Relationship between Secondhand Smoking with Depressive Symptom and Suicidal Ideation in Korean Non-Smoker Adults: The Korean National Health and Nutrition Examination Survey 2010–2012
Article information
Abstract
Background
Research suggests that mental health is affected not only by smoking, but also by secondhand smoking. But the most researches have been conducted in North America and/or Europe. We examined whether this relationship remains evident within the South Korean population. Specifically, we investigated the effect of secondhand smoking on depressive symptoms and suicidal ideation.
Methods
We analyzed data from 6,043 non-smoking adults who participated in the 2010–2012 Korea National Health and Nutrition Examination Survey. We compared the presence of depressive symptoms and suicidal ideation in 3,006 participants who were exposed to secondhand smoking in the office or at home with 3,037 non-exposed participants.
Results
In unadjusted logistic regression analysis, secondhand smoking exposure group had more suicidal ideations than no secondhand smoking exposure (16.1% vs. 12.2%; odds ratio [OR], 1.50; 95% confidence interval [CI], 1.241–1.804), but risk of depressive symptoms was not significantly different between two groups (15.2% vs. 12.2%; OR, 1.21; 95% CI, 0.997–1.460). In multivariate logistic regression analysis, Among those exposed to secondhand smoking, the OR for depressive symptoms was 1.02 (95% CI, 0.866–1.299) and 1.43 (95% CI, 1.139–1.802) for suicidal ideation. Overall, secondhand smoking at home was significantly related to depressive symptoms and suicidal ideation. Among females, secondhand smoking exposure at home only (not in the office) was related to depressive symptoms and suicidal ideation.
Conclusion
Exposure to secondhand smoking, especially at home, may be associated with an increase in especially in female depressive symptoms and suicidal ideation among adults in South Korea.
INTRODUCTION
Smoking is a well-established risk factor for mental illness. Indeed, literature suggests that smokers are 1.5 times more likely to experience major depression than non-smokers.123) Psychiatric disorders, like major depression disorder, can involve or lead to suicidal attempts and suicidal ideation,4) and previous studies report that smoking is an influential factor for suicide-related behaviors.567) Beyond firsthand smoke, secondhand smoking is related with an increased prevalence of cardiovascular diseases and lung cancer, and recent research reveals that secondhand smoking may contribute to mortality.891011) However, it is less clear how secondhand smoking influences psychiatric disorders, even though smoking itself is a well-researched risk factor. Some studies suggest that secondhand smoking is related to depression, anxiety, and mental health issues,121314) but a significant relationship between secondhand smoking and depression or anxiety was not found in a study that examined serum cotinine levels.15)
There has been a steady decrease in the rate of smoking in South Korea for the last decade, and the South Korean government has introduced a law to regulate smokers in public areas,16) but the country's rate of smoking among adults, particularly male, is in the highest across all Organization for Economic Cooperation and Development (OECD) member countries.17) Further, South Korea's suicide rates are the highest among OECD member countries, according to the statistics of OECD health data, irrespective of gender.17) To our knowledge, research has been conducted on secondhand smoking exposure and its associated with depressive symptoms in adolescents in South Korea, but there is a lack of research investigating adults as well as the relationship between secondhand smoking and suicidal ideation.18) In the present study, we aim to identify the influence of secondhand smoking exposure on depressive symptoms and suicidal ideation by examining data from the Korea National Health and Nutrition Examination Survey (KNHANES).
METHODS
1. Study Participants
This study utilized data acquired during the first to third years (2010–2012) of the KNHANES V. The KNHANES is conducted by the South Korean Ministry of Health and Welfare, and in the fifth period they extracted sample survey group and surveyed total of 25,533 participants aged at least 1 year old from 3,800 families annually. Only data from adults who had never smoked was included, thus, data was excluded from those who were younger than 19 years of age, or when age was missing, those who had ever smoked, or had missing data for smoking experience, and those who did not complete all the questions used in this study or indicated "I don't know." Consequently, the total number of participants included in this study was 6,043. The study was approved by the institutional review board of the Samsung Medical Center (IRB file no. 2015-02-242).
