Relationship between Neck Length, Sleep, and Cardiovascular Risk Factors
Article information
Abstract
Background
Neck circumference, as a predicator of obesity, is a well-known risk factor for obstructive sleep apnea and cardiovascular diseases. However, little research exists on neck length associated with these factors. This study explored the association of neck length with sleep and cardiovascular risk factors by measuring midline neck length (MNL) and lateral neck length (LNL).
Methods
We examined 240 patients aged 30 to 75 years who visited a health check-up center between January 2012 and July 2012. Patients with depressive disorder or sleep disturbance were excluded from this study. MNL from the upper margin of the hyoid bone to the jugular notch and LNL from the mandibular angle to the mid-portion of the ipsilateral clavicle were measured twice and were adjusted by height to determine their relationship with sleep and cardiovascular disease risk factors.
Results
Habitual snorers had shorter LNL height ratios (P = 0.011), MNL height ratios in men (P = 0.062), and MNL height ratios in women (P = 0.052). Those snoring bad enough to annoy others had shorter MNL height ratios in men (P = 0.083) and women (P = 0.035). Men with objective sleep apnea had longer distances from the mandible to the hyoid bone to the mandible (P = 0.057). Men with metabolic syndrome had significantly shorter LNL height ratios (P = 0.021), and women with diabetes, hyperlipidemia, and metabolic syndrome had shorter MNL height ratios (P < 0.05).
Conclusion
This study shows that a short neck by measuring the MNL is probably associated with snoring. In addition, MNL is related to cardiovascular disease risk factors in women.
INTRODUCTION
With a high prevalence of 35% to 45% in men and 15% to 28% in women, snoring is a common health problem and a major symptom of sleep disordered breathing.1,2) Sleep apnea accompanying excessive sleepiness is also a relatively common disease with prevalence rates of 3% to 7% in men and 2% to 5% in women.3) According to a 2004 report, prevalence rates of sleep apnea among middle-aged Korean adults were 4.5% for men and 3.2% for women.4)
With the recently discovered associations between sleep disordered breathing and daytime sleepiness, decreased concentration and intellectual ability, common causes of secondary hypertension, insulin resistance, dyslipidemia, cardiovascular disease, and so on, there is an increasing interest in sleep apnea.3) In terms of physical characteristics, habitual snorers are generally known to have obese bodies, thick necks, small jaws and oral cavities, and large tongues.5) In support of this, several published reports have implied independent associations between thick necks as measured by neck circumference and snoring, sleep apnea, and cardiovascular risk factors.6,7,8) However, virtually no evidence supports the notion that short necks are related to sleep disordered breathing or cardiovascular disease. One of the few studies on this topic, which was conducted with rheumatoid arthritis patients, reported that individuals with sleep apnea had shorter cervical spines as measured by cervical spine radiography but no objective indicators concerning physical neck measurements.9) Also, another study that examined the anthropometric characteristics of obstructive sleep apnea patients in relation to rapid eye movement sleep included neck length measurements from the mastoid part of the temporal bone to the clavicle.10) Thus, in order to explore the association of neck length with sleep and cardiovascular risk factors, we used a measuring tape to measure the midline neck length (MNL) and the lateral neck length (LNL) of each subject in the consulting room.
METHODS
1. Subjects
Under the approval of the institutional review board (IRB No. 2012-045), the initial number of subjects selected included 350 adults aged 30 to 75 years who visited a general hospital between January 2012 and July 2012, were informed of the purpose and procedure of the study, and gave their prior consent for participation. Patients with a history of depression or sleep disorder or those currently on related medications were then excluded from among these subjects, leaving 240 subjects to participate in the study.
2. Methods
1) Anthropometry
Each subject's height and weight were measured using an automatic anthropometry device, and body mass index was calculated using the weight (kg)/height2 (m2) formula. For neck length measurement, the subject was seated on a chair with his or her back resting firmly against the back of the chair and facing front. As illustrated in Figure 1, the MNL was measured as the distance from the upper margin of the hyoid bone to the jugular notch. The LNL was measured in the same position as the distance from the angle of the mandible to the mid-portion of the ipsilateral clavicle. Each measurement was taken twice to every 0.1 cm using a 7-mm-wide measuring tape. Based on the reasoning that each person's neck length varies according to his or her height, the average of the two measurement values was divided by the height and then multiplied by 100 to produce the MNL height ratio and the LNL height ratio, respectively. In addition, the length of lower margin of the mandible to the upper margin of the hyoid bone (MHL) was obtained by subtracting the MNL from the LNL.
