Usefulness of the Alcohol Use Disorders Identification Test-Korean Revised Version in Screening for Diagnostic and Statistical Manual of Mental Disorders 5th Edition Alcohol Use Disorder among College Students
Article information

Abstract
Background
There is a distinction in alcohol consumption behavior between adults and college students. This study aims to verify the usability and the optimal cutoff point of Alcohol Use Disorders Identification Test–Korean revised version (AUDIT-KR) for screening alcohol use disorder in college students when the diagnostic and statistical manual of mental disorders (DSM), 5th edition diagnostic criteria is applied.
Methods
A total of 922 college students living in Daejeon were enrolled and divided into two groups based on how many items they corresponded to among DSM-5 alcohol use disorder diagnostic criteria: those who corresponded to ≥2 of the 11 items were classified into the patient group (107 males, 89 females) while the others into the control group (311 males, 415 females). The participants were evaluated using AUDIT-KR to find the optimal cutoff point for screening alcohol use disorder, sensitivity, and specificity.
Results
The mean±standard deviation scores in the AUDIT-KR were 12.76±7.27, 10.72±4.62 for males and females, respectively, in the patient group. In contrast, in the control group the scores were 6.26±5.23 and 3.95±3.59 in males and females, respectively. The area under the receiver operating characteristic curve (95% confidence interval) regarding alcohol use disorder screening by AUDIT-KR was 0.768 (0.715–0.821) and 0.883 (0.848–0.919) for males and females, respectively. The optimal cutoff point of alcohol use disorder for males was >9, sensitivity 64.49%, and specificity 76.85%. The optimal cutoff point for females was >6, sensitivity 82.02%, and specificity 80.48%.
Conclusion
This study suggested that AUDIT-KR can be used as a screening tool for alcohol use disorder in groups of college students when DSM-5 diagnosis criteria are applied.
INTRODUCTION
In Korea, students often go through a very tough and stressful process preparing for college entrance exams and tend to feel free when they enter university. Entering university has multiple implications in that students are legally allowed to drink alcohol and are susceptible to alcohol-related situations. Korean college students are likely to lapse into heavy drinking, and 25% experience alcohol use disorders [1].
It is crucial to note that problematic drinking habits in youth may heavily affect future drinking habits. Many previous studies have shown that drinking habits formed during college years continue even after graduation and are highly likely to develop into drinking problems [2,3]. In this regard, drinking problems among college students cannot be dismissed as a temporary individual problem and, furthermore, can be the starting point of social challenges.
In this sense, it is important to identify college students’ alcohol use disorders, and the World Health Organization recommends the Alcohol Use Disorder Identification Test (AUDIT) [4]. The AUDIT is an index consisting of 10 questions for measuring hazardous drinking, symptoms of alcoholic dependence, and harmful drinking [5-7]. The AUDITKorean revised version is a revised version of the AUDIT in which the concept of a standard drink is applied. The reliability and validity of the AUDIT-Korean revised version have already been proven by Kim et al. [8] The study by Lee et al. [1] on the usefulness of alcohol screening tests found that the AUDIT is more useful than the CAGE (cut down, annoyed, guilty feelings, eye opener) or the CUGE (cut down, under the influence, guilty feelings, eye opener) measure for university student groups.
The diagnostic and statistical manual of mental disorders (DSM), 5th edition was published in 2013 as a handbook for the diagnosis and statistics of mental disorders published by the American Psychiatric Association [9]. Compared with the DSM-IV, the DSM-5 incorporates alcohol dependence and abuse into one term: ‘alcohol use disorder.’ It also divides the severity of the disorder into three levels: mild, moderate, and severe. The question in the DSM-IV that asks whether there are legal problems due to alcohol drinking has been replaced in the DSM-5 with the question of whether one craves alcohol. This change suggests that the prevalence rate of alcohol use disorder in Koreans is expected to increase when considering the domestic environment, where satisfying a craving is easier because of lower alcohol prices and the relatively generous Korean practices for legal drinking compared to Western countries.
