INTRODUCTION
Nutrition labels provide the information on the main nutrients and their quantities in foods. In general, nutrition labels show the nutrient content of one serving of food and give a comparison with the daily recommended intake in a specific format. Nutrition labels have been made mandatory for almost all processed foods in the US and Canada for many years.1,2) In Korea, nutrition labels show the contents of nine nutrients, including energy, carbohydrates, sugars, proteins, fats, saturated fats, trans fats, cholesterol, and sodium as per the regulations.1,3)
According to 'Nutrition labels and health claims: the global regulatory environment' published by World Health Organization (WHO) in 2004, the information on the nutrient content and their health promotion effect of processed foods are particularly important, and nutrition labels are useful tools to deliver this information.2) Consumers read nutrition labels to compare different foods and to obtain information on negative characteristics of foods such as fat, calories, and sodium content.4,5) Nutrition labels are becoming more important as useful tools that help users choose the appropriate foods for health management. The US Food and Drug Administration estimated in 1993 that the introduction of mandatory nutrition labeling would led to prevention of 39,200 cases of cardiovascular disease and cancer, and 12,902 cases of death for the next 20 years, leading to a national benefit of 4.4 to 22 billion dollars.6)
Previous studies on factors that affect the use of nutrition labels have shown that females, and those of higher income and education level tend to read nutrition labels more frequently.7,8,9) Similarly, analyses of data from the 2007-2008 Korea National Health and Nutrition Examination Survey (KNHANES) have shown that those with higher household income and education level were more likely to read nutrition labels.10) A number of other studies have also looked into the association between the use of nutrition labels and the actual pattern of nutrient intake, some of which have shown that those who read nutrition labels tended to consume less calories and fats, and more fruits, vegetables and fiber.8,9,11,12,13) On the other hand, a study by Harnack et al.14) showed that there was no difference in the intake of calories between those who ordered from a fast food restaurant menu with the energy content displayed, and those who ordered from menus without. Elbel el al.15) compared the difference in calories, saturated fat, sodium, and sugar content of foods ordered from fast food restaurants in selected areas of New York before and after the introduction of mandatory display of nutrition information on the menus. In a systematic review published in 2011, only 2 out of the 7 studies published between 2008 and 2011 showed an actual decrease in the intake of calories by displaying calories, and overall it was concluded that there was insufficient evidence that caloric intake was reduced.16)
Considering the fact that the main aim of nutrition labels is to promote healthy eating, it is important to compare the differences in diet habits due to nutrition label reading. Yet, there are limited studies in Korea that look into this effect in adults, except a few studies that were done on the use of nutrition labels and dietary habits in youth.17,18,19,20) Therefore the aim of this study was to investigate the association between the use of nutrition labels and eating habits using the KNHANES data.
METHODS
1. Subjects
This study was based on data from the fourth KNHANES (2007-2009). KNHANES is a national project that was started in 1998 that targets all households and citizens living in the Republic of Korea to investigate the population's health status, health awareness and actions, and food and nutrition intake. The subjects were selected using a 3-step stratified cluster sampling method from the Population and Housing Census Report. A trained investigator visited each household to complete the questionnaires orally. In the fourth KNHANES, 24,871 out of 31,705 participated, resulting in a participation rate of 78.4%. Of the 24,871 participants, we excluded 6,661 under the age of 20. We also excluded 2,183 people who did not respond to the question on the use of nutrition labels, and 2,103 people who did not respond to the question on sociodemographic factors that were found to be associated with the use of nutrition labels, resulting in a final study population of 13,924 people.
2. Study Variables
The sociodemographic factors associated with nutrition label reading used in this study were gender, age, body mass index (BMI), marital status (single, divorced or separated, married), education level (under middle school, middle school graduate, high school graduate, university graduate), household income, number of family members (1-2 persons, more than 3 persons), subjective perception of body figure (thin, average, obese), smoking status (non-smoker, ex-smoker, current smoker), and alcohol use frequency (less than once per month, twice per month to once weekly, twice weekly or more), as per previous studies.9,10) The presence of chronic diseases such as hypertension, diabetes, and dyslipidemia were assessed using the response to the question on the presence of chronic disease.
The use of nutrition label was assessed using responses 'yes' or 'no' to the question 'Do you read nutrition labels when purchasing or choosing processed foods?' All those that did not respond to this question or answered 'I don't know' were excluded from analysis.
