Relationship of Simple Renal Cyst to Hypertension
Article information
Abstract
Background
Simple renal cyst is the most common cystic deformation found in adults. However, there were a few systematic Korean reports for the clinical symptoms and complications of simple renal cysts. The author's purpose was to determine the relationship between simple renal cysts diagnosed by abdominal ultrasonography and hypertension.
Methods
Among 13,482 persons who took a routine physical examination at Ulsan University Hospital in 2002, 5,127 persons who took medical examinations again in 2010 were selected. We excluded persons who had renal cyst, hypertension, diabetes, liver cirrhosis, kidney disease, thyroid disease, and cancer in 2002. Analysis was conducted for 505 subjects with newly diagnosed simple renal cyst and 2,744 subjects without renal cyst in 2010. The simple renal cyst group was compared to a control group without renal cyst.
Results
Among 3,249 subjects, simple renal cyst and hypertension were newly diagnosed in 505 subjects and 503 subjects. The subjects who had simple renal cysts had significantly higher hypertension incidence (odds ratio [OR], 1.53; 95% confidence interval [CI], 1.20 to 1.94). Significant hypertension incidence was observed especially when the subjects had cysts located on both kidneys (OR, 3.48; 95% CI, 2.12 to 5.71), two (OR, 3.08; 95% CI, 1.84 to 5.15) or more cysts (OR, 3.12; 95% CI, 1.38 to 7.04), and larger cysts more than 1 cm in diameter (OR, 1.55; 95% CI, 1.16 to 2.07).
Conclusion
The presence of simple renal cysts was significantly positively related to the incidence of hypertension. Bilateral distribution, two or more number, and larger size than 1 cm diameter were the characteristics of simple renal cyst related to hypertension.
INTRODUCTION
Simple renal cyst consists of 70% of all asymptomatic kidney tumors which can be found in all age groups but its prevalence increases with age, more than 5% in age of 40's and 36% in 80's and is often diagnosed as an incidental findings.1,2,3) There are limited numbers of systematic study reports about clinical manifestations and natural history of simple renal cysts due to its rare progression to clinically significant complications. And most reported studies are of limited value because they are either cross-sectional or Target a small population.1,2,3,4)
Hypertension is one of the most common chronic diseases and in 2013 the World Health Organization reported that about 40% of the population over 25 years of age has been diagnosed with hypertension worldwide. The number of people diagnosed with hypertension worldwide has increased dramatically from 6 million in 1980 to 1 billion in 2008, and among 17 million deaths caused by cardiovascular disease every year, 9.4 million deaths are estimated to be hypertension related.5) The Korean National Health and Nutrition Examination Survey (KNHANES) in 2011 reported that prevalence of hypertension those over 30 years of age was 28.5%, a 3.9% increase from 24.6% in 2007.
The second most common cause of death in Korea was cardiovascular disease, accounting for 19.5% of all causes in 2012. The importance of prevention and treatment of hypertension can easily be presumed from the above facts in terms of both individual and national health.6)
The relationship between simple renal cysts and hypertension has been reported by many studies,7,8,9,10,11,12) but Al-Said et al.13) reported simple renal cysts and its association with kidney dysfunction but not hypertension. The controversy over the relationship between simple renal cyst and hypertension is ongoing and most studies conclude further examination and studies are needed. This study aims to examine newly diagnosed simple renal cyst and its relation to diagnosis of hypertension during 8 years of study.
METHODS
1. Subjects
Among 13,482 people who underwent general physical examination at Ulsan University Hospital from March to December 2002, 5,127 people who returned for another physical examination between March and December 2010 were initially selected. From the initial selections, 275 subjects with simple renal cyst, 340 subjects with diabetes, 1,260 with hypertension, 31 with liver cirrhosis, 52 with thyroid disease, 2 cancer patients, and 1 patient with kidney disease diagnosed by 2002 were excluded along with 542 subjects with insufficient information from surveys in year 2010. The remaining 3,249 subjects were analyzed in this study.
2. Methods
Both general physical examinations in 2002 and 2010 took general history surveys for factors such as smoking, drinking, physical exercise, medical history, and drug usage. Physical measurements were taken by skilled nurses.
