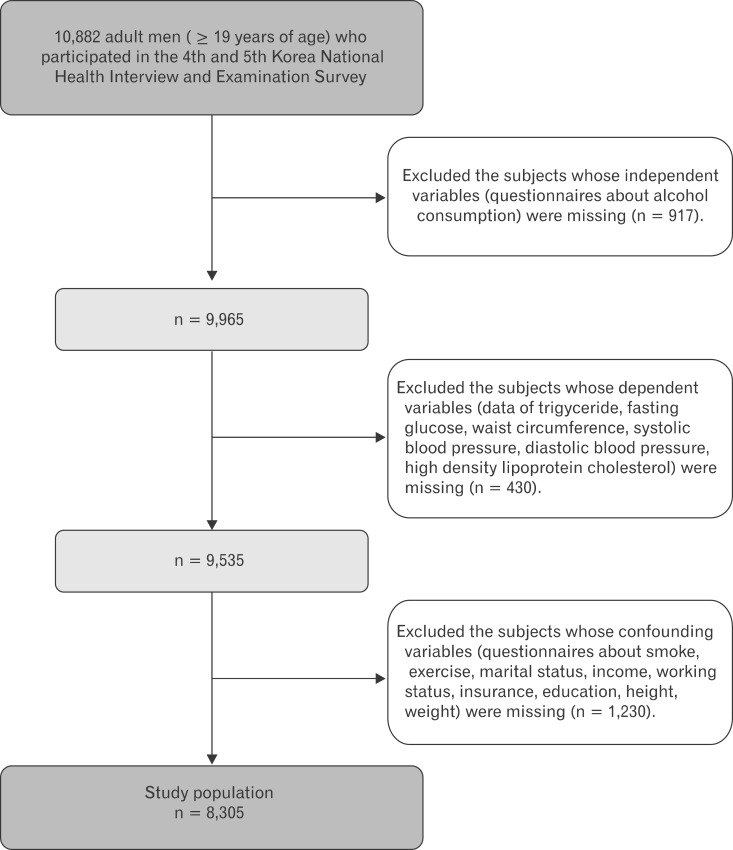
From the database of the 4th and 5th Korea National Health and Nutrition Examination Survey (KNHANES) conducted in 2007-2010, data of 10,882 adult men (≥19 years of age) was included in this analysis. We excluded the subjects whose independent variables (the questionnaires about alcohol consumption) were missing (n = 917). We also excluded the subjects whose dependent variables (data of triglyceride, fasting glucose, waist circumference, systolic blood Pressure, diastolic blood pressure, high density lipoprotein [HDL] cholesterol) were missing (n = 430) and the subjects whose confounding variables (questionnaires about smoking, exercise, marital status, income, working status, insurance, education, height, weight) were missing (n = 1,230). Following these exclusions, we included 8,305 subjects in the analysis.
2. Demographic and Socioeconomic Factors
We collected data on the demographic factors and health behaviors of the subjects. The demographic variables were age, sex, educational level (elementary school or less, middle school, high school, and college or more), working status (active, inactive), marital status (married, separated/widowed/divorced, single), insurance status (national health insurance, medical aid), and monthly income (<1 thousand won/mo, ≥1 thousand won/mo and <3 thousand won/mo, ≥3 thousand won/mo). The health behavioral variables included smoking (non-smoker, exsmoker, smoker), exercise (low, moderate, or high by tertiles of metabolic equivalent of task minutes per week). The Korean version of the International Physical Activity Questionnaire short form was used to calculate the metabolic equivalent of task minutes per week (MET-minutes per week).9) Then we classified the subjects into 3 exercise groups by tertiles of MET-minutes per week.
3. Assessment of Drinking
We calculated pure alcohol consumed per day using the database of the Korea National Health and Nutrition Examination Survey. We used the data of the frequency of drinking in the last 1 year and glasses of alcohol per drinking. Then we classified the subjects into nonconsumer (<1 g/d), light consumer (1-14.9 g/d), moderate consumer (15-29.9 g/d), and heavy consumer (≥30 g/d) groups.10)
WHO defined high risk drinking as drinking over 60 g of pure alcohol a day for men, and 40 g of pure alcohol a day for women.11) According to this definition, binge drinking is defined as drinking more than 7 glasses of alcohol for men in the Korea National Health and Nutrition Examination Survey.
We grouped subjects into a non-binge drinking group and a binge drinking group. Then we classified the binge drinking group by the frequency of binge drinking according to the questionnaires of the Korea National Health and Nutrition Examination Survey (lower = about 1/mo or less, higher = more than 1/wk).