3. Diet Assessment
Evaluation of nutrition intake was performed using the daily nutrient intake data collected by 24-hour recall in KNHANES. Nutrients included in analyses were the calories, macronutrient (carbohydrates, proteins, fat) intake and energy ratio, fiber, sodium, potassium, vitamin A, carotene, retinol, and vitamin C. The recommended intake of nutrients was set by the nutrition guidelines published by WHO and the 2010 Dietary Reference Intakes for Koreans by Korean Nutrition Society. The recommended daily intake of sodium was under 2 g, at least 3,500 mg for potassium, at least 700 mg of calcium, and at least 20 g of fiber. The recommended intake of fat was under 25% and 30% of total energy intake.
4. Statistical Analysis
The subjects were divided into two groups depending on whether or not they read nutrition labels. The differences in variables including the age, gender, BMI, marital status, education level, household income, number of family members, subjective perception of body figure, smoking status, alcohol use, nutrition education, presence of hypertension, diabetes, or dyslipidemia were then analyzed using t-test and chi-square test. We confirmed that stratified gender analysis was possible using Mantel-Haenszel test for homogeneity and the subjects were subsequently analyzed for each gender. After correcting for variables that affect nutrition label reading, analysis of covariance was performed to compare the intake of individual nutrients between those who read nutrition labels and those who do not. Then multiple logistic regression analysis was performed to calculate and evaluate the odds ratio (OR) and 95% confidence interval (CI) of the adherence to recommended daily intake of nutrients with nutrition label reading. In order to represent all Korean adults without biased estimates, sampling weights were applied to account for the complex sampling. Statistical analysis was done using Stata ver. 12.0 (Stata Co., College Station, TX, USA) and P-values of 0.05 or less were taken to have statistical significance.
RESULTS
1. General Characteristics of the Subjects
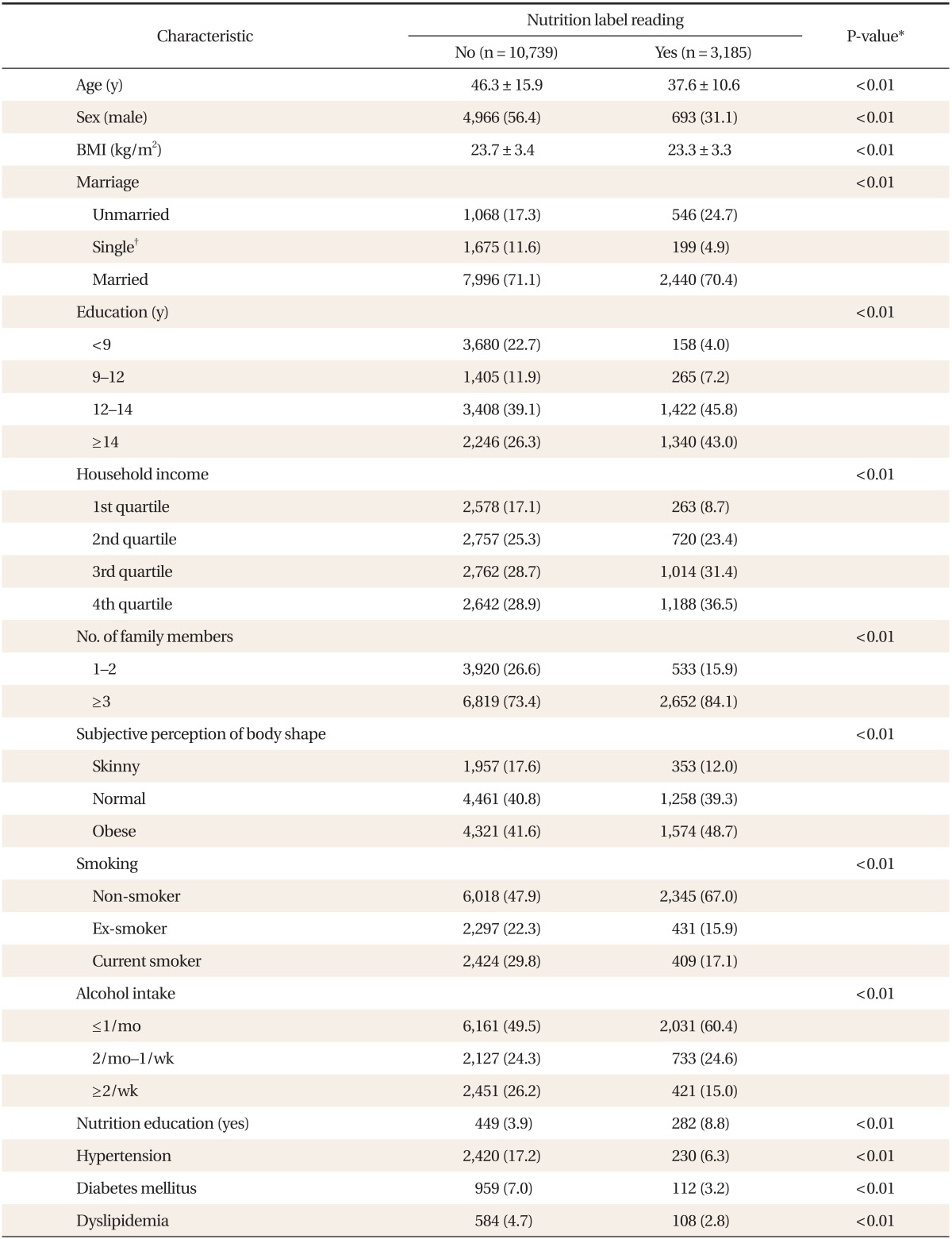