So far, there have been studies in Korea on the usefulness of the AUDIT-Korean revised version and the optimal cutoff point in screening alcohol use disorders based on the DSM-5 diagnosis for the general public but not yet for college students. This study, based on the DSM-5, aimed to confirm the usefulness of the AUDIT-Korean revised version and the appropriate optimal cutoff point for college students who have different drinking habits than the general public.
METHODS
1. Research Participants
In this study, surveys were carried out during December of 2016 with 1,034 college students living in Daejeon who were selected using an accidental sampling method. Accidental sampling refers to a type of survey that is conducted in certain areas where a considerable number of students in a university come and go frequently. The survey for this research was performed anonymously in the central libraries of two universities located in Daejeon. The students who were briefed on and disagreed with the survey were excluded from the research; 922 students who answered all the items in the questionnaire were enrolled. Written informed consents were obtained. This research was approved by the clinical ethics commission of the Chungnam National University Hospital (IRB approval no., CNUH 2016-09-006-002).
2. Data Collection
The questionnaire considered multiple sociodemographic factors such as gender, age, college degree specialization, underlying disorders, grade, participation in club activities (social activities within university) and frequency of club member gatherings, residence type (dormitory/home with family/home apart from family), whether or not the individual has methods of stress relief, financial support (allowance/part-time job), and whether or not the individual has family members (up to the 2nd degree of kinship) with drinking problems. Regarding drinking habits, the questionnaire included items such as the type of alcohol, frequency of drinking on a weekly basis, average drinking quantity at a time and maximum drinking quantity at a time. The AUDIT-Korean revised version questionnaire was used [8].
According to the guidelines of the National Institute on Alcohol Abuse and Alcoholism (NIAAA), male at-risk drinkers were defined as those that have an average of more than 4 glasses maximum at a time (binge drinking) or more than 14 glasses per week (heavy drinking). Among women, at-risk drinkers were defined as those that have an average of more than 3 glasses maximum at a time (binge drinking) or more than 7 glasses per week (heavy drinking) [10]. In addition, heavy drinking was defined as having more than 8 glasses per week for men and 4 glasses per week for women according to the recommended guidelines for Korean adults [11]. A standard glass defined by the NIAAA amounts to 14 g of pure alcohol, which is equivalent to a bottle or can of beer (about 350 mL) with 4.5% alcohol, a glass of wine (about 150 mL) with 12% alcohol, or a shot of whiskey (about 45 mL) with 40% alcohol. Calculations in this research were based on this standard and also considered a standard shot a quarter bottle of soju (about 90 mL) with 20% alcohol or a bowl of makgeolli (about 300 mL) with 6% alcohol.
The DSM-5 diagnosis questionnaire suggested by the NIAAA was used to evaluate whether or not one has alcohol use disorder [12]. The case group found to have alcohol use disorder was classified as follows based on the diagnosis classification of the DSM-5: mild for those who have two to three symptoms, moderate for those who have four to five symptoms, and severe for those who have six or more symptoms. The students who were not considered to have alcohol use disorders were classified as the control group.
3. Statistical Analysis
IBM SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analysis. Regarding demographic characteristics—in particular, smoking status, participation in club activities (social activities within university), whether or not the individual has stress relief methods, whether or not the individual has family members with drinking problems, and residence type—a chi-square test was used to compare the control and patient groups for both male and female participants. A ttest was used to determine differences in age, AUDIT-Korean revised version scores, average drinking quantity at a time, maximum drinking quantity at a time, and the amount of drinking per week between the control and patient groups.
A receiver operating characteristic (ROC) curve and the area under the ROC curve were drawn for male and female participants separately. The optimal cutoff point, sensitivity, specificity, positive predictive value, and negative predictive value of the AUDIT-Korean revised version for screening alcohol use disorder were investigated. The significance level for all statistics was set to be under 0.05.
RESULTS
1. General Characteristics of the Research Participants
Among sociodemographic characteristics, the average age (P=0.009) was younger for the female students in the patient group than those in the control group. There were more problem drinkers among family members in the patient group than in the control group (P=0.010). There were no significant differences statistically in smoking status, participation in club activity, whether or not the individual has stress relief techniques, and residence type between the patient and control groups among female students. For the male students, none of the sociodemographic characteristics showed a significant difference between the patient and control groups.
