INTRODUCTION
Low density lipoprotein cholesterol (LDLC) is a major risk factor in atherosclerosis and coronary heart disease (CHD) and a main target for diagnosis and treatment of hyperlipidemia.1) The National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) guidelines for hyperlipidemia, which are the most commonly referred to guidelines, were recently updated to ATP IV.2,3) These guidelines suggest that the calculated LDLC (CLDLC), assessed using the Friedewald formula, should be the primary lipid target for CHD risk reduction.4) The reference method for measuring LDLC is beta quantification.1,5) Friedewald-estimated LDLC is used in clinical practice because it is more convenient and less expensive than the more complicated and time-consuming beta quantification.6) However, the CLDLC is inaccurate when triglycerides (TG) are greater than 400 mg/dL, which occurs in dysbetalipoproteinemia and hyperlipoproteinemia secondary to diabetes, as well as when patients have not fasted.7,8,9,10)
Because of the limitations of the Friedewald calculation, homogenous methods capable of full automation have been introduced for directly quantifying LDLC.11) The direct LDLC (DLDLC) quantification produces variable results due to differences in the homogenization method and reagents. The Cholesterol Reference Method Laboratory Network (CRMLN) of the Centers for Disease Control of the United States certifies manufacturers of clinical diagnostic products and offers a list of validated reagents for accurate LDLC quantification.12) However, there are hospitals using the direct LDLC assay with components not listed by the CRMLM, which has led to questions regarding the assay's validity. Therefore, we evaluated assay performance using the domestic HiSens reagent in comparison to the LDLC calculated using the Friedewald equation.