Systolic and diastolic blood pressure was measured after at least 10 minutes of rest, sitting down. Hypertension was defined with current antihypertensive use or either systolic pressure over 140 mm Hg or diastolic pressure over 90 mm Hg with prior history of hypertension diagnosis. Diabetes was defined using diagnostic criteria based on reports from American Diabetes Association in 2010;14) fasting glucose of ≥ 126 mg/dL, use of insulin or oral hypoglycemic agents and hemoglobin A1c (HbA1c) ≥ 6.5%. Liver cirrhosis and thyroid disease was defined based on surveys or by the results from upper abdomen ultrasonography and thyroid function tests (normal values: FT4, 0.78 to 1.54 ng/dL; TSH, 0.35 to 5.5 ng/dL), respectively as part of physical examination. Body mass index (BMI) was measured using weight (kg)/height (m2). Current use of antilipidemic agents or total cholesterol level over 240 mg/dL was defined as dyslipidemia in this study. Alcohol use was divided into three groups regardless of beverage type: less than once a week, once or twice a week and more than 3 days in a week. Smoking was also divided into three groups: non-smoker, old smoker and current smoker. Exercise was further divided into non-exerciser, irregular exerciser, and regular exerciser regardless of exercise type and time. Diagnosis of simple renal cyst was made when internally anechoic, sharply defined and smooth-walled and round or oval shaped cyst was noted on ultrasonography. Simple renal cyst group was further divided into unilateral or bilateral by distribution, less than or larger than 1 cm of diameter by size, and 1, 2, or more than 3 by total number of the cyst found.
3. Statistical Analysis
Statistical analysis was done using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Factors such as age, BMI, diabetes, dyslipidemia, and social history (alcohol, smoking, and exercise) that can effect development of hypertension were adjusted using logistic regression. P-value of < 0.05 was defined to be statistically significant.
