INTRODUCTION
The incidence rates of chronic diseases in adults, such as hypertension, diabetes mellitus, and dyslipidemia, have been increasing. Consequently, issues regarding their treatment and prevention have received increased attention worldwide.1) The results of recent studies have shown that proper levels of physical activity reduce the risk of progression of these chronic diseases.2,3) Proper levels of physical activities also tends to lower cardiovascular risks and mortality rates.4)
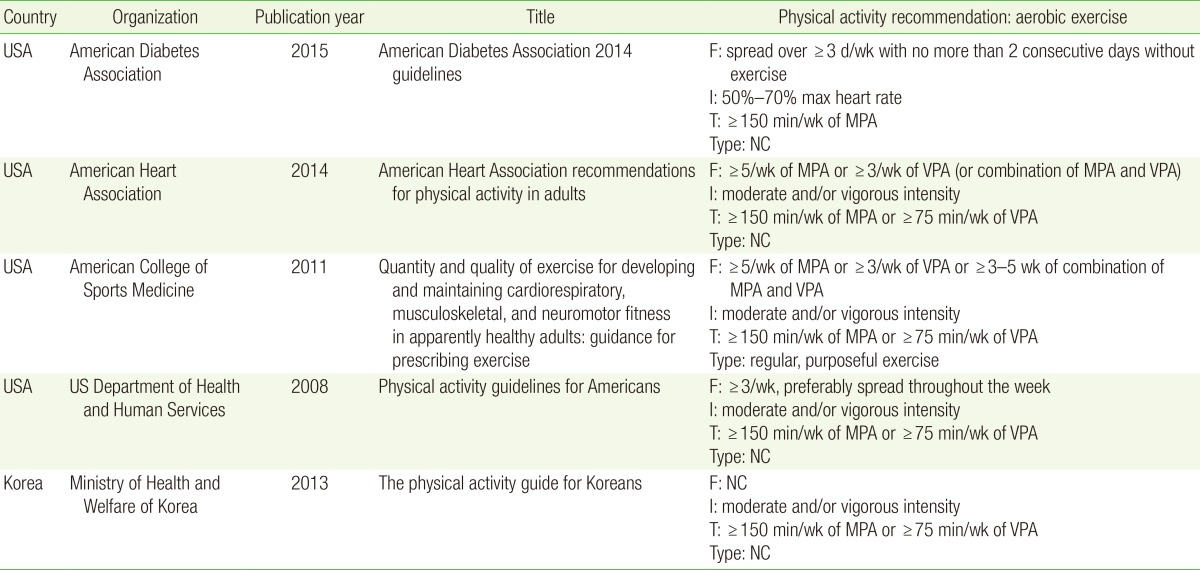
Many organizations have encouraged and provided guidelines for appropriate physical activities (Table 1).5,6,7,8,9,10) For example, the 2014 American Heart Association guidelines recommend aerobic exercise of moderate intensity for at least 150 minutes per week (more than 5 days a week) or more than 75 minutes per week in vigorous intensity (more than 3 days a week). The guidelines also recommend more than 2 days per week of moderate to high intensity resistance exercise.
However, few people follow these guidelines. Research based on the National Health and Nutrition Examination Survey (NHANES) in 2005-2006 found that the 62.0% of people self-reported exercising according to guideline recommendations, which is far beyond the 9.6% rate measured by accelerometry.11) This finding suggests that their physical activity levels were not as sufficient as the respondents had reported them to be. In South Korea, research conducted in 2001 based on the Korean NHANES (KNHANES) showed that 71.8% of adults self-reported that they did not exercise at all.12) A 2012 study by the Korean National Health Insurance Service, found that only 7.95% of participants reported moderate physical activity (MPA) for more than 30 minutes, 5 days per week; 13.37% reported vigorous physical activity (VPA) for more than 20 minutes, 3 days per week.13)
Other studies have examined physical activity levels of patients with chronic disease. Examination of the amount of physical activity using accelerometry based on 2003-2006 NHANES data revealed that patients with cardiovascular disease exercised 8.6 to 11.4 minutes per day at moderate to vigorous intensity.14) In the United States, a study targeting stroke survivors found that 17.9% of stroke patients met the weekly physical activity guidelines, compared to 25.0% of unaffected participants.15) Another study compared physical activity levels between patients with diabetes and the general population.16) The results revealed that 31% to 34% of patients with diabetes did not meet the recommended level of physical activity, a rate 13% to 19% higher than that of the general population. The level of physical activity among patients with chronic disease was low, and even lower than that among the general population.