The average drinking quantity at a time (both male and female P<0.001), maximum drinking quantity at a time (both male and female P<0.001), drinking quantity per week (both male and female P<0.001), and average AUDIT-Korean revised version score (both male and female P<0.001) were significantly higher in the patient group (Table 1).
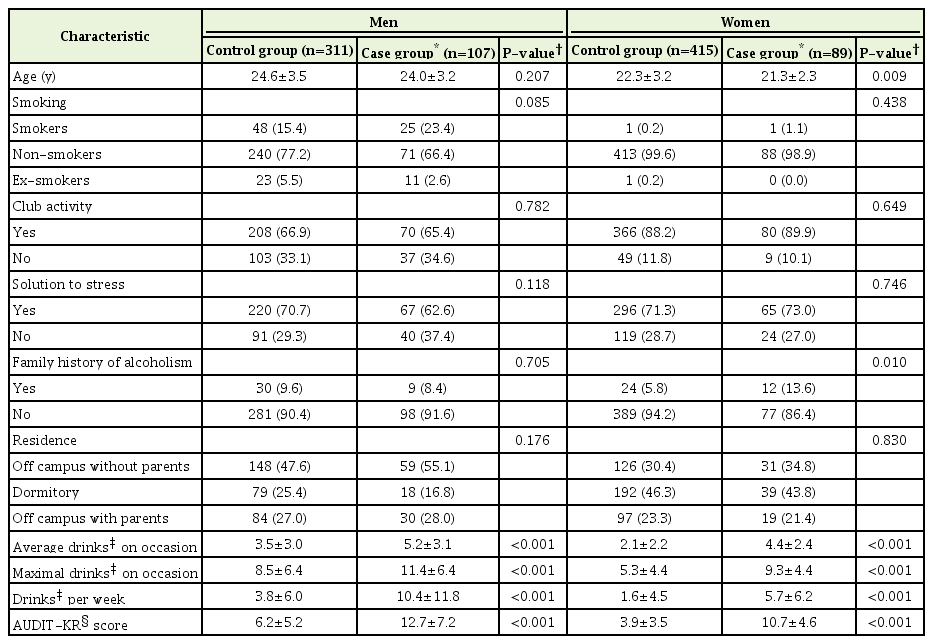
General and drinking characteristics of the participants
2. Drinking Status of the Research Participants
The proportion of the students not drinking any alcohol was 13.39% for male and 15.00% for female students. The proportion of binge drinking was 56.69% for male and 34.12% for female students. The proportion of heavy drinking was 11.24% for male and 8.13% for female students based on NIAAA guidelines and 16.26% and 14.08%, respectively, based on the Korean guidelines. The proportion of the students that had alcohol use disorder according to the DSM-5 diagnostic criteria was 25.59% for male students and 17.65% for female students. In addition, the proportion of mild, moderate, and severe level in severity of alcohol use disorder was 13.87%, 8.13%, and 3.58%, respectively, for male students and 11.50%, 5.15%, and 0.99%, respectively, for female students (Table 2).

Binge drinking, heavy drinking, and DSM-5 alcohol use disorder among the participants
The frequency of positive responses to each symptom in the DSM-5 diagnosis criteria was highest for item no. 1 (“Have you had times when you have ended up drinking more or for longer than you intended?”) and the 2nd highest for item no. 3 (“Have you spent a lot of time drinking? Or being sick or getting over other aftereffects?”), corresponding to the category of impaired control in both genders (Table 3).