The subjects were divided into two groups depending on whether or not they read nutrition labels, and the differences in these two groups were analyzed (Table 1). Of all 13,924 subjects, 3,185 (24.7%) were nutrition label readers, of which 693 (12.2%) were male and 2,492 (30.2%) were female. The mean age of the nutrition label readers was 37.6 years, whereas that of non-readers was 46.3 years. The percentage of males of nutrition label users was 31.1% versus 56.4% in non-readers of nutrition labels. The education level and household income were both higher in the nutrition label readers. Those who had more than 3 persons in their family were more likely to read nutrition labels than those from smaller families of 1 to 2 members. Those who perceived themselves as being obese subjectively were also more likely to read nutrition labels. There were more non-smokers and a smaller percentage of people who drank alcohol 2 or more times each week in nutrition label readers. Those who had previously received nutrition education tended to read nutrition labels more, and there were more people with chronic diseases such as hypertension, diabetes and dyslipidemia in non-readers.
2. Nutrient Intake and the Use of Nutrition Labels
Multiple linear regression analysis was done to investigate the intake of nutrients depending on the use of nutrition labels (Table 2). In men, those who read nutrition labels had higher intake of calcium (534.8 mg vs. 576.1 mg, P = 0.015) and vitamin C (106.3 mg vs. 117.2 mg, P = 0.022) compared to those who did not read nutrition labels. The calorie intake, carbohydrates, proteins, fat intake and energy ratio, fiber, sodium, potassium, vitamin A, carotene, and retinol was not different between the two groups. In women, the calorie (1,585.4 kcal vs. 1,536.8 kcal, P = 0.013) and carbohydrates (275.2 g vs. 267.1 g, P = 0.016) intake was lower in those who read nutrition labels, with higher intake of protein (13.9% vs. 14.3%, P < 0.01). There was no significant difference in the fat intake and energy ratio, fiber, sodium, potassium, calcium, vitamin A, carotene, retinol, and vitamin C between users and non-users of nutrition labels.