4. Anthropometric Measures
Body weight and height were measured using standard protocols to the nearest 0.1 kg and 0.1 cm, respectively. Waist circumference was measured at the narrowest point between the lower borders of the rib cage and the uppermost borders of the iliac crest at the end of normal expiration. Blood pressure was measured with a mercury sphygmomanometer.
5. Laboratory Evaluation
Antecubital vein blood samples were drawn and centrifuged after fasting (fasting time ≥12 h). These blood samples were used to evaluate total cholesterol, HDL cholesterol, triglyceride, and glucose levels.
6. Definition of Metabolic Syndrome
We defined metabolic syndrome according to National Cholesterol Education Program's Adult Treatment Panel III revised in 2005 (meeting more than 3 of following criteria):12) 1) abdominal obesity: waist circumference ≥ 90 cm;13) 2) high blood pressure: systolic blood pressure ≥130 mm Hg or diastolic blood pressure ≥ 85 mm Hg or taking hypertension medication; 3) fasting hyperglycemia: fasting blood sugar ≥ 100 mg/dL or taking diabetes medication or insulin therapy; 4) hypertriglyceridemia: triglyceride ≥ 150 mg/dL or taking dyslipidemia medication; 5) low HDL cholesterol: HDL cholesterol ≤ 40 mg/dL or taking dyslipidemia medication.
We grouped those who take dyslipidemia medication into a hypertriglyceridemia group and low HDL cholesterol group. And we grouped those who take diabetes medication or insulin into a fasting hyperglycemia group, and those who take hypertension medication into a high blood pressure group.
7. Analysis
We examined the characteristics of the subjects by t-test (continuous variable) and by chi-square test (categorical variable). We used multiple logistic regression analysis to examine the relationship between the frequency of binge drinking and metabolic syndrome and each component of metabolic syndrome. We examined the adjusted odds ratios and 95% confidence intervals adjusting for age in model 1. In model 2, smoking status, pure alcohol consumed per day, exercise, insurance status, education, working status, marital status, and monthly income were adjusted for in addition to model 1. In model 3, body mass index was adjusted in addition to model 2. We divided subjects into 3 groups including a non-binge drinking group, a lower binge drinking group, and a higher binge drinking group, and divided each group into 4 subgroups by pure alcohol consumed per