METHODS
1. Population
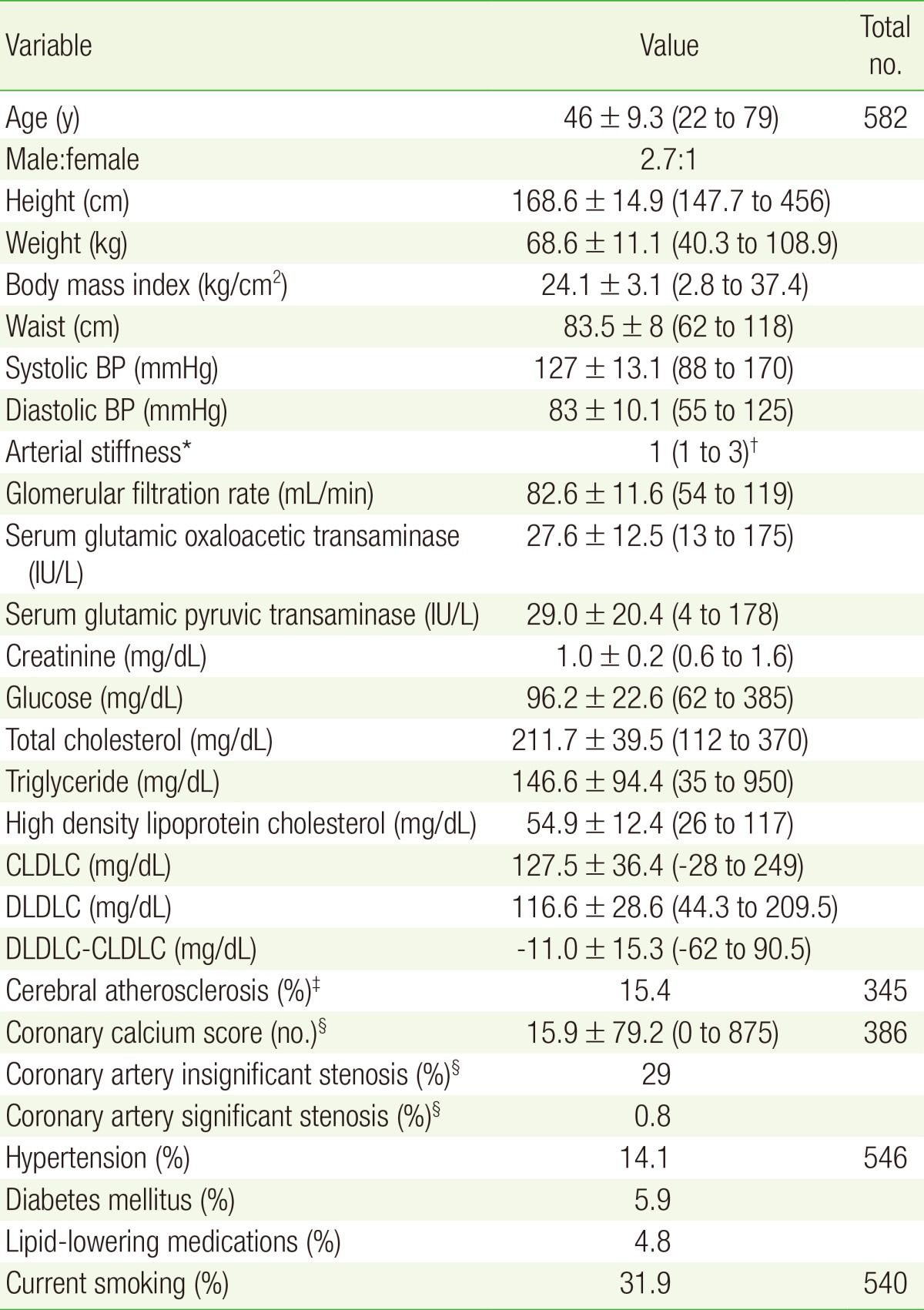
Our population consisted of 582 subjects who visited the health promotion center of the KEPCO Medical Center in Seoul, Repulic of Korea for general health check-ups between November 2012 and February 2013. Lipid profiles in the 12-hour fasting state, among other values, were analyzed (Table 1). All data were obtained by retrospective review of electronic medical records. The study protocol was reviewed and approved by the institutional review board of the KEPCO Medical Center (No. HIRB-2014-002).
2. Lipid Measurement
CLDLC was calculated using the Friedewald equation (LDLC =[total cholesterol (TC)]-[high density lipoprotein cholesterol (HDLC)]-TG/5).13) TC and TG were measured using the AU CHOLESTEROL A reagent and the AU TRIGLYCERIDE agent (Beckman Coulter Inc., Galway, Ireland). DLDLC and HDLC were measured directly using the HiSens LDLC and HiSens HDLC reagents (HBI Co. Ltd., Anyang, Korea), respectively. All lipid profiles except CLDLC were measured using the Olympus AU2700 chemistry analyzer (Beckman Coulter Inc., Fullerton, CA, USA).
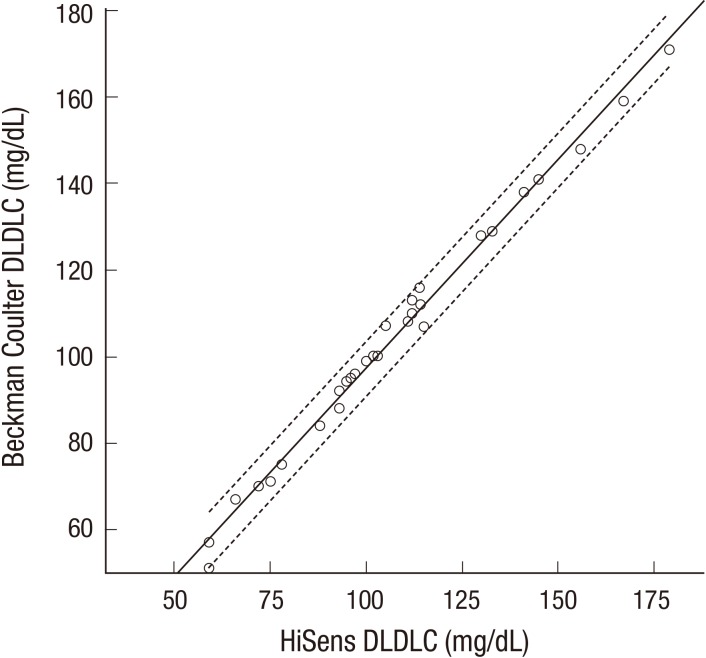
To verify the accuracy of DLDLC quantification using HiSens reagents, 30 samples with TG levels less than 400 mg/dL were randomly collected for quality control. DLDLC concentrations were compared to concentrations measured using the Beckman Coulter 5821 analyzer and dedicated reagent (BCDR) using simple regression analysis.