2. Data Collection
Taken from the self-report questionnaires and measurements of the KNHANES, the following variables were analyzed for the purpose of this study: (1) physical measurements of weight and height drawn; (2) demographic data, including age, sex, level of education, marital status, number of family members, level of income within household, type of health insurance, and employment status; (3) health status, including history of gastric cancer, hepatic cancer, colon cancer, breast cancer, cervical cancer, lung cancer, thyroid cancer, and other types of cancer, current morbidity of osteoarthritis, rheumatic arthritis, atopic dermatitis, myocardial infarction, chronic kidney disease, diabetes mellitus, hypertension, dyslipidemia, stroke, subjective health status, and subjective body perception; (4) healthy behavior, including alcohol intake, passive and active smoking status, participation in vigorous physical exercise, participation in moderate physical exercise, participation in at least 30 minutes of walking per day, and average hours of sleep; and (5) psychiatric health, including depressive symptoms and suicidal ideation.
3. Definitions of Variables
To assess type of secondhand smoking exposure, we categorized subjects into two groups according to the place of exposure: in the workplace or at home. The non-exposed group consisted of participants who indicated they had not been exposed to secondhand smoking. The exposed group consisted of participants who reported that they were exposed to secondhand smoking for less than 1 hour or 1 hour or more. These data combined into 'yes' on the secondhand smoking status in order to analyze the exposed and non-exposed groups by workplace and home. With regard to depressive symptoms, we categorized participants into two groups: the depression group consisted of individuals who reported depressive symptoms for at least 2 continuous weeks in the last year and non-depression group consisted of those who did not report depressive symptoms. For suicidal ideation, we categorized participants into two groups according to their response to the question about having suicidal ideas during the past year. Age was categorized into 3 groups, 19 to 44, 45 to 64, and 65 years or more. Education level was categorized into 4 groups according to final graduating status: elementary school or less, middle school, high school, and college or more. Marital status was categorized into 3 groups as never married, divorced or separated, and married. Number of family members, including the participant, was categorized into 2 groups: 4 or less and more than 5. Household income was categorized into 4 groups as low, middle to low, middle to high, and high. Health insurance status was categorized into 2 groups, including those with health insurance and those without. Employment status was categorized into 2 groups: employed and unemployed. We pooled together history of gastric cancer, hepatic cancer, colon cancer, breast cancer, cervical cancer, lung cancer, thyroid cancer and other types of cancer, and then categorized cancer history into 2 groups: no history of cancer and history of at least 1 cancer. We calculated current morbidity of any of the following diseases, osteoarthritis, rheumatic arthritis, atopic dermatitis, myocardial infarction, chronic kidney disease, diabetes mellitus, hypertension, dyslipidemia, and stroke, and subsequently classified number of chronic disease into 3 groups: 0, 1, 2, or more. Subjective body perception was categorized into 5 groups, including very thin, thin, normal, fat, and very fat, and subjective health was categorized into 5 groups, including very good, good, modest, bad, and very bad. To analyze alcohol intake, we categorized subjects into 4 groups based on alcohol use disorders identification test (AUDIT) scores: 0 to 11 (normal), 12 to 24 (problem drink), 15 to 25 (alcohol use disorder), and 26 or more (alcohol dependency).19) Regular physical activity was defined as participating in at least one of the following: vigorous activity for more than 20 min/d at least 3 days a week, moderate activity for more than 30 min/d at least 5 days a week, or walking more than 30 min/d at least 5 day a week. Based on these scores, we categorized participants into 2 groups: regular physical activity and non-regular physical activity. Average hours of sleep were categorized into 2 groups of less than 6 hours and 6 hours or more.