Several previous studies have analyzed the effects of aerobic physical activity in patients with chronic disease; however, these studies targeted only patients with single diseases. To our knowledge, no other studies have targeted patients with hypertension, diabetes, or dyslipidemia, which can result in cardiovascular and cerebrovascular diseases. Consequently, it is difficult to compare physical activity levels among patients with these three diseases based on data from previous studies.
In addition, most studies were performed in the United States; few have used representative data to evaluate the physical activity of Asian patients with chronic diseases. For this reason, the aim of this study was to investigate the association of physical activity levels with hypertension, diabetes, and dyslipidemia in South Korea using representative data.
METHODS
1. Study Population
Data were collected from the fifth KNHANES, a national project that examined the sociodemographic status, health status, and health behavior including physical activities and nutritional status, of all members of households living in South Korea between 2010 and 2012. The survey was based on the Population and Housing Census Report from the National Statistical Office and selected 13,800 households from 600 districts in which household members older than 1 year of age were interviewed. A three-step stratified cluster sampling method was used to extract the samples. The rolling sampling method was adopted so that each one-year rolling sample represented a probability sampling of the whole country. The rolling samples were designed to be homogeneous and independent. Health examinations and surveys were conducted by a mobile health examination center, while the nutrition surveys were conducted by visiting each household.
Among 25,534 people who participated in the survey and health examinations, 6,140 were excluded for age (less than 20 years); 4,349 for not answer questions regarding biological, demographic, psychosocial factors, physical activities, physician-diagnosed chronic disease; and 1,172, for medical history of angina, myocardial infarction, stroke, and cancer. The final number of participants included in this study was 13,873.
2. Variables Related to Chronic Disease
Individuals were classified as having chronic disease such as hypertension, diabetes, and dyslipidemia based on diagnosis by medical professionals.
3. Variables Related to Physical Activities
Self-reported physical activity levels were estimated based on responses gathered from interviews of household members, which involved asking participants to recall their physical activity behaviors in the previous week. A KNHANES questionnaire on physical activities was developed based on the short-form International Physical Activity Questionnaire. It contained the following questions: "How many days did you perform vigorous activities for more than 10 minutes last week? How long were these workouts?"; How many days did you perform moderate activities for more than 10 minutes last week? For how long?"; "How many days did you walk for more than 10 minutes last week? For how long?"; and "How long did you remain sedentary last week?"
The weighting procedure was performed in accordance with recommendations in the appendix of the Physical Activity Guidelines for Americans (PAGA), which defines M2VPA as the moderate to vigorous physical activity performed in 2 minutes. The PAGA also defines 1 minute of VPA as 2 minutes of MPA. The M2VPA score was therefore calculated as twice the weekly VPA time added to the weekly MPA time. Based on M2VPA scores, the participants were divided into two groups: insufficient (<150 min/wk) and suffıcient (≥150 min/wk).
4. Biological, Demographic, and Psychosocial Variables
A previous meta-analysis study described physical activities and their related variables.17) Based on this research, the final biological, demographic, and psychosocial variables measured in the current study were age, body mass index (BMI), monthly household income, education (12 years or less or 13 years or more), residential area (urban or rural), marital status (married, single, separated, divorced, or bereaved), exercise competence (workable or limited movement), stress level, self-evaluation of daily activity level (active: gentle or strenuous movement in the workplace; stable: no, little, or light movement in the workplace), and self-evaluation of health level.
5. Statistical Analysis
Stata ver. 13.1 for Windows (Stata Co., College Station, TX, USA) was used to process data and perform statistical analyses. To determine the baseline characteristics according to sex, numbers (%) or mean values were calculated. Multivariate logistic regression analysis was performed while controlling for preidentified variables related to physical activities in order to clarify the correlation between chronic diseases and physical activities. Multivariate logistic analysis was also performed to identify factors highly related to physical activity levels.