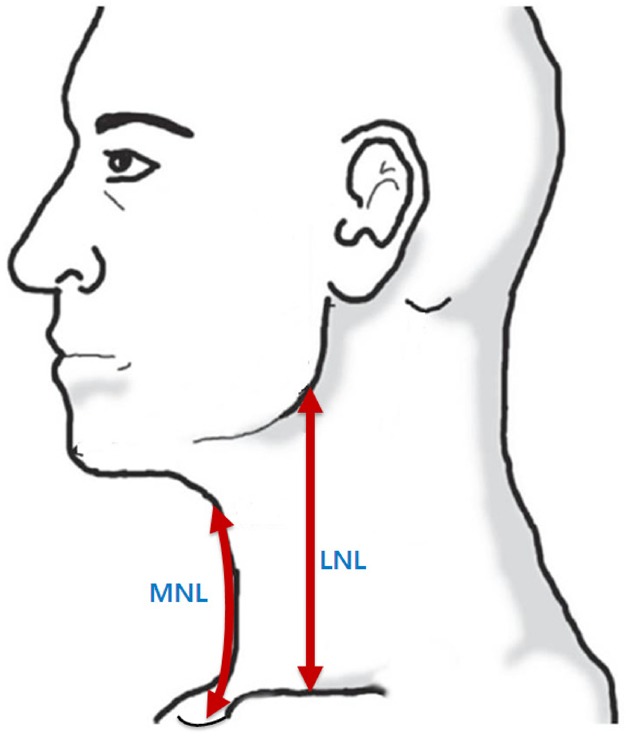
Landmark and reference line for neck length. MNL was measured from the upper margin of the hyoid bone to the jugular notch. LNL was measured from the mandibular angle to the mid-portion of the ipsilateral clavicle. MNL: midline neck length, LNL: lateral neck length.
2) Measurement of snoring, sleeping patterns, and sleep apnea
Investigators interviewed the subjects directly to complete a structured questionnaire on factors such as sleeping patterns, snoring, and sleep apnea. Questions concerning snoring included the degree of disturbance to others as well as the frequency and intensity of snoring. The questionnaire also categorized any subjects whose sleep apnea was witnessed by others sleeping with them 'at least once a week' as having sleep apnea. For sleeping patterns, the total sleeping duration, the time taken to fall asleep (sleep latency), and the degree of freshness after waking up were investigated.
3) Cardiovascular risk factors
The subjects' history of hypertension, diabetes, hyperlipidemia, stroke, smoking, alcohol consumption, physical exercise, and duration of physical exercise were investigated through self-administered questionnaires and investigator interviews. For blood pressure measurement, the subject was instructed to relax in a sitting position for at least 5 minutes and abstain from coffee and smoking for at least 30 minutes. Then, the subject's arm was placed on a desk at the same level as the heart, and the blood pressure was measured using a mercury sphygmomanometer. As stated in the JNC-7 (seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure), subjects with systolic blood pressure (SBP) ≥140 mm Hg or diastolic blood pressure (DBP) ≥90 mm Hg or those on antihypertensive drugs were categorized as having hypertension. As for diabetes, subjects with blood glucose levels ≥126 mg/dL after 8 hours of fasting or glycosylated hemoglobin level ≥6.5% or those under treatment for diabetes were categorized as having diabetes. Subjects with fasting low density lipoprotein (LDL) cholesterol levels ≥130 mg/dL or those on hyperlipidemia medication were categorized as having hyperlipidemia. Metabolic syndrome was defined as any patients who met more than three of the five criteria according to the American Heart Association/National Heart, Lung, and Blood Institute Adult Treatment Panel III 2005 criteria. We used the following diagnostic criteria for metabolic syndrome: (1) SBP ≥130 mm Hg, DBP ≥85 mm Hg, or the current use of antihypertensive drugs; (2) fasting blood sugar ≥100 mg/dL or the current use of antidiabetic drugs; (3) triglyceride level ≥150 mg/dL or the use of treatment agents; (4) high density lipoprotein (HDL) cholesterol level <40 mg/dL in men and <50 mg/dL in women or the use of treatment agents; and (5) waist circumference ≥90 cm in men and ≥85 cm in women.