RESULTS
1. General Characteristics
Among 3,249 targets, 3,032 (93.3%) were male. Average age was 54.0 ± 3.6 years and BMI was 23.5 ± 2.5 kg/m2. Average systolic and diastolic blood pressure was 120.4 ± 11.7 mm Hg and 77.8 ± 8.3 mm Hg, respectively. Alcohol use over three times in a week, regular exerciser, and current smokers were 12.7%, 42.9%, and 30.1% of the total, respectively (Table 1).
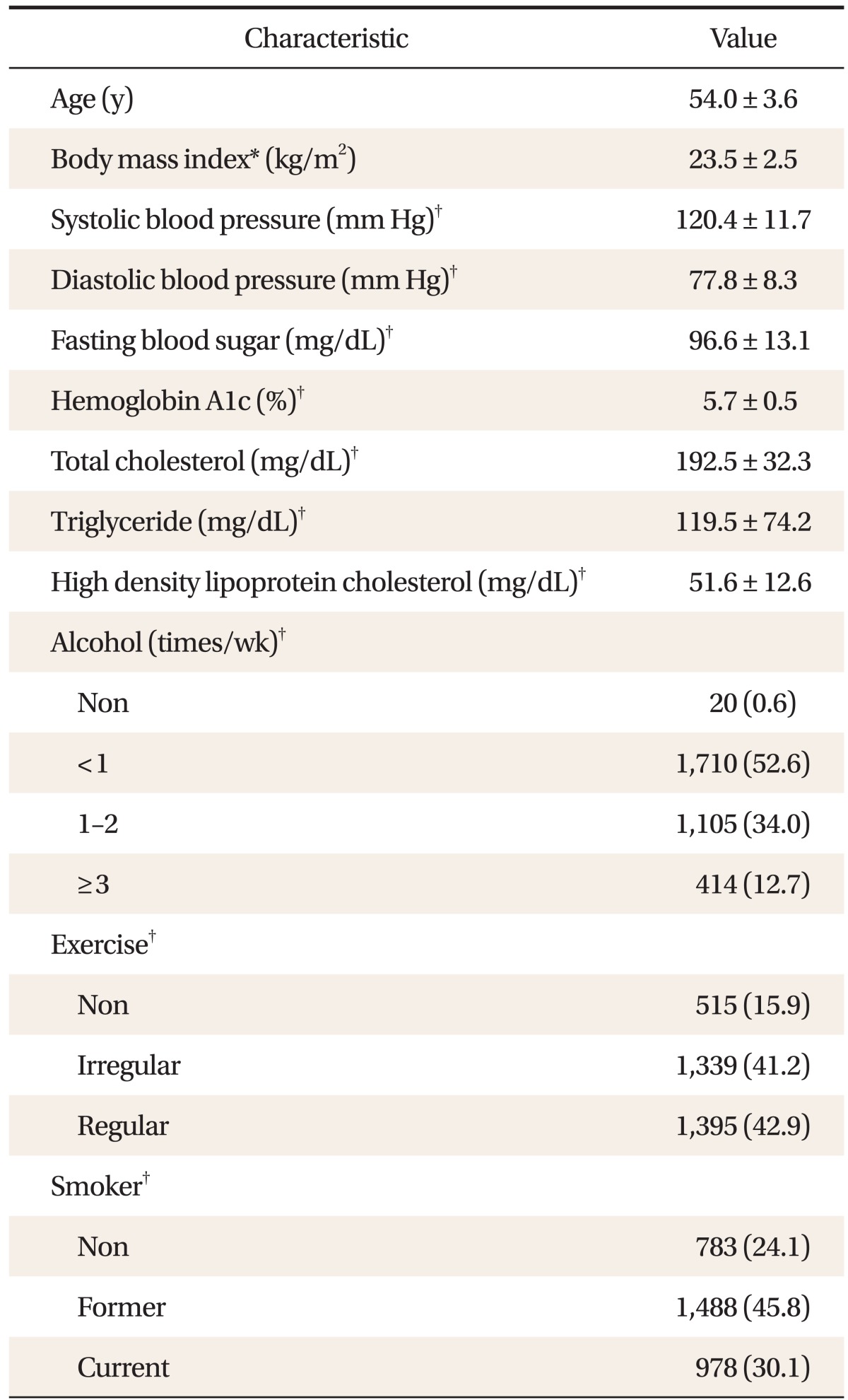
General characteristics of study subjects (n = 3,249)
2. Simple Renal Cyst and Development of Hypertension
Among 3,249 subjects (217 female and 3,032 male), 505 (15.5%) new renal cyst was diagnosed. Incidence by sex was higher in males (16.2%, 490/3,032) than females (6.9%, 15/217) (P < 0.001). Hypertension incidence was 15.5% (503/3,249) in all subjects and 20.6% in newly diagnosed simple renal cyst group.
3. Incidence of Hypertension in Newly Diagnosed and Non-Simple Renal Cyst Group
Incidence of hypertension was higher in the newly diagnosed simple renal cyst group with odds ratio of 1.53 (95% CI, 1.20 to 1.94) compared to the non-simple renal cyst group. After adjustment for age, BMI, diabetes, dyslipidemia, alcohol, and exercise, odds ratio was 1.44 (95% CI, 1.13 to 1.84), showing increased risk of hypertension (Table 2).
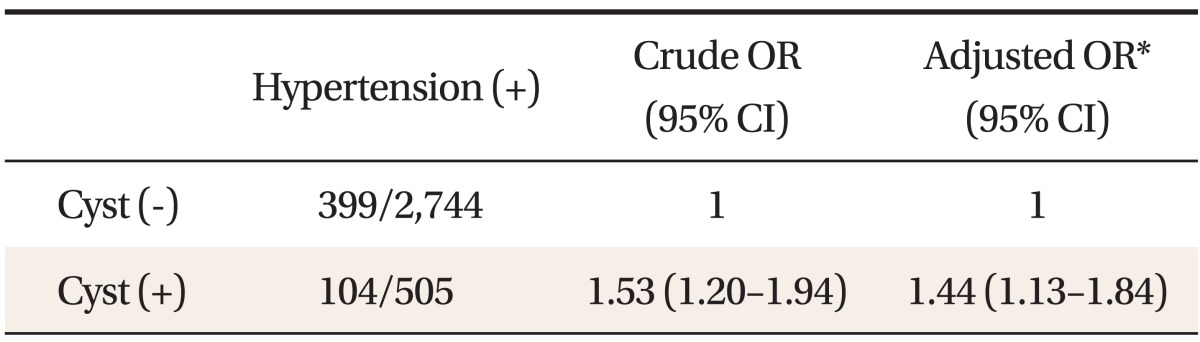
Crude and adjusted OR of hypertension according to the presence of simple renal cysts
4. Simple Renal Cyst by Distribution and Hypertension
When simple renal cyst was unilateral, odds ratio was 1.29 (95% CI, 0.99 to 1.68) and no statistical significance was found. But with bilateral cysts, statistically significant increased risk of hypertension was observed with odds ratio of 3.48 (95% CI, 2.12 to 5.71). This result was also observed even after adjustment (Table 3).