3. Statistical Analysis
The means┬▒standard deviations and medians for continuous variables and proportions (percentiles) for categorical variables were calculated for all descriptive statistics. The differences in LDLC concentrations were analyzed by two sample paired t-tests, linear regression analysis using Pearson's correlation coefficients, and the multiple logistic regression analysis. A P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed with the statistical software package PASW SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
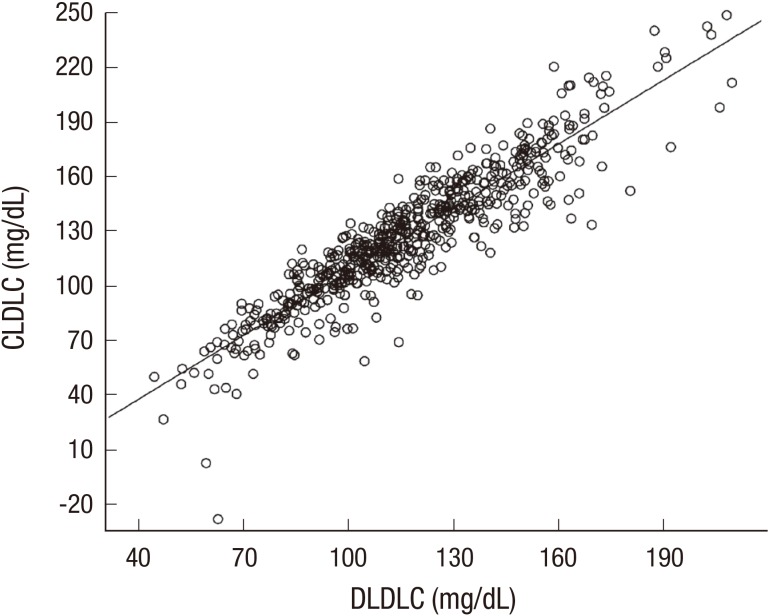
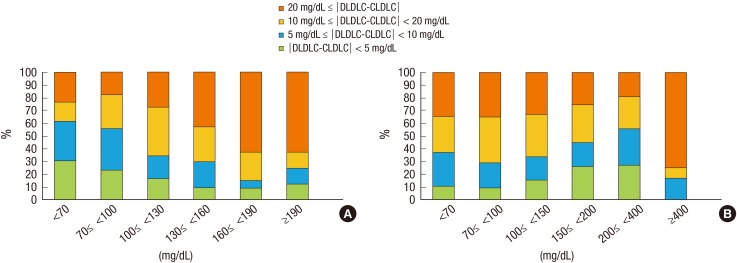
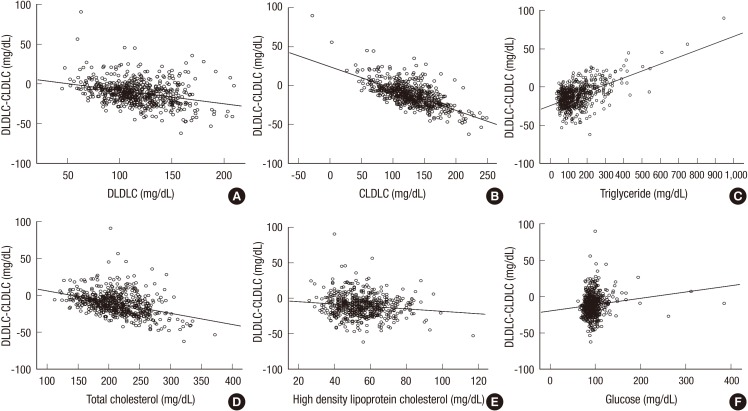
The population baseline characteristics are listed in Table 1. The mean of DLDLC and CLDLC were 116.6┬▒28.6 mg/dL (range, 44.3 to 209.5 mg/dL) and 127.5┬▒36.4 mg/dL (range, -28 to 249 mg/dL), respectively. The DLDLC and CLDLC values were strongly correlated according to simple linear regression analysis (Pearson's correlation coefficient r=0.917, P<0.001) (Figure 1). However, the mean difference between DLDLC and CLDLC was -11.0┬▒15.3 mg/dL (range, -62 to 90.5 mg/dL), and the DLDLC was significantly lower than CLDLC (P<0.001). For 61.9% of subjects, the absolute difference in LDLC measurements was more than 10 mg/dL, and for 86.9% of these subjects, the DLDLCs were lower than the CLDLCs. For 30.9% of subjects, the absolute difference in LDLC measurements was more than 20 mg/dL, and for 87.8% of these subjects, the DLDLCs were lower than the CLDLCs. The fraction of subjects with the absolute difference, more than 20 mg/dL of LDLC measurements increased