3. Association between the Use of Nutrition Labels and the Adherence to Recommended Intake of Major Nutrients
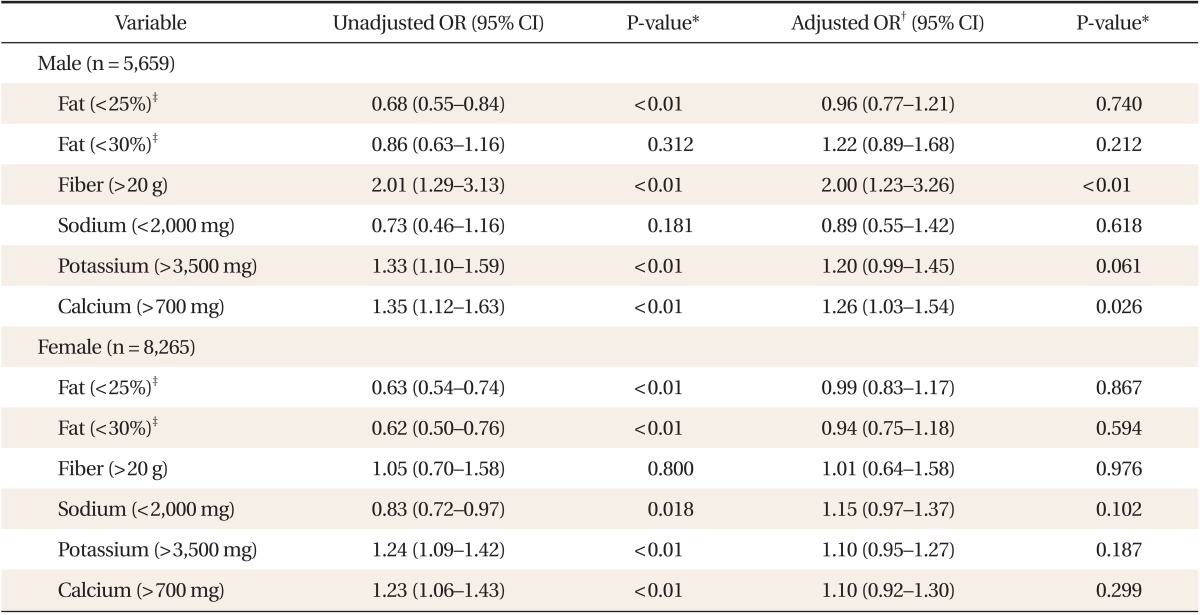
To investigate the association between the use of nutrition labels and the adherence to recommended intake of major nutrients such as fat, fiber, sodium, potassium, and calcium, we conducted multiple logistic regression analysis (Table 3). In men, nutrition label readers were found to follow the recommended fiber intake of 20 g or more (OR, 2.00; 95% CI, 1.23 to 3.26) and recommended calcium intake of 700 mg or more (OR, 1.26; 95% CI, 1.03 to 1.54), with no difference in the adherence to recommended intake of fat, sodium, and potassium. However in women, there was no difference in the adherence to recommended intake of fats, fiber, sodium, potassium, and calcium depending on the use of nutrition labels.
DISCUSSION
In this study, nutrition label users were found to be relatively younger, have higher proportion of females, higher level of education and income, and higher number of family members compared to non-users of nutrition labels. In men, nutrition label users had higher intake of calcium and vitamin C compared to non-users. In women, the total intake of calories and carbohydrates was lower in nutrition label users, with higher energy ratio of protein, although there was no difference in the intake of other micronutrients. In men, nutrition label readers were more likely to adhere to the recommended intake of fiber and calcium, but not fat, sodium and potassium, whereas in women, the use of nutrition labels did not affect the adherence to the recommended intake of any nutrients.
Similar to previous findings, this study also showed that younger people and women were more likely to read nutrition labels.9,10) This seems to be due to having different opportunities to receive nutrition education or information on nutrition labels according to gender and age group. The different preferences of processed foods, which have nutrition labels, may also have affected the results. Women tend to show higher interest in dietary habits than men, and the gender differences may also be reflecting the role of married women who generally look after the diet of the family. Similar to previous findings, we also found that those with higher level of education and income were more likely to read nutrition labels. This is likely to be due to these people having higher interest in health, maintaining a healthy diet, and thus showing more interest in nutrition labels when choosing foods. We also found that those who subjectively perceived themselves as being obese were more likely to read nutrition labels, which is likely to be due to their increased interest in calories and nutrition intake.
Previous studies on the association between the nutrition label use and the intake of nutrients have shown different results according to study subjects and method. A study done in university students in the US showed that those who read nutrition labels had higher intake of fruits, vegetables, and fiber.13) A study which analyzed data from Continuing Survey of Food Intakes by Individuals and Diet and Health Knowledge Survey of the US showed that the use of nutrition labels was associated with higher vitamin C intake and lower cholesterol intake.21) On the other hand, a study that compared nutrition intake before and after displaying the nutrients on fast food menus in New York showed that although subjects answered that their choice from the menu was affected by nutrition labels, their actual intake of calories, saturated fats, sodium, and sugar was not different.15) A systemic review of previous studies on the effect of displaying caloric content and the intake of calories reported that only 2 of the 7 studies published between 2008 and 2011 showed an actual decrease in calories by caloric content display.16) This difference may be due to different study designs and populations, as some studies were done in adolescent populations and there were differences in cities, income level, and fast food restaurants.