day. Adjusting for age, smoking status, exercise, insurance status, education, working status, marital status, and monthly income, we examined the adjusted odds ratio for metabolic syndrome in those in each of the 11 subgroups compared to those in the non-binge drinking and nonconsumer subgroups. Reported probability values were 2-sided and a P-value < 0.05 was considered statistically significant. Stata SE ver. 12.0 (Stata Co., College Station, TX, USA) was used in all statistical analysis with 'svy' commands to account for complex sampling design, and included sampling weights, which enabled the results to represent the entire population of adult men.
RESULTS
1. Characteristics of Subjects
As demonstrated in Figure 1, final study population were 8,305 men. Subjects who had higher frequency of binge drinking had higher body mass index, waist circumference, triglyceride, HDL cholesterol, systolic blood pressure, diastolic blood pressure, fasting glucose, pure alcohol consumed per day, and statistically significant. Age, hypertension, diabetes, dyslipidemia treatment, smoking status, exercise, marital status, education, working status, monthly income, and insurance status were different between groups and statistically significant (Table 1).
2. The Risk of Metabolic Syndrome According to the Frequency of Binge Drinking
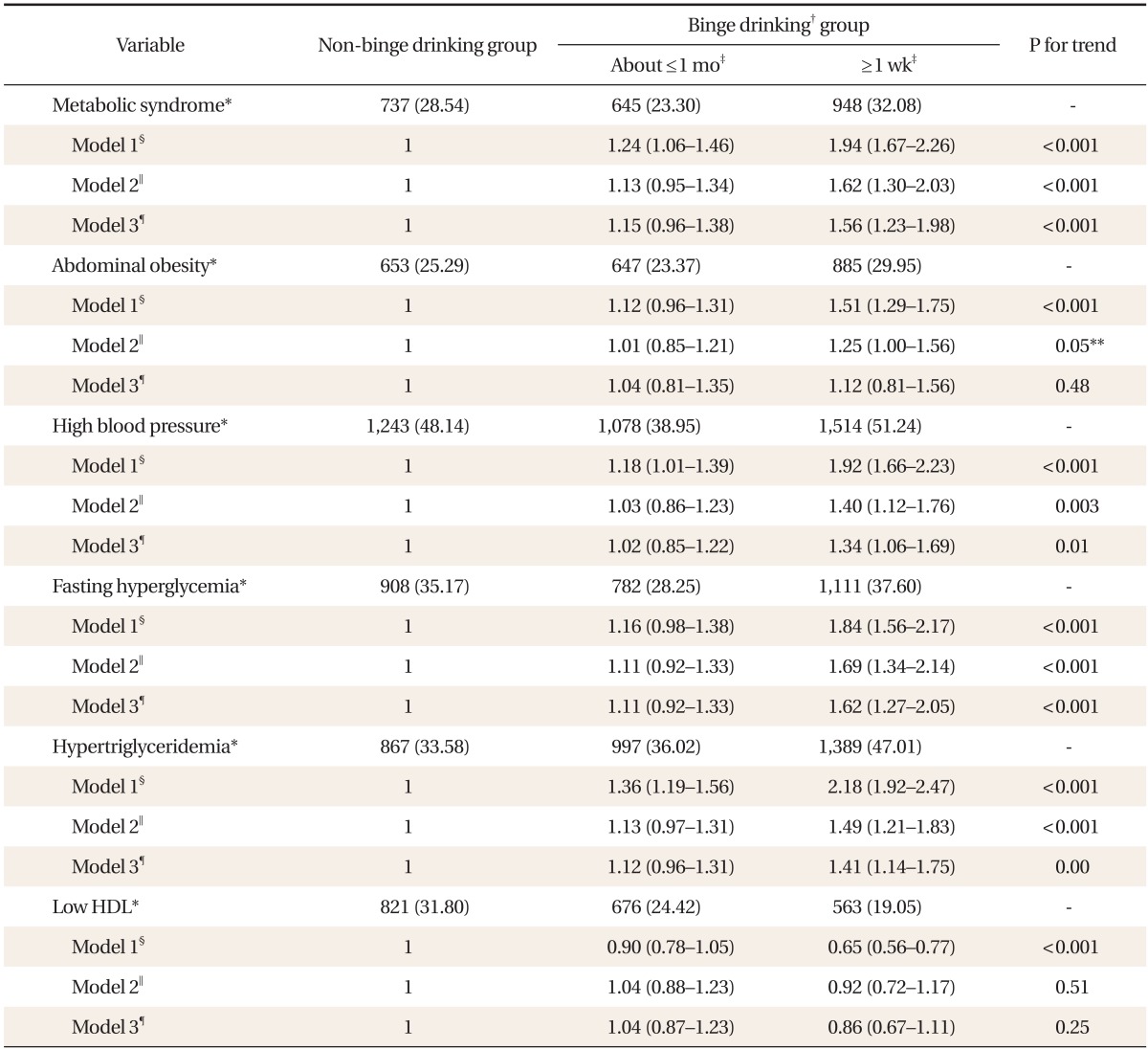
Table 2 presents the results. In model 1, the adjusted odds ratio for metabolic syndrome in those who had higher frequency (more than 1/wk) of binge drinking was 1.94 (95% confidence interval [CI], 1.67 to 2.26; P for trend = <0.001). In model 2, the adjusted odds ratio for metabolic syndrome in those who had a higher frequency (more than 1/wk) of binge drinking was 1.62 (95% CI, 1.30 to 2.03; P for trend = <0.001). Among the components of metabolic syndrome, abdominal obesity, high blood pressure, fasting hyperglycemia, hypertriglyceridemia had a positive association with the frequency of binge drinking (P for trend = 0.048, 0.003, <0.001, <0.001, respectively). In model 3, the adjusted odds ratio for metabolic syndrome in those who had higher frequency (than 1/wk) of binge drinking was 1.56 (95% CI, 1.23 to 1.98; P for trend = <0.001). Among the components of metabolic syndrome, high blood pressure, fasting hyperglycemia, and hypertriglyceridemia had a positive association with the frequency of binge drinking (P for trend = 0.012, <0.001, 0.001, respectively).