3. Statistical Analysis
Chi-square tests and t-tests were used to analyze baseline characteristics of subjects according to sex, and analysis of variance tests and t-tests were used for comparative analysis of anthropometrics against snoring, sleeping disorder, sleep apnea, daytime sleepiness, etc. All statistical analyses were done using PASW SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). A P-value <0.05 was considered statistically significant.
RESULTS
1. Baseline Characteristics of Subjects
Of all 240 subjects, 178 (74.2%) were men and 62 (25.8%) were women. The average age was 49.1 ± 8.5 years for men and 47.2 ± 9.7 years for women. All measurements of the MNL, measured twice for each subject, were around 8 cm with no significant differences between men and women. Women had slightly longer LNLs than men (P < 0.05). Blood tests showed no significant differences in C-reactive protein level, LDL cholesterol level, or history of diabetes or hyperlipidemia between men and women. However, there were differences between men and women in serum HDL cholesterol, triglycerides, and drinking and smoking status. While sleeping duration was similar between men and women, those habitually snoring 4 times or more a week numbered 48 men (27.0%) and 6 women (9.7%), and those exhibiting symptoms of sleep apnea numbered 41 men (23.0%) and 2 women (3.2%), which was significantly higher in men than in women (Table 1).
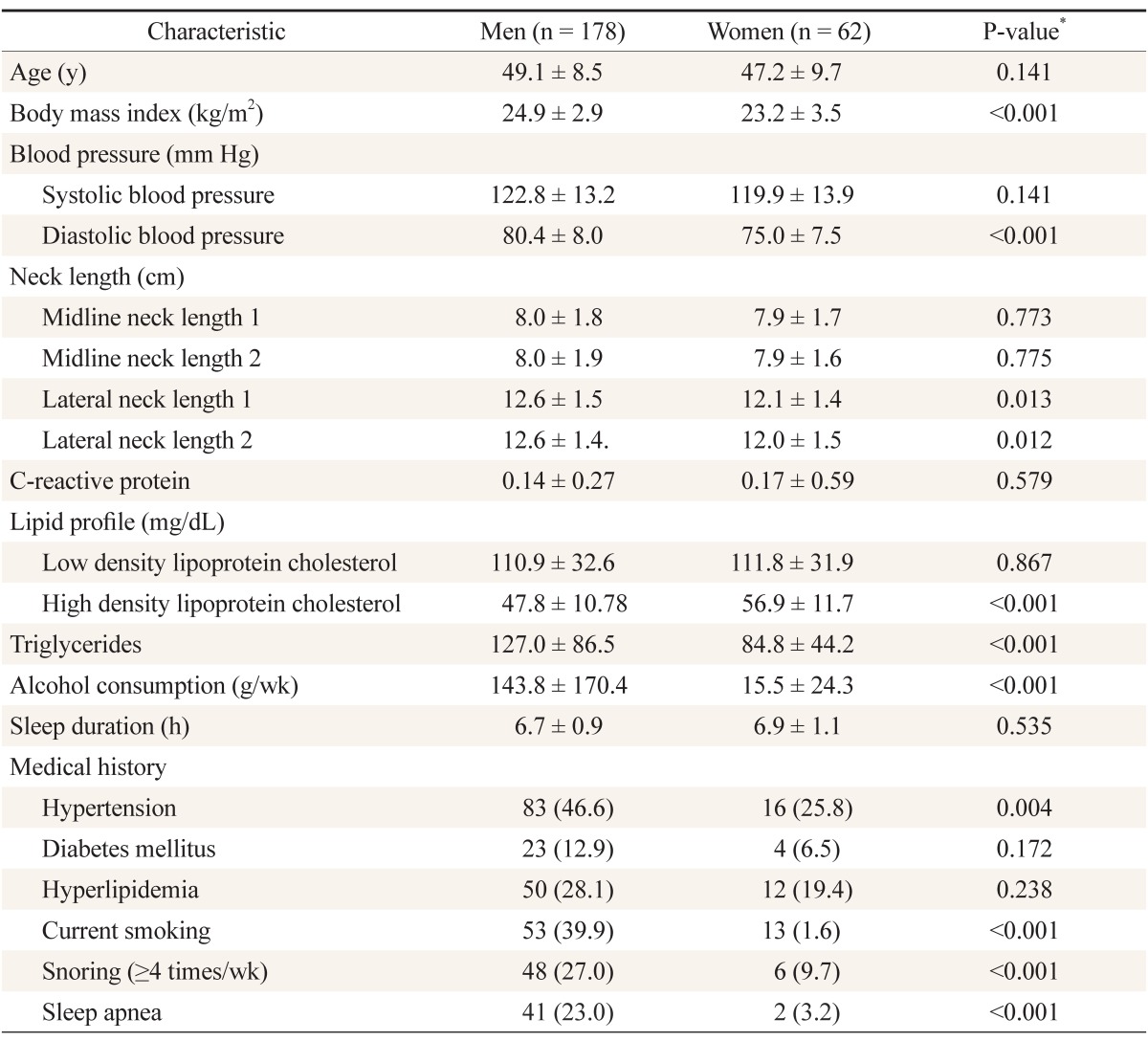
Baseline characteristics of the subjects
2. Relationship between Snoring, Sleep Apnea, and Neck Length
Men who snored 4 times or more in a week had significantly shorter LNL height ratios (P = 0.011) and shorter MNL height ratios (P = 0.062), which was not statistically significant. There were no differences in the MHL. There were also no differences between the neck length indicators for intensity of snoring or snoring bad enough to annoy others.
Women who snored 4 times or more in a week had shorter MNL height ratios (P = 0.056), but there were no differences in LNL height ratio or MHL. While there were no differences in neck anthropometrics for intensity of snoring, those snoring bad enough to annoy others had shorter MNLs (P = 0.036) (Table 2).
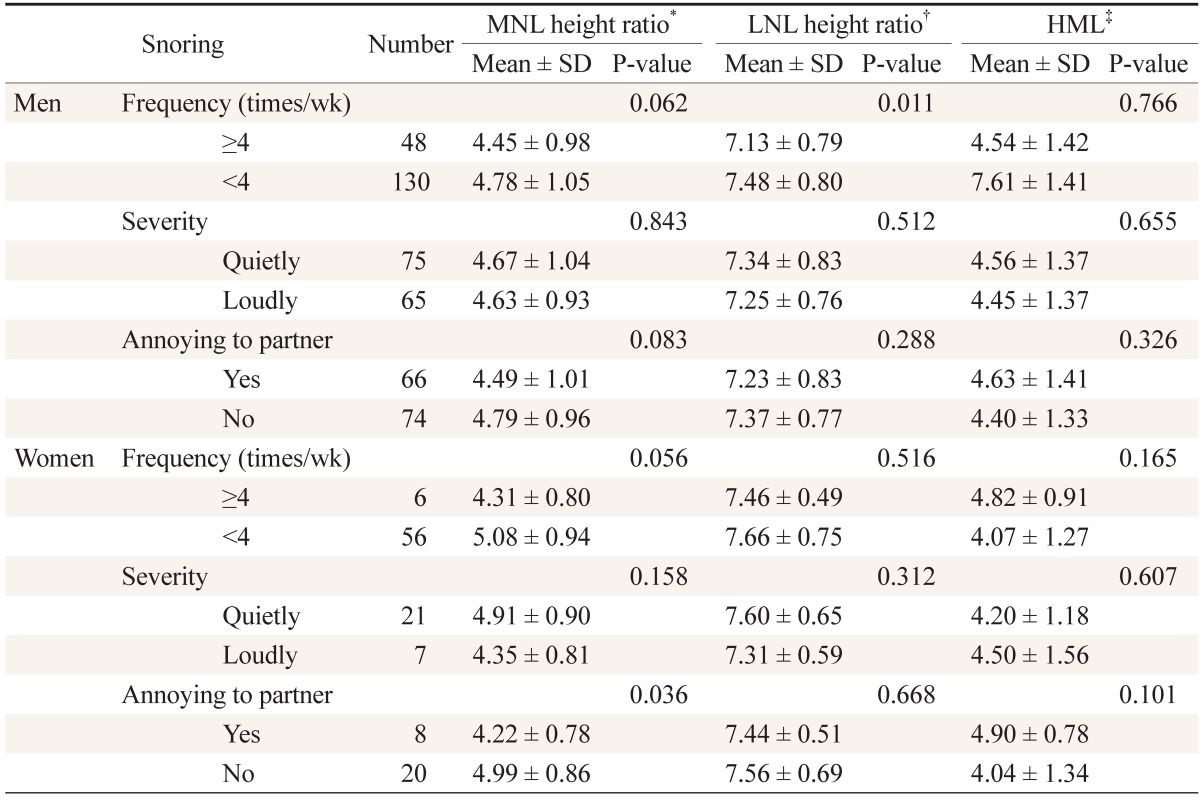
The relationship between snoring patterns and neck lengths
Men with sleep apnea had longer MHL than those without sleep apnea (P = 0.057) but without statistical significance. There were two women who had sleep apnea and their MNL height ratios were significantly shorter than that of other women without sleep apnea (P = 0.020) (Table 3).