RESULTS
1. Study Participant Baseline Characteristics and Physical Activity Levels
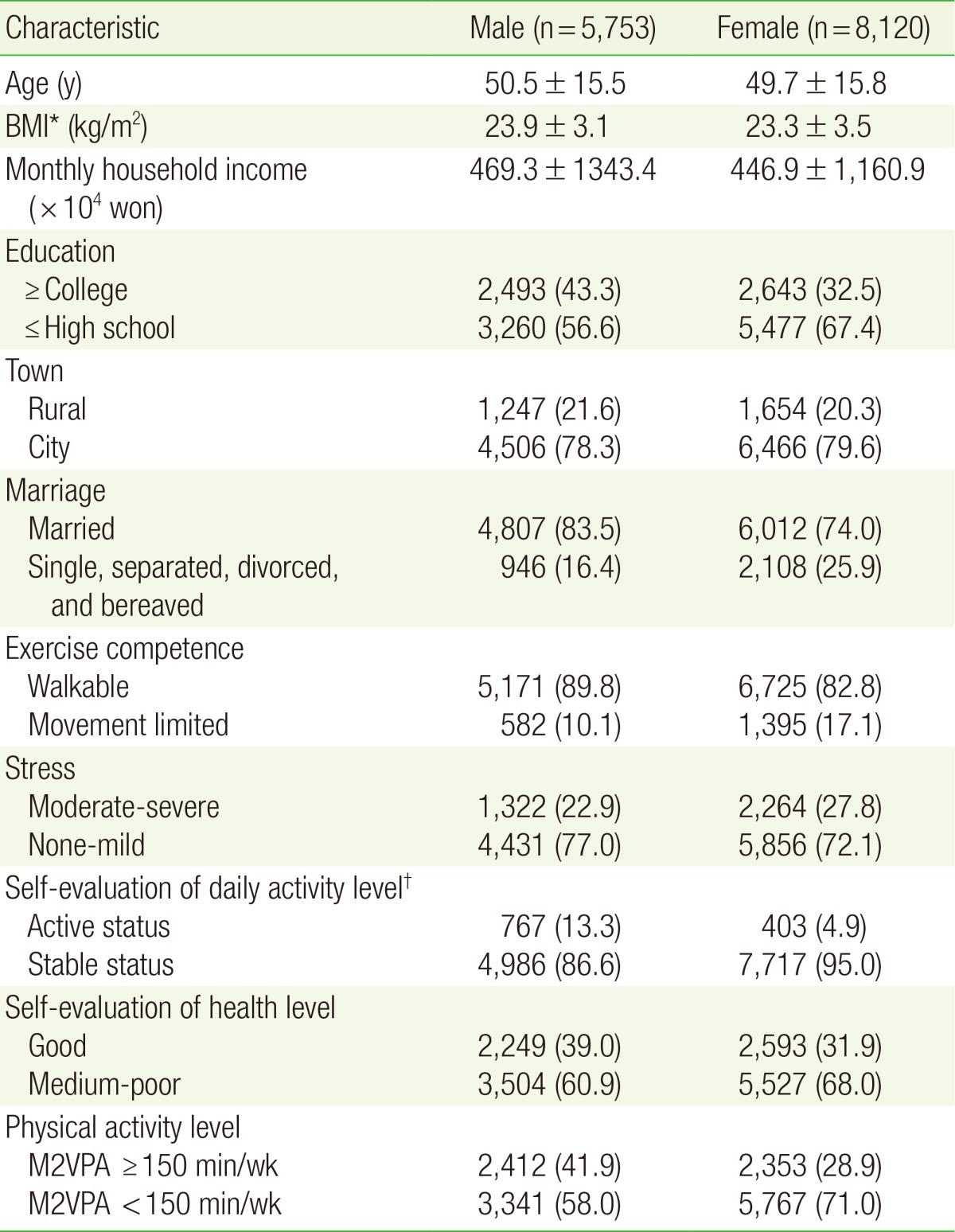
The basic characteristics of the study participants are shown in Table 2. Of 13,873 participants, 5,753 were male and 8,120 were female. Of these male and female participants, 2,412 (41.9%) and 668 (26.3%), respectively, met the physical activity level criterion (M2VPA ≥150 min/wk).