4. Statistical Analyses
We analyzed KNHANES V original data from 2010 to 2012 according to the data analysis guidelines for KNHANES, which, given the complex sampling design, included weighting certain variables. We calculated frequencies and percentages according to participant characteristics, and conducted univariate logistic regression analysis and estimated odds ratio (OR) with 95% confidence intervals (CIs) to examine the variables that may influence depression symptoms and suicidal ideation. To examine the relationship between secondhand smoking and reported depression symptoms and suicidal ideation, we conducted a multivariate logistic regression analysis and adjusted for the variables that were significant in the univariate analyses conducted on both the total sample and by gender. Further, we conducted a sub-group analysis according to the place of the secondhand smoking exposure. P-values less than 0.05 were considered statistically significant. All statistical analyses were conducted using IBM SPSS ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Demographic Characteristics
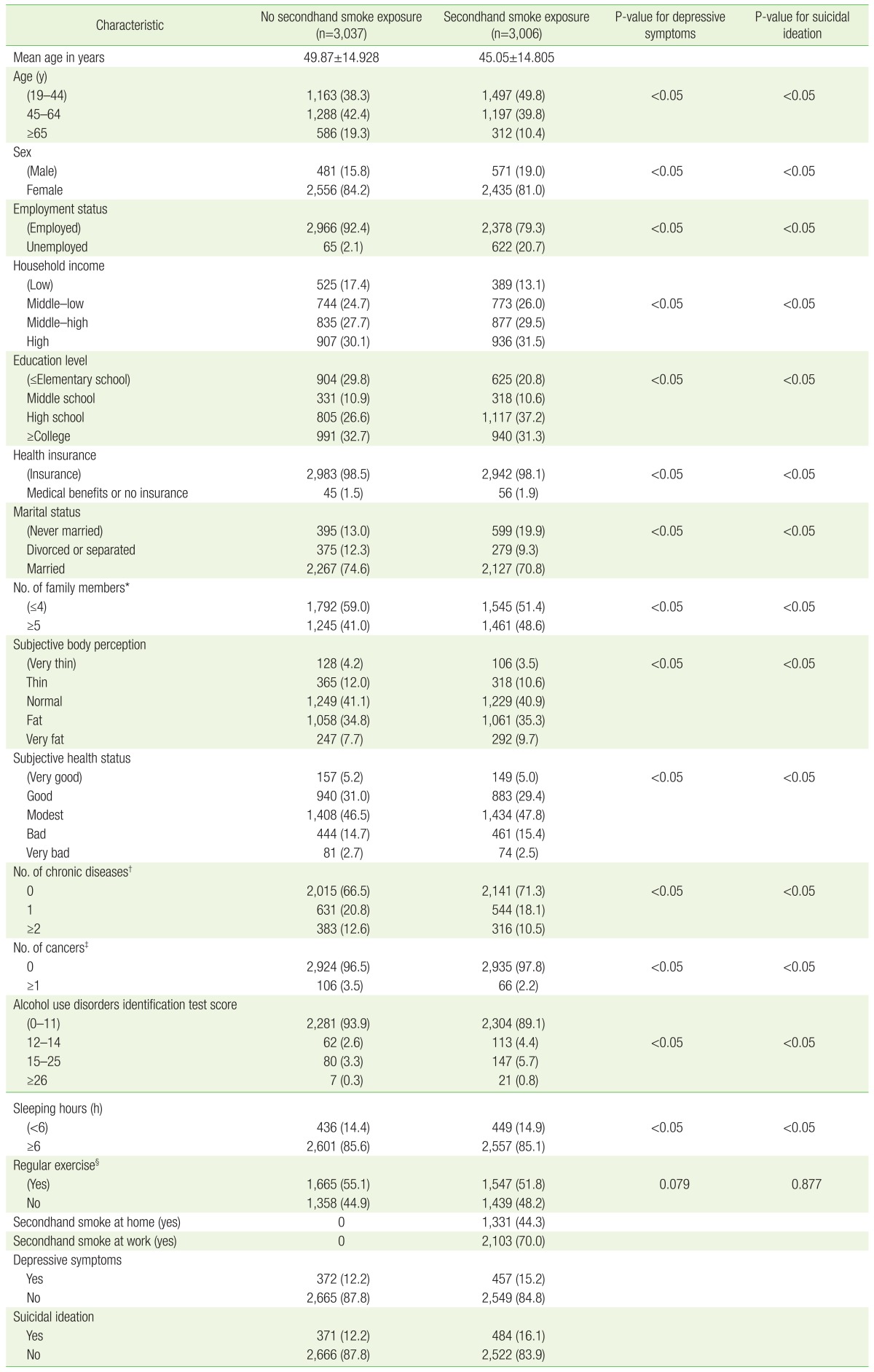
Demographic characteristics of participants are presented in Table 1. The mean age of all 6,043 participants was 47.48. The proportion of women was higher as 1,052 (17.4%) were male and 4,991 (82.6%) were female. The mean age of males was 46.19 and the mean age of females was 51.04. Half of the sample (n=3,037, 50.3%) was not exposed to secondhand smoking while the other half (n=3,006, 49.7%) was. Approximately the same percentage of males (n=571, 54.3%) and females (n=2,435, 48.8%) indicated that they had been exposed to the secondhand smoking. Of those not exposed to secondhand smoking, 372 (12.2%) reported depressive symptoms and, of those exposed, 457 (15.2%) reported depressive symptoms. Regarding suicidal ideation, 371 non-exposed participants (12.2%) and 484 exposed participants (16.2%) indicated that they had experienced such thoughts. For education level, 1796 non-exposed participants (59.1%) and 2,057 exposed participants (68.4%) recorded that they graduated high school or a higher level of education. Finally, alcohol intake data identified 149 non-exposed participants (4.9%) and 469 exposed participants (9.3%) as problem drinkers (Korean version of AUDIT score of 12 or higher).
Sociodemographic characteristics and related factors associated with depressive symptoms and suicidal ideation
2. The Relationship between Demographic Characteristics and Depressive Symptoms
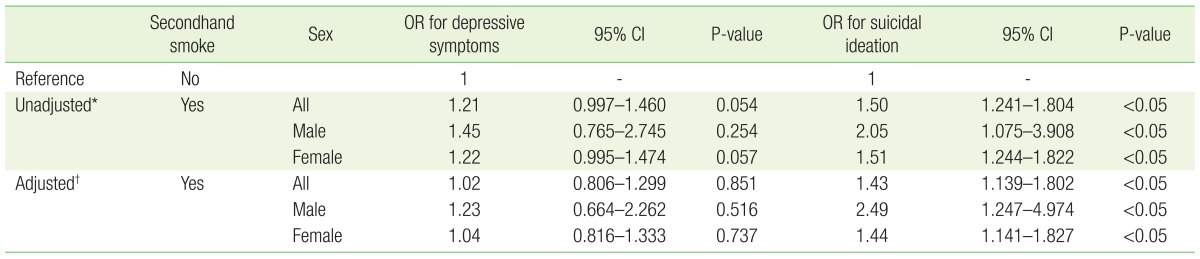
Table 1 presents the results of univariate logistic regressions for the relationships between sociodemographic characteristics and depressive symptom and suicidal ideation. In Table 2, we display the univariate logistic regression models for the relationships between secondhand smoking exposure and depressive symptoms or suicidal ideation. The unadjusted OR for depressive symptoms in the secondhand smoking group compared to the non-exposed group was 1.21 (95% CI, 0.933–1.480), but this relationship was not statistically significant (P=0.054). Other characteristics that were associated with reporting depressive symptoms include the following: 45 years of age or older, female gender, unemployed, low household income, low education level, no medical insurance, divorced or separated, 4 or less family members, very thin or very fat subjective body perception, bad or very bad subjective health status, presence of chronic disease, history of cancer, alcohol use disorder or alcohol dependency, and sleeping less than 6 h/night.