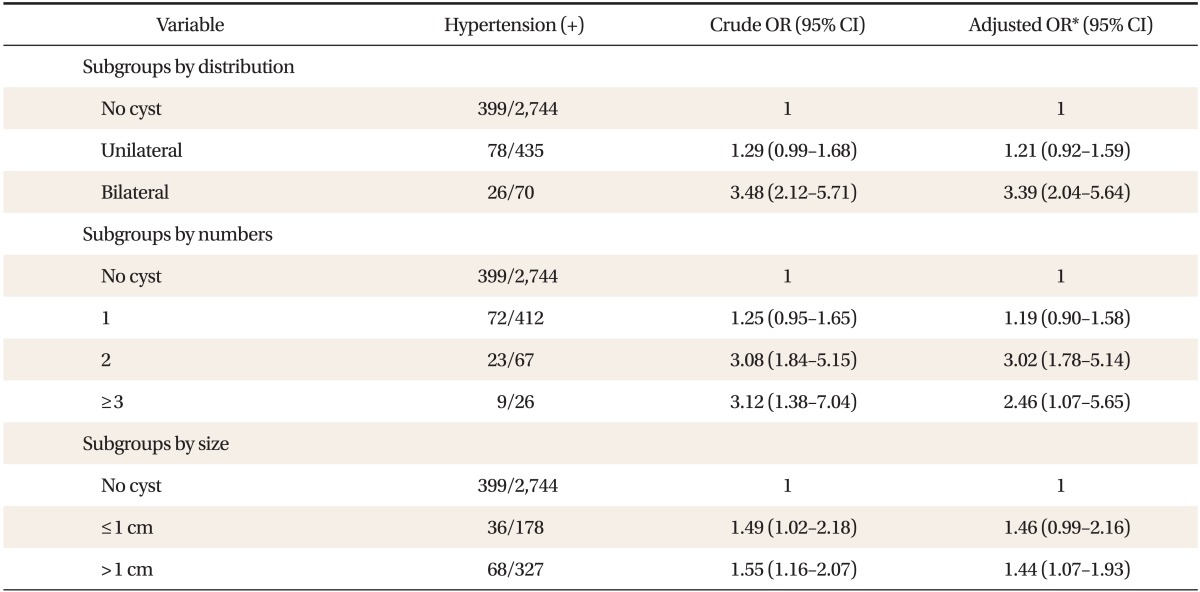
Crude and adjusted OR of hypertension in groups by distribution of cysts, numbers, and size
5. Total Number of Simple Renal Cyst and Hypertension
Total number of simple renal cyst was divided into three groups: one, two, and more than three. Each odds ratio was 1.25 (95% CI, 0.95 to 1.65), 3.08 (95% CI, 1.84 to 5.15), and 3.12 (95% CI, 1.38 to 7.04), respectively. With one simple renal cyst, no significant increased risk of hypertension was found but with two or more than three cysts, statistically significantly increased risk with positive correlation. The same was true even with after adjustment (Table 3).
6. Size of Simple Renal Cyst and Hypertension
Largest diameter of less than and more than 1 cm was analyzed. Odds ratio was 1.49 (95% CI, 1.02 to 2.18) and 1.55 (95% CI, 1.16 to 2.07), respectively, with all groups to have increased risk of hypertension. But adjusted odds ratio in the two groups were 1.46 (95% CI, 0.99 to 2.16) and 1.44 (95% CI, 1.07 to 1.93), respectively, and increased risk in only diameter of more than 1 cm group was noted (Table 3).