2. Association between Physical Activity and Chronic Disease
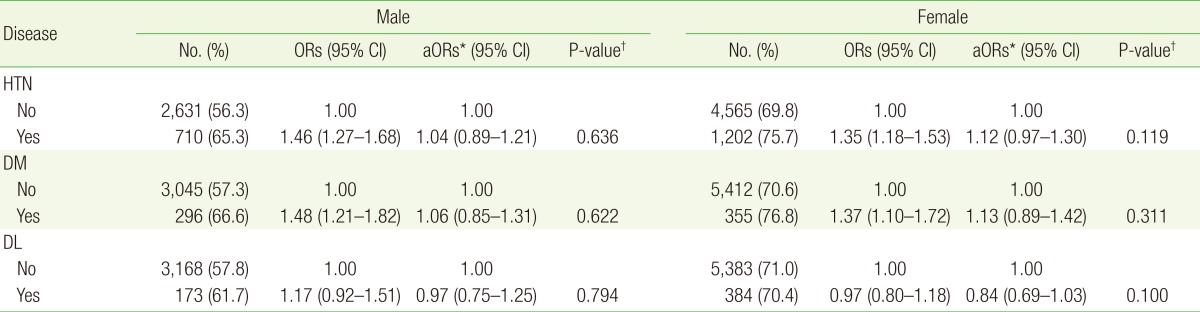
Univariate analysis of the association between physical activity and hypertension revealed that participants with hypertension tended to comply with the physical activity guidelines less faithfully than those without hypertension. Of male and female subjects without hypertension, 56.4% and 69.9% had insufficient physical activity levels, respectively. Meanwhile, of those with hypertension, 65.4% (odds ratio [OR], 1.46; 95% confidence interval [CI], 1.27-1.68) and 75.8% (OR, 1.35; 95% CI, 1.18-1.53) had insufficient physical activity levels, respectively (Table 3).
Likewise, participants with diabetes tended to comply with the physical activity guidelines less faithfully than adults without diabetes. Of male and female subjects without diabetes, 57.4% and 70.7% had insufficient physical activity levels, respectively. Meanwhile, of those with diabetes, 66.7% (OR, 1.48; 95% CI, 1.21-1.82) and 76.8% (OR, 1.37; 95% CI, 1.10-1.72) had insufficient physical activity levels, respectively (Table 3).
However, no significant difference was found between the groups with and without dyslipidemia. Of male and female subjects without dyslipidemia, 57.9% and 71.1% had insufficient physical activity levels, respectively. Meanwhile, among those with dyslipidemia, 61.8% (OR, 1.17; 95% CI, 0.92-1.51) and 70.5% (OR, 0.97; 95% CI, 0.80-1.18) had insufficient physical activity levels, respectively (Table 3).
Multivariate logistic regression revealed no significant differences in physical activity levels for both sexes between groups with and without hypertension, diabetes, and dyslipidemia (men with hypertension: adjusted odds ratio [aOR], 1.04; 95% CI, 0.89-1.21; women with hypertension: aOR, 1.12; 95% CI, 0.97-1.30; men with diabetes: aOR, 1.06; 95% CI, 0.85-1.31; women with diabetes: aOR, 1.13; 95% CI, 0.89-1.42; men with dyslipidemia: aOR, 0.97; 95% CI, 0.75-1.25; women with dyslipidemia: aOR, 0.84; 95% CI, 0.69-1.03) (Table 3).
3. Factors Associated with Low Physical Activity Levels
Multivariate logistic regression analysis was conducted using factors related to physical activity. The analysis included chronic disease status as a factor to determine if chronic diseases affected physical activity levels.
Patients with at least one chronic disease among hypertension, diabetes, and dyslipidemia were regarded as having chronic disease. The results revealed that participants who were older (aOR, 1.75; 95% CI, 1.50-1.74), were female (aOR, 1.61; 95% CI, 1.50-1.74), had lower BMI (aOR, 1.15; 95% CI, 1.06-1.24), had lower monthly household income (aOR, 1.24; 95% CI, 1.15-1.35), had lived in a city (aOR, 1.12; 95% CI, 1.02-1.23), had a stable status in the self-evaluation of daily activity level (aOR, 2.16; 95% CI, 1.90-2.45), or had medium or poor self-evaluated health levels (aOR, 1.32; 95% CI, 1.22-1.43) showed insufficient physical activity levels (Table 4).
DISCUSSION
In the present study, data from the fifth KNHANES was used to investigate the association between physical activity levels and chronic diseases in adults older than 20 years. Univariate analysis revealed that people with hypertension or diabetes had insufficient physical activity levels compared to their healthy counterparts.
Comparison of physical activity between subjects with and without hypertension and diabetes revealed that insufficient physical activity level of patients was 9% greater in male and 6% greater in female than unaffected subjects. Hence, increased physical activity should be encouraged in this population.