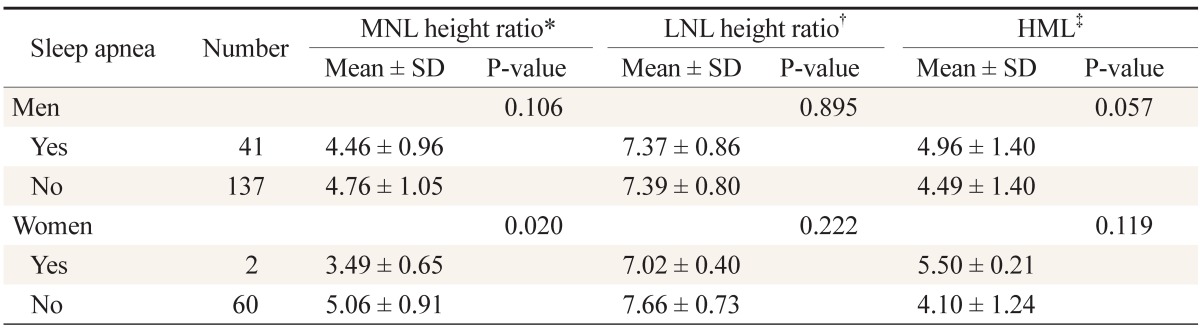
The relationship between sleep apnea and neck lengths
3. Relationship between Sleeping Patterns and Neck Length Height Ratios
For sleeping patterns, our analysis of the relationship of sleep times, sleep latency, and waking refreshed to the MNL height ratio and the LNL height ratio revealed that there were no significant differences in neck lengths between men and women. Men with sleep times <6 hours had shorter LNL height ratios than men with sleep times ≥8 hours but without statistical significance, and women with sleep times of 6 to 8 hours had significantly shorter LNL height ratios than women with sleep times ≥8 hours (Table 4).

The relationship between sleep pattern and neck lengths
4. Relationship between Cardiovascular Risk Factors and Neck Length
In the relationship between neck length height ratios and hypertension, diabetes, hyperlipidemia, and metabolic syndrome among men, while there were no differences in the MNL height ratio, the LNL height ratio was found to be shorter only in the group with metabolic syndrome than in the group without metabolic syndrome (P = 0.021). Among women, the MNL height ratio was significantly shorter in the group with diabetes (P = 0.038), the group with hyperlipidemia (P = 0.013), and the group with metabolic syndrome (P = 0.015). However, no differences were found in the LNL height ratio regarding cardiovascular risk factors (Table 5).