dependent to DLDLC concentrations (Figure 2). Simple linear regression analysis suggested that the difference in LDLC measurements was negatively correlated with DLDLC and CLDLC (Figure 3). The categorical concordance of LDLC measurements according to the NCEP ATP III guidelines was only high in LDLC concentrations less than 70 mg/dL and 190 mg/dL or more (Table 2). The differences in LDLC measurements were positively correlated with TG concentration (r=0.557, P<0.001) (Figure 3). The fraction of subjects with the absolute difference, more than 10 mg/dL of LDLC measurements decreased dependent to TG concentrations except for 400 mg/dL or more unlike DLDLC (Figure 2).
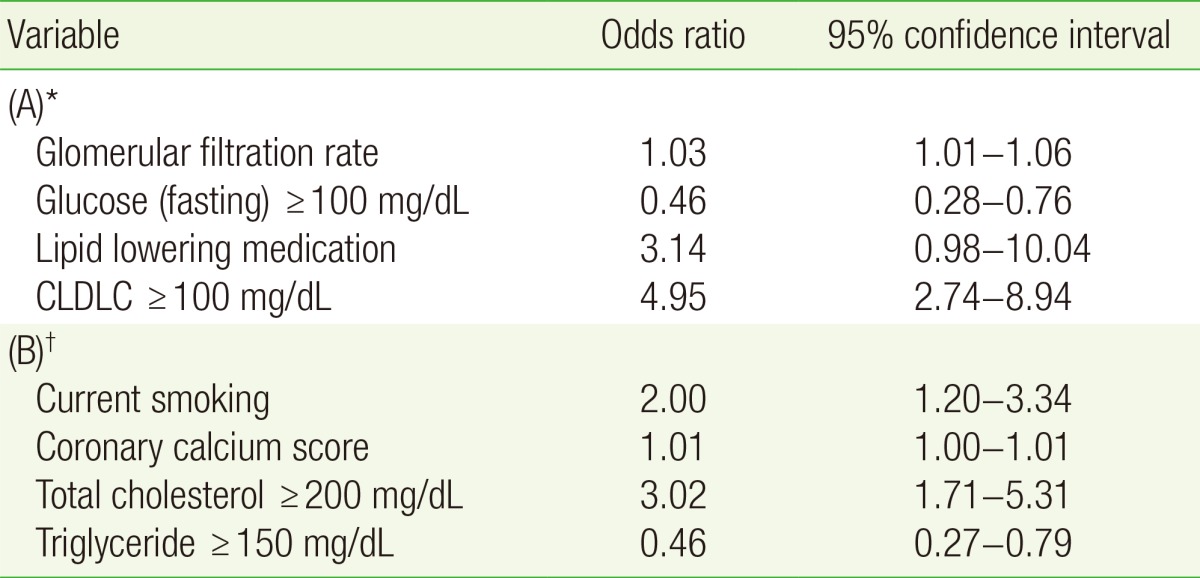
Among other factors, TC and HDLC were negatively correlated with the difference in LDLC measurements, while glucose was slightly positively correlated (simple linear regression) (Figure 3). The multiple logistic regression analysis showed that high glucose, glomerular filtration rate, and high CLDLC were significantly associated with high LDL differences (Table 3). Lipid lowering medications were also associated with high differences in LDL measurements, but the statistical significance was slightly low (P=0.054). Additionally, current smoking, coronary calcium score, high TC, and high TG were significantly associated with very high LDL differences, but the goodness of fit for the logistic regression was slightly low (P=0.047, estimated by the Hosmer-Lemeshow test). The HiSens DLDLC concentrations were strongly correlated the with Beckman Coulter DLDLC measurements (simple linear regression, rŌēź0.975) (Figure 4).