Depressive symptoms and suicidal ideation analyzed by secondhand smoke and sex
3. The Relationship between Demographic Characteristics and the Suicidal Ideation
The unadjusted OR for suicidal ideation in the secondhand smoking group compared to the non-exposed group was 1.50 (95% CI, 1.241–1.804; P<0.05). Other characteristics that demonstrated a relationship with the suicidal ideation were: 45 years of age or older, female gender, unemployed, low household income, low education level, no medical insurance, divorced or separated, 4 or less family members, very thin or very fat subjective body perception, bad or very bad subjective health status, presence of chronic disease, history of cancer, alcohol dependency, and sleeping less than 6 h/night.
4. The Relationship between Secondhand Smoking Exposure and Depressive Symptoms and Suicidal Ideation
The results of multivariate logistic regressions, after adjusting for variables that demonstrated significance in univariate analyses, are provided in Table 2. The relationship between secondhand smoking exposure and reporting depressive symptoms was not statistically significant (OR, 1.02; 95% CI, 0.806–1.299), but the relationship between secondhand smoking exposure and suicidal ideation was statistically significant (OR, 1.43; 95% CI, 1.139–1.802; P<0.05 ).
5. The Relationship between Secondhand Smoking Exposure and Depressive Symptoms and Suicidal Ideation Analyzed by Place of Exposure
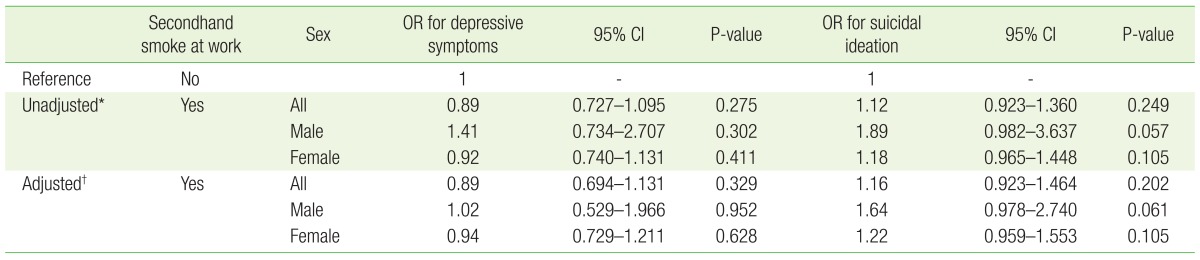
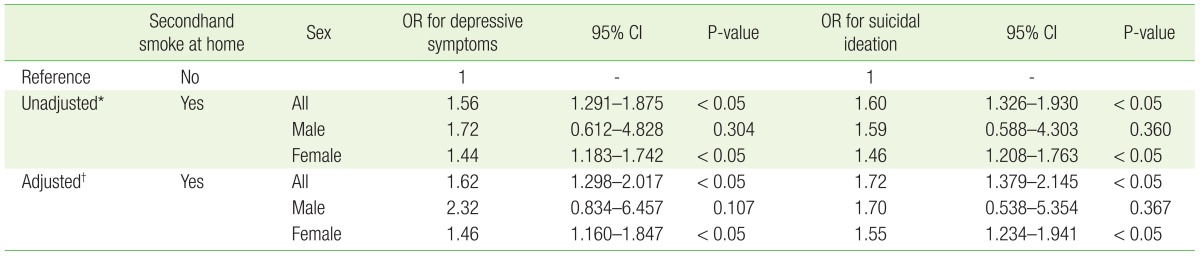
Table 3 presents the subgroup analysis for the relationship between secondhand smoking exposure and depressive symptoms and suicidal ideation among those exposed at the workplace, and Table 4 shows the subgroup analysis for those exposed at home. According to the multivariate logistic regression, the relationships between secondhand smoking exposure in the workplace and depressive symptoms and suicidal ideation were not statistically significant, but the relationships between secondhand smoking exposure at home and depressive symptoms (OR, 1.62; 95% CI, 1.298–2.017) and suicidal ideation (OR, 1.72; 95% CI, 1.379–2.145) were both significant.