DISCUSSION
In this study, newly diagnosed simple renal cyst was found to be associated with increased risk of hypertension, especially when renal cyst was either bilateral, with more than 2 cysts or with largest diameter of more than 1 cm. The exact mechanism between simple renal cyst and hypertension is not known. Rho et al.15) have reported that large renal cyst may increase risk of hypertension and Luscher et al.10) have reported that activation of renin-angiotensin system by result of compression of renal artery by renal cyst may be the mechanism by which renal cyst contributes to hypertension. Pedersen et al.16) have stated underlying kidney disease or renal ischemia by result of cystic expansion may be the cause of secondary increase in renin secretion. Hence increased systolic and diastolic blood pressure in renal cyst group compared to the control. Decreased numbers of nephrons with aging is another hypothetical theory related to hypertension.17,18)
Increased risk of hypertension was noted when renal cyst was bilateral and with more than 2 cysts in this study. Based on theoretical view of compression of renal artery by the cyst, compensation by unaffected kidney against increasing blood pressure in cases of unilateral cyst can be presumed. With one simple renal cyst, it is 100% unilateral and with two cysts, 24.7% is unilateral and 75.3% is bilateral, underpinning the above theory.
The size of the renal cyst appears to have been related to the risk of hypertension in this study's results, but when the group with diameter of more than 1 cm was subdivided into more than 2 cm, 3 cm, and 5 cm, no significant increased risk was found. An important fact to take note of is that the larger the diameter of the cyst, size of the targets decreased rapidly for statistical analysis. Further studies with a larger population is needed. Incidence of renal cyst was 15.5%, similar to prevalence rate of 7.8% to 17.2% from local studies.2,7)
Prevalence rate of hypertension in this study was 15.5%, lower than previous reports from the KNHANES in 2007,19) 21.0% and 43.6% in ages 40s and 50s, respectively. Sexual differences of renal cyst may be controversial. Local studies by Chin et al.,7) Pedersen et al.,20) and Terada et al.21) have reported that prevalence rates are 2 to 4 times higher in males than in females. But Park et al.11) and Yamagishi et al.22) have reported similar prevalence rates between two sexes. In this study, prevalence rate in males was 2.3 times higher in males with 16.2% and 6.9% in females (P < 0.001). These differences in prevalence rates between males and females was previously stated by Bae et al.12) and may be related to hormonal and habitual differences between the sexes.
Although a certain relationship between simple renal cyst and hypertension was noted through this study, it is not enough to explain accurate order of relation. Terada et al.21) reported that hypertension may induce kidney dysfunction, leading to renal cyst formation. Although absent in this study's results, incidence of renal cyst by hypertension in 2010 was analyzed additionally. Odds ratio was 1.52 (95% CI, 1.20 to1.94), statistically significant increased incidence. But if this theory was unconditionally absolute, incidence of hypertension would not increase with only bilateral cysts, multiple renal cysts but not with a single cyst and only with renal cysts with larger than 1 cm of diameter as this study's result showed. Also according to some reports10,23,24) about normalization of blood pressure after renal cystectomy and percutaneous cyst decompression, simple renal cyst may be preceding condition to hypertension.
In general, characteristics of subjects, decreased fasting blood sugar (FBS) but increased HbA1c was noted and decreased total cholesterol and triglyceride but increased high density lipoprotein was also noted. This may be explained as most subjects being employees of major companies in Ulsan have diligently corrected harmful life styles in the short term prior to examination to avoid any disadvantageous measures by the examination results. Hence although short term glycemic results (FBS) improved, long term glycemic results (HbA1c) have not been affected.
Limitations to this study may include the fact that the order of relation between hypertension and renal cyst was not taken into consideration at the point of study design. Further study is needed to clarify the order of relation between two conditions. Another limitation is that groups with multiple cysts were not further identified by distribution of cyst. Authors believe that regardless of number of the cyst, bilateral renal cysts may increase risk of hypertension and if this is true, compensation mechanism by unaffected kidney against increasing blood pressure may be backed up. Identification of the relationship between the cyst size and location within the kidneys with hypertension is also needed. Another limitation to take into account is the measurement reliability because abdomen ultrasonography was not always performed again by a single doctor in 2002 and 2010. If the relationship between simple renal cyst and hypertension is clarified through suggested measures above, increased risk of hypertension could be taken into account through observation and treatment of simple renal cyst with bilateral distribution, multiple cysts or large diameter as this study has shown.
Notes
No potential conflict of interest relevant to this article was reported.