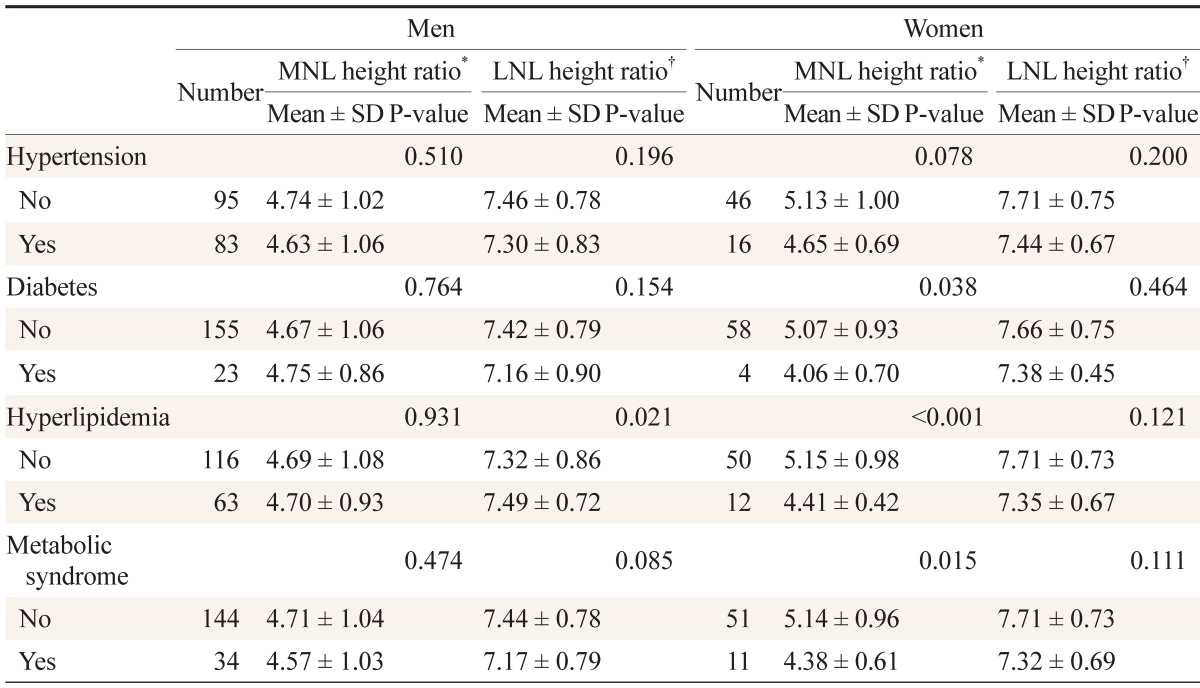
The relationship between cardiovascular risk factors and neck lengths
DISCUSSION
The purposes of this study were to explore the association of a short neck with sleep disordered breathing and cardiovascular risk factors and to evaluate the methods of measuring neck length with regard to the relationship. As a result, we learned that a short neck length has some correlation with snoring, with the MNL showing a greater correlation than the LNL in most of the categories examined. Short MNL also showed a significant correlation to cardiovascular risk factors among women but no correlation among men. Total sleep time, sleep latency, and waking up refreshed had no correlation with neck length.
Snoring is the sound produced when breathing air passes through the upper airways and vibrates the structures in the pharynx region while sleeping. Snoring used to be considered a sign of sound sleep in the past, but recent findings have indicated that snoring is a symptom of sleep-disordered breathing, which not only interferes with one's family or community life because of the noise but also is a cardiovascular risk factor. The ratio of habitual snorers who snore at least 4 times a week was 27% and 9.7% for men and women, respectively, in this study. This was slightly more than the ratio of 19.5% for men found by Oh and Cho11) and showed similar patterns with the prevalence rates of 24% for men and 10% for women in a study of individuals in Japan.12) The slight difference between this study and that of Oh and Cho.11) is thought to be the fact that the average age of subjects in this study was about 8 years older. In this study, we defined sleep apnea as the subject's apnea witnessed by his or her partner at least once a week, and the prevalence rate was found to be 23% and 3.2% for men and women, respectively. In a study of 5,020 middle-aged men and women in Korea, the prevalence rate of sleep apnea with an apnea hypopnea index score of 5 and higher was 27% and 16% for men and women, respectively.4) While this study showed a similar prevalence rate for men, the prevalence rate for women in this study was lower, perhaps because most of the subjects were lighter weight young women.
Male habitual snorers were generally found to have shorter LNLs and MNLs, while female habitual snorers were found to have shorter MNLs. Those who snored bad enough to annoy their sleep partners were generally found to have shorter MNLs, and there were no differences in neck lengths regarding the intensity of the snoring noise. In other words, snoring was found to have some correlation to neck length, with a possibly close correlation to shorter MNLs. A study of residents in Ansan, Korea, reported a positive correlation between short neck length and snoring among women but no differences among men.13) However, this particular report did not state any methods used to measure neck length. No further studies on the correlation of neck length and snoring could be found.