DISCUSSION
We evaluated the differences in LDLC concentrations measured by the HiSens reagent and those calculated using the Friedewald equation. According to previous studies, calculations of LDLC based on the Friedewald equation (CLDLC) correlated well with quantification of LDLC (DLDLC), but generally, CLDLC was underestimated in comparison to DLDLC.1,4,6,14,15,16,17) Our results suggest that CLDLC generally correlated with DLDLC, but CLDLC was significantly higher than DLDLC, with a mean difference of -11.0┬▒15.3 mg/dL. The DLDLC measured using the HiSens reagent was consistent with measurements made using BCDR (the mean difference was about 2.9 mg/dL, P<0.001), ensuring quality control. The highest discrepancies (62.5%) in LDLC occurred when the LDLC was higher than 160 mg/dL, but less than 190 mg/dL. These results suggest the possibility of improper management of patients with hyperlipidemia, including the general population without CHD risk, according to the ATP III or IV guidelines.
Large differences in LDLC measurements (Ōēź10 mg/dL) were observed in more than half of the participants with serum TG levels less than 200 mg/dL, which is inconsistent with other studies.14,18) Serum TG levels of more than 400 mg/dL were associated with very large differences in LDLC measurements (Ōēź20 mg/dL). Here we found that HDLC, obesity, diabetes, and gender, among the values reported by Choi et al.14) were not significantly associated with large differences in LDLC measurements. Diabetes and lipid lowering medications seemed to influence these results, but these were factors for a minority of patients.
Although the HiSens reagent for DLDLC measurements showed good correlation with other domestic reagent in a study,19) results were inconsistent with other studies, particularly in that the CLDLC was higher than DLDLC and the large differences in LDLC measurements were not generally dependent on TG concentrations, although high TG produced a positive bias. These discrepancies can be attributed to inaccuracies in either CLDLC or DLDLC estimations. It is known that the DLDLC procedure is more precise and accurate than the CLDLC, calculated using three analytical variables (TC, TG, and HDLC).11,20) However, some DLDLC measurements have been limited because of cholesterol rich very low density lipoprotein (VLDL) and intermediate density lipoprotein (IDL) for patients with diabetes or type III hyperlipidemia.21,22) The ultracentrifugation as a reference method measures LDL including IDL, and lipoprotein(a), which are all atherogenic particles. However, direct methods for measuring such particles are influenced by the VLDLC/TG ratio, the size of the LDL particle, and the wrong assignment of the calibrator value, etc. When the VLDL is rich in TG, direct methods tend to underestimate LDL-C22) and have been reported to be less reactive with lipoproteins, which contains small, dense LDL and/or lipoprotein(a).23)
High TG levels can cause low CLDLC if the TG ratio is not adjusted in the Friedewald equation.21,22,24) Both LDLC measurements can be negatively biased by high TG and the absolute difference between them can be reduced. Although the two DLDLC measurements were consistent with each other, neither of the two reagents used for our DLDLC measurements were verified by CRMLN, warranting further studies.
There were several limitations to the methodologies presented here. We did not compare the results with the reference method (beta quantification) or verified direct methods by CRMLN, for measuring LDLC. This study was cross-sectional and included healthy participants from one center. However, we found that there were differences between DLDLC and CLDLC, which could have a significant impact on clinical decisions.
In conclusion, DLDLC measurements were significantly lower than CLDLC measurements, and the differences between LDLC measurements were prone to negative and positive biases that were dependent on CLDLC and TG concentrations, respectively. In contrast to other studies, large differences in LDLC measurements were not dependent on TG concentrations. Our work suggests that verification of DLDLC accuracy is needed and differences in LDLC measurements should be accounted for in making clinical decisions.