3. The Risk of Metabolic Syndrome According to the Frequency of Binge Drinking and Daily Pure Alcohol Consumed per Day
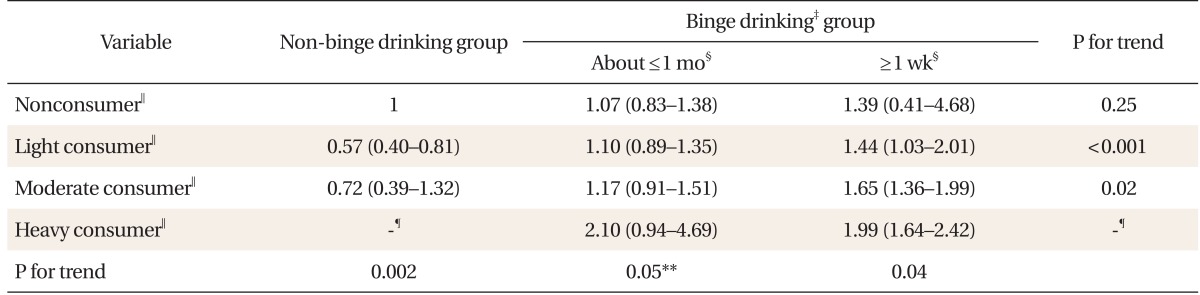
We examined the adjusted odds ratio for metabolic syndrome in those in each subgroup of the frequency of binge drinking and pure alcohol consumed per day. Table 3 presents the results. We could not calculate the odds ratio in those in the non-binge drinking and heavy consumer groups, because there were only 2 subjects in the subgroups. In each group of light consumer and moderate consumer, the frequency of binge drinking had a positive association with metabolic syndrome (P for trend = <0.001, 0.018, respectively). In the heavy consumer group, the odds ratio for metabolic syndrome was 2.10 (95% CI, 0.94 to 4.69) in the lower binge drinking group, and the odds ratio was 1.99 (95% CI, 1.64 to 2.42) in the higher binge drinking group. In the higher frequency binge drinking group, pure alcohol consumed per day had a positive association with metabolic syndrome (P for trend = 0.041). In the non-binge drinking group, light consumers had a lower risk for metabolic syndrome compared to nonconsumers or moderate consumers.
DISCUSSION
We found that the frequency of binge drinking is positively associated with metabolic syndrome in adult men after adjusting for pure alcohol consumed per day and other possible confounding factors. We also found that pure alcohol consumed per day was positively associated with a higher risk of metabolic syndrome in the higher frequency binge drinking group, while an inverse association was observed in the non-binge drinking group. In other words, the effect of drinking on metabolic syndrome may depend on the frequency of binge drinking.
Another study was conducted to examine the relationship between the intensity of alcohol drinking and metabolic syndrome.14) In that study, the intensity of drinking had a linear relationship with fasting hyperglycemia and hypertriglyceridemia. But the association was not independent of the total amount of drinking. Thus, there was a methodological difference with our study.
It is well recognized that heavy drinking increases the risk of high blood pressure and high triglyceride and metabolic syndrome.5,7,15) Moderate drinking is reported to lower the risk of metabolic syndrome.11) The relationship between drinking and metabolic syndrome may be a J-shape.16) There have been few studies examining the relationship between drinking and cardiovascular disease which also consider binge drinking. Interestingly, in our study, pure alcohol consumed per day had a protective effect on metabolic syndrome in the non-binge drinking group. In addition, in the highest binge drinking group, pure alcohol consumed per day had a positive association with metabolic syndrome, suggesting that not only the amount of alcohol consumed but also binge drinking is associated with cardiovascular disease.
Alcohol affects the onset of metabolic syndrome in various ways. Alcohol suppresses lipid oxidation from adipose tissue and enhances fat deposition, preferentially in the abdominal area, and can lead to increases triglyceride in the blood stream.17) It is reported that heavy drinking causes enhancement of insulin resistance and type 2 diabetes.18) And it is suggested that repeated drinking and withdrawal symptoms increases the risk of hypertention.19,20) On the other hand, alcohol suppresses the removal of HDL cholesterol in the blood stream, and reduces vitality and concentration of CETP (cholesterol ester transfer protein) thus decreasing the transformation of HDL of cholesterol ester to materials causing atherosclerosis.7,21) These effects are not fully understood and need further investigation. We can only suggest that these effects are intensified when drinking over a certain amount of alcohol at one time. as Another mechanism may be at work, as reported in one study in which binge drinking induced insulin resistance by disrupting hypothalamic insulin action in rats,22) suggesting that the same mechanism may be at work in humans. More studies are required to examine the underlying mechanism.
Our Study has some limitations. First, daily food intake is reported to be significantly associated with metabolic syndrome. However, the questionnaire about food intake on the KNHANES was a single 24-hour dietary recall which is not an optimal way to assess daily food intake. We did not adjust for daily food intake using that data. Second, the cross-sectional nature of this study prevented us from determining an exact cause-and-effect relationship. Third, with regard to definition of binge drinking, an error may have occurred due to indirect measurement. But the cause-effect relationship between alcohol drinking and metabolic syndrome is already recognized. In spite of these limitations, our study is important since it is the first study to examine the relationship between the intensity of alcohol drinking and metabolic syndrome after adjusting for several confounders including pure alcohol consumed per day in Korea.
In conclusion, our study found a significant relationship between the frequency of binge drinking and metabolic syndrome in adult men. And the effect of drinking on metabolic syndrome may depend on the frequency of binge drinking. Further studies are required to confirm this association.