It is likely that nutrition label readers would have higher interest in healthy diets compared to non-readers. However, there was no difference in the intake of antioxidants such as vitamin A, retinol, and carotene as well as sodium intake between readers and non-readers of nutrition labels in both genders. It is well known that high sodium intake is associated with increased risks of chronic disease such as hypertension, stroke, and cardiovascular disease,22) and WHO recommends a daily intake of more than 2.5 g of potassium and under 2 g of sodium. The same recommended amount of sodium is used in Korea, although according to the 2011 KNHANES, the average sodium intake of Koreans is more than double of this, at 4.9 g per day. The adverse effect of sodium was well recognized, and other countries have made efforts to reduce salt intake at a national level. For example, a national campaign to reduce the sodium intake in UK led to a successful reduction in sodium intake by 10%. Similar successful sodium reduction has been achieved in Japan, Finland, and Ireland.23,24) There have been recent movements in Korea to reduce sodium intake, but there are still limitations such as the diet tradition of salted foods and eating soups with meals, and increased consumption of processed foods. Sodium intake is also different in men and women. According to 2010 KNHANES, the percentage of sodium intake relative to the recommended daily intake of 2 g per day was 403% in men and 289% in women, showing that men were consuming much more sodium than women. In this study, men also showed higher sodium consumption, but there was no difference in sodium intake and the adherence to recommended intake of sodium according to nutrition label use in both genders.
Our study showed that in men, nutrition label users had higher calcium intake and were more likely to adhere to the recommended intake, although this was not observed in women. Calcium deficiency affects bone metabolism and thus increases the risk of osteoporosis and fractures in women.25,26) There have also been reports of calcium deficiency and its association with diabetes27) and colorectal disease.28) Calcium intake is important in the aging population, but it is also one of the most deficient nutrients in Koreans for all ages and genders. The recommended calcium intake in the US is 1,000 to 1,200 mg, whereas the recommended intake is 650 to 750 mg in Korean adults. However, according to the 2010 KNHANES, the average calcium intake was 529 mg, with the percentage of recommended intake of 79% in men and 69% in women, showing that women had relatively lower calcium intake than men.
In this study, only 24.7% of the subjects responded that they read nutrition labels. If the rate of nutrition label use was higher, the intake of other micronutrients may have been significantly different between nutrition label readers and non-readers. Nevertheless, the fact that the use of nutrition labels (where the majority of nutrition label users were young with high socioeconomic status) was not associated with the intake of important nutrients for Koreans shows that the current nutrition labeling policy does not have a significant effect on the vulnerable nutrients. However, we should note that only processed foods have nutrition labels. The majority of foods do not have nutrition labels, which means that even though a person chooses foods based on nutrition labels it would only have a small effect on the overall nutrient intake. However, if the nutrition labeling policy is changed so that the important nutrients such as sodium and calcium are emphasized and their effect on health is displayed, it may lead to changes in the overall pattern of food intake.1)
There are several limitations of this study. Firstly, this is a cross-sectional study which means that it cannot explain the causal relationship between the use of nutrition labels and the actual nutrient intake. The use of nutrition labels may affect diet patterns, but on the other hand, those who have more interest in health and have healthier dietary habits may be more likely to read nutrition labels. A number of studies done overseas have shown that the display of nutrition information on restaurant menus have effects on the selection and consumption of foods by consumers,11,15) although this has not been studied in depth in Korea. Secondly, the 24-hour recall that we used to evaluate the consumption of nutrients is limited in that it cannot reflect long-term dietary habits.29) This can be addressed by using a food frequency questionnaire, which will need to be developed and adjusted to fit the purpose of the study. Thirdly, the use of nutrition labeling was determined by self-response questionnaires, and hence may be prone to recall bias.
However this study is important in that it has used data that represents the adult population in Korea to confirm the association between the use of nutrition labels and actual nutrient intake, in a setting of limited domestic studies on the use of nutrition labels. The results of this study will need to be confirmed with further studies on the effects of nutrition labeling on nutrient intake.