In this study, sleep apnea as reported by sleep partners was found to have no significant differences in all neck length height ratios among men. However, a report of a boy with Rubinstein-Taybi syndrome14) and a study of rheumatoid arthritis patients9) reported that a short neck was related to sleep apnea. While thick necks are known to be prone to fat deposition in the soft tissue of the upper airways, which obstructs the upper airways and causes snoring and sleep apnea, the mechanism of short necks causing snoring or sleep apnea is unknown. Nevertheless, the correlation analysis of obesity and neck lengths in our subjects with values adjusted for age and sex revealed highly negative correlations of obesity to the MNL (r = -0.215, P = 0.001) and the LNL (r = -0.140, P = 0.031). It is thought that obese individuals have body shapes that usually feature shorter necks.
In this study, we found that men with sleep apnea tended to have longer MHL, which is consistent with the lateral cephalometric radiograph findings of several studies.15,16) Although American and European studies have pointed out obesity as the most common cause of sleep apnea, the number of non-obese individuals complaining of sleep apnea is greater in Asia than in the West. A study that attempted to analyze skeletal characteristics and soft tissue structure of Asian patients reported the lower-positioned hyoid bone as a key characteristic of sleep apnea.17) Susarla et al.18) also reported that individuals with longer distances from the base of the maxillary sinus to the upper margin of the hyoid bone have longer soft-tissue upper airways with greater air resistance, resulting in severe sleep apnea.
In this study, we obtained the MHL by subtracting the MNL from the LNL instead of taking direct measurements. This method was chosen because it is not easy to directly measure this length with a measuring tape. Since the correlation analysis of the MHL and the MNL among the subjects of this study, with the values adjusted for age and sex, showed a highly negative correlation (r = -0.636, P < 0.001), applying the MNL, i.e., the distance from the upper margin of the hyoid bone to the jugular notch, reversely may be a viable method in the clinical context. In terms of anthropometrics, individuals with longer soft-tissue upper airways and shorter lengths from the upper margin of the midline hyoid bone to the jugular notch are thought to be more susceptible to sleep-disordered breathing.
Men generally showed little correlation between neck length and cardiovascular risk factors, but those with cardiovascular risk factors tended to have slightly shorter LNLs than MNLs. On the other hand, women with diabetes, hyperlipidemia, or metabolic syndrome had significantly shorter MNLs. It has been reported that neck circumference is an indicator of subcutaneous fat distribution in the upper body, is closely related to insulin resistance, and acts as an independent cardiovascular disease risk factor.19) However, no study concerning neck length has been done. Sleep apnea is a major cardiovascular risk factor, as it causes insulin resistance, activates the sympathetic nervous system, and activates the hypothalamic-pituitary-adrenal axis through repetitive hypoxia and sleep fragmentation. Recent studies have shown that snoring is independently correlated to metabolic syndrome,10) cardiovascular disease,20) and carotid atherosclerosis.21)
It is quite interesting that women exhibited a greater correlation of MNL not only to snoring or sleep apnea but also to cardiovascular risk factors than men. Such prominent differences are thought to be because women are less exposed to environmental factors such as smoking and alcohol consumption.
The limitations of this study include, firstly, that the study could not include a wide range of population groups, but the majority of the subjects were confined to relatively healthy middle-aged men because of the difficulties involved in measuring the neck circumference, waist circumference, MNL, LNL, etc., with a measuring tape. Secondly, although each measurement was taken twice to minimize the error that could be caused by the position or condition of the patient, it is thought that the degree of errors between individuals would not be negligible. Nonetheless, this study is a meaningful first attempt in measuring neck length. When conducting future studies on neck length, it might be interesting to measure MNL in the reclining position and in the sitting position and compare the results. Another idea would be to examine the relative condition of the neck length to the neck circumference with regard to sleep-disordered breathing and cardiovascular risk factors.
In conclusion, it was found that short necks, especially those with short MNLs, are related to snoring to some extent and short necks among women are related to cardiovascular risk factors.
Notes
No potential conflict of interest relevant to this article was reported.