Positive responses for DSM-5 symptoms questionnaire
3. The Usefulness of the Alcohol Use Disorder Identification Test-Korean Revised Version and the Optimal Cutoff Point in Screening Alcohol Use Disorder
In screening alcohol use disorder using the DSM-5 diagnosis criteria, the area under the ROC curve (95% confidence interval) of the AUDITKorean revised version was 0.768 (0.715–0.821) for the male students and 0.883 (0.848–0.919) for the female students (Figure 1). The optimal cutoff point for screening alcohol use disorder was 6 for female students and 9 for male students. The sensitivity was 64.49%, specificity was 76.85%, positive predictive value was 48.93%, negative predictive value was 88.69%, and Youden index was 0.4131 with an optimal cutoff point for screening alcohol use disorder of 9 for the male students. The sensitivity was 82.02%, specificity was 80.48%, positive predictive value was 47.40%, negative predictive value was 95.40%, and Youden index was 0.6250 with an optimal cutoff point for screening alcohol use disorder of 6 for the female students (Table 4).
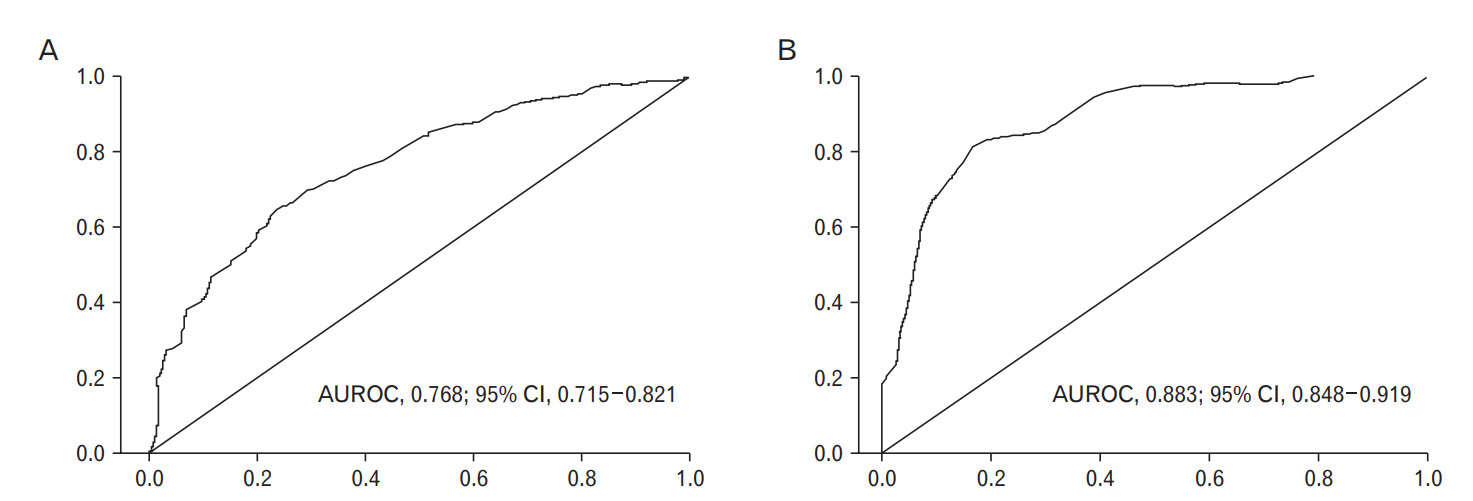
Receiver operating characteristic curves of Alcohol Use Disorders Identification Test-Korean revised version for identifying alcohol use disorders according to diagnostic and statistical manual of mental disorders, 5th edition. (A) Man. (B) Woman. AUROC, area under the receiver operating characteristic curve; CI, confidence interval.
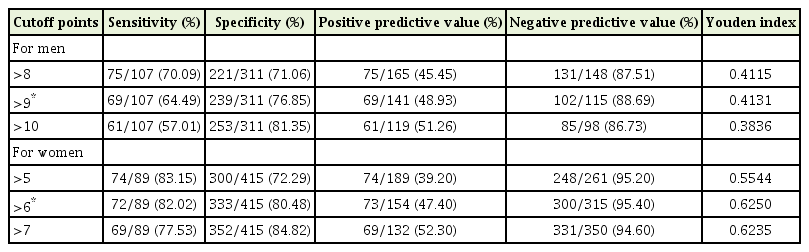
Cutoff points and performance of the Alcohol Use Disorders Identification Test-Korean revised version for identifying alcohol use disorder according to the DSM-5 in college students
DISCUSSION
In Korea, there have been studies on the usefulness of the AUDIT-Korean revised version and the optimal cutoff point in screening alcohol use disorders based on diagnosis criteria of the DSM-5 for the general public but not specifically for college students. This study intended to confirm the usefulness of the AUDIT-Korean revised version and the optimal cutoff point in screening alcohol use disorders based on the diagnosis criteria of the DSM-5 among college students, who have different drinking habits than the general public.