Furthermore, because physical activities have been widely reported to affect not only chronic disease prevention and management but also reduce the risk of cardiovascular complications and mortality, it is necessary to recommend increased physical activities to patients with chronic diseases and low physical activity levels.2,3,4)
Many studies have reported that physical activities prevent hypertension and lead to decreased blood pressure.2,18) Furthermore, Rossi et al.19) reported that physical activity could decrease the risk of cardiovascular complications and all-cause mortality rates.
In addition, physical activities prevent development of diabetes by reducing BMI and HbA1c levels.20,21) In one cohort study, Nylen et al.22) suggested that physical activities decrease the risk of mortality in patients with type 2 diabetes. Several systemic reviews also suggested that physical activities could lower the risks of cardiovascular complications and mortality in individuals with diabetes.23,24)
However, while relatively few studies have confirmed the association between dyslipidemia and physical activity, some have showed the disease preventive effect of physical activity. Dancy et al.25) reported that people with sufficient physical activity tend not to have hypertriglyceridemia and low high density lipoprotein cholesterol (HDLC) concentrations. LeBlanc and Janssen26) also reported the association between physical activity and triglyceride and HDLC levels. Therefore, physical activity is important in patients with chronic diseases.
In the present study, there were no significant differences in physical activity levels among patients with hypertension, diabetes, or dyslipidemia compared with their healthy counterparts, after correcting for variables. In other words, the reason for their low physical activity levels was not due to the chronic diseases themselves, but was rather due to other factors that can affect physical activities. Multivariate logistic regression analysis using factors known to be related to both physical activity and chronic diseases revealed that older age, female sex, lower BMI, lower monthly household income, city living, stable status in self-evaluation of daily activity levels, or medium or poor self-evaluated health level were correlated to insufficient physical activity levels. The statistical reasons for this difference after correcting for variables might include an overlap between the many variants related to chronic disease and physical activity levels; i.e., covariants. Bauman et al.17) reported that variants related to adult physical activities include age, education, sex, income and socioeconomic status, marital status, ethnic origin, health status or perceived fitness, overweight or obesity, attitudes, intention to exercise, stress, activity history during adulthood, and social support from friends and peers. Studies that investigated factors associated with reduced physical activity levels among patients with diabetes showed similar results. Furthermore, these factors may be variants that simultaneously affect the development of chronic diseases. Kim et al.27) reported that age, sex, household income, and educational level were associated with diabetes prevalence in South Korea. Nayak et al.28) found that age, sex, ethnicity, family history, BMI, and waist circumference were among the most important risk factors for diabetes. Therefore, these covariants were assumed to have no significant association between physical activity level and chronic diseases in multivariate analysis.
Unlike in patients with hypertension or diabetes, univariate and multivariate analysis revealed no significant differences in physical activity levels between patients with dyslipidemia and their healthy counterparts. This might be due to the fact that no symptoms disrupt physical activities in dyslipidemia, unlike in hypertension or diabetes. Further investigations are necessary to validate these findings.
Although chronic disease itself was not related to physical activity levels in this study, patients with chronic diseases had low physical activity levels. Therefore, patients with chronic diseases should be encouraged to engage in more physical activities, and several studies have described methods to encourage patients. Promoting behavior, decreasing physical environmental barriers, and increasing family social support for exercise may increase physical activity levels.29) In one systemic review, Sazlina et al.30) reported that individualized coaching, goal setting, peer support, physical activity monitoring, use of technology, and follow-up support increased physical activity levels.
This study has some limitations. First, a question regarding the reasons why chronic disease patients could not exercise properly was omitted from the questionnaire. If this question had been included, specialized programs for high-risk groups could have been developed. Second, the cross-sectional design of this study prevented identification of a causal relationship between chronic disease and physical activity. Because healthy people tend to sustain healthier lifestyles, they may have more sufficient physical activity levels than people with chronic diseases. Conversely, however, they may not have chronic diseases because they have sufficient physical activity levels. Lastly, a recall bias might have existed because physical activity levels were measured using self-directed questionnaires.
In conclusion, patients with chronic diseases such as hypertension and diabetes tended to have lower physical activity levels than their healthy counterparts, while patients with dyslipidemia showed no significant differences from their healthy counterparts. Given the significance of physical activities in chronic disease management, the physical activity levels of these patients needs to be improved. Although many studies have confirmed the relationship between chronic disease and physical activity, few have investigated physical activity in patients with chronic diseases. This study uses representative data from Koreans to elucidate the current physical activity levels of patients with hypertension, diabetes, and dyslipidemia, which can lead to cardiovascular diseases.