Depressive symptoms and suicidal ideation analyzed by secondhand smoke at the workplace and participant sex
Depressive symptoms and suicidal ideation analyzed by secondhand smoke in the home and participant sex
6. The Relationship between Secondhand Smoking Exposure and the Depressive Symptoms and Suicidal Ideation Analyzed by Gender
Tables 2 through 4 present the relationship between secondhand smoking exposure and depressive symptoms and suicidal ideation according to gender. Based on the multivariate logistic regressions, there wasn't a gender difference between in the relationship between secondhand smoking exposure and depressive symptoms and the suicidal ideation in total exposure, or exposure in the workplace. However, among women exposed at home, we observed a significant relationship between exposure and depressive symptoms (OR, 1.46; 95% CI, 1.160–1.847) and suicidal ideation (OR, 1.55; 95% CI, 1.234–1.941).
DISCUSSION
A study conducted in the United States between 2011 and 2012 reported that 21.3% of adults aged 20 and older were exposed to secondhand smoking,20) whereas this study found 50.3% of adults in South Korea are exposed, which is more than twice as high as the US population.
We found a significant relationship between suicidal ideation and secondhand smoking exposure, but the association between depressive symptoms and secondhand smoking exposure was not significant. The nature of the relationship between secondhand smoking and the report of suicidal ideation is unclear, but there are some possible explanations. First, smoking is a risk factor for suicide, and secondhand smoking exposure may have similar physiological effects as smoking firsthand. secondhand smoking induces a decrease in dopamine and GABA (gamma aminobutyric acid) secretion,21) and a study suggests the role of reducing dopamine secretion to the suicidal attepts in non-depressed patients.22) Thus, it is possible that secondhand smoking can induce physiological effects such as reduced dopamine secretion and, consequently, result in suicidal ideation. Second, there may be a stimulation of impulsiveness and aggression due to unwanted secondhand smoking inhalation. A previous study reported increased aggressive and antisocial behaviors in participants with long-term household secondhand smoking exposure,23) and in another study, 77.8% of non-smokers indicated that they were disturbed by secondhand smoking and 69.9% of non-smokers reported that they were physically affected by secondhand smoking.24) Thus, the stress due to secondhand smoking could be a factor in the significant relationship.25) The study population that we investigated was comprised of participants who had never smoked, so dissatisfaction and stress could have manifested into suicidal ideation. Third, beyond depressive disorder, other mental disorders are related to secondhand smoking,1415) and they could be risk factors for suicide.426)
In the subgroup analyses, exposure within the home showed a relationship with increased risk of suicidal ideation as well as increased risk of depressive symptoms. This relationship was significant only among women, but the number of males exposed to secondhand smoking was 571, which was much smaller than the 2,435 women. Considering the similar trend displayed in the OR for the men's subgroup, further investigation with a larger number of participants is advised.
There are some limitations to this study. First, this is a cross sectional study based on a questionnaire that was conducted by interviewing and self-reporting, so we are unable to demonstrate the causality of the relationship. Second, we could not conduct a quantitative analysis because of the lack of information regarding the intensity and duration of secondhand smoking exposure, and we did not evaluate the biochemical approach such as using the cotinine level. Third, although we adjusted the analysis for multiple sociodemographic factors, we could not include some possible confounding variables, such as family relationships, quality of life, or life satisfaction. Fourth, we could not conduct the analysis to include whether an increase of suicidal ideation resulted in an increase in suicides committed. Fifth, this study was only conducted on non-smokers, so there is a need to include smokers in future research.
Previous research has examined the relationship between smoking and suicide, but to the best of our knowledge, secondhand smoking and suicidal behavior, specifically, have not been investigated.567) Some studies have revealed the difficulty in clarifying the direction of causality between smoking and suicide,527) but this study, which analyse the exposure to the secondhand smoking, not the firsthand smoking, could suggest a different approach about the causality of smoking and suicide.
There is some evidence to suggest a decrease in secondhand smoking exposure has resulted from enthusiastic advertisements and policies to regulate exposure.282930) Thus, in an attempt to improve suicide prevention, the public and the government should control secondhand smoking by increasing levels of awareness and attention.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.