Closer proximity of the area under the ROC curve with 1 indicates high usefulness of the test. In this respect, this study confirmed the AUDIT-Korean revised version as a screening tool for alcohol use disorders based on the diagnosis criteria of the DSM-5 as the area under the ROC curve was 0.768 for male and 0.883 for female participants. In research of Hagman [13], the calculation of the area under the ROC curve for the AUDIT based on the diagnostic criteria of the DSM-5 among college students in the United States showed values similar to this study: 0.810 for male and 0.727 for female participants. In similar research by Kokotailo et al. [14] on American college students, the areas under the ROC curve for male and female participants were 0.872 and 0.791, respectively, which are also similar to the results in our study. However, in research conducted by Lee et al. [1], the value of the area under the ROC curve shows some different results—as high as 0.970 for male students and 0.989 for female students. In the interpretation of this difference, it should be noted that Lee et al. [1] used the diagnosis criteria of the DSM-IV whereas our study used the criteria of the DSM-5. Interpretation of these results suggests that the DSM-IV to DSM-5 test results showed that the accuracy of the test decreased from excellent to good. If similar studies are done in the future, the accuracy of the test should be checked and compared again.
This study showed that the optimal cutoff point for alcohol use disorder for male college students was 9. Research from Hagman [13] was consistent with our study, setting the threshold of the AUDIT cutoff point for male students at 9 for screening alcohol use disorders based on the DSM-5 among 251 American college students. Also, in research by Lee et al. [1], the DSM-IV TR was used to check the status of alcohol use disorders among Korean college students through diagnostic interviews, and it was confirmed that the standard cutoff point of the AUDIT for screening problem drinking among female students was 6 points, as seen in the present study. On the other hand, the 2004 research by Kokotailo et al. [14] on 302 American college students suggested that the standard cutoff point is 6 points regardless of gender. Differences in these studies may arise from certain changes in DSM diagnosis criteria and differences in ethnicity and culture.
Additionally, this research examined the positive frequency of each symptom in the DSM-5. As a result of the analysis of the frequency in the current research, items no. 1 (“Do you drink alcohol more or for longer periods than you intended?”) and no. 3 (“Do you spend a lot of time drinking alcohol and trying to overcome sickness or other side effects from drinking?”), both of which correspond to the impaired control category, showed the highest and 2nd highest frequency, respectively. The results show that the major cause of alcohol use disorders among college students is ‘impaired control,’ which may come from the cultural background in Korea that not refusing to drink is accepted as a virtue. It is anticipated that repetitive behavior of encouraging each other to drink and not refusing to do so leads to impaired control and binge drinking. There is a need for education to raise awareness of these inappropriate drinking habits as drinking behavior during college periods may determine drinking habits over a lifetime.
In our study, the proportion of binge drinking among students based on the NIAAA guidelines was 56.69% for male students and 34.12% for female students, comparatively higher than for heavy drinking. In a previous thesis studying drinking habits of college students, the proportion of binge drinkers, a drinking characteristic of Korean students, was as high as 82.2% (male 87.6%, female 33.5%) compared to the proportion of Canadian college students, which was 62.4% (male 66.9%, female 58.7%) [15,16]. Also, heavy episodic drinking was significantly higher in college students than in non-college students of the same age, so, once again, it is clear that college students have unique drinking habits [17]. However, the result of this study showed a lower proportion of binge drinking than previous studies. It is considered that college efforts to reduce drinking that induces frequent drinking accidents on university campuses lead to this result. So far, the research by Naimi et al. [18] on the US general public found that the frequency of binge drinking was 32.2% for adults aged 21 to 25, which was higher than for adults aged 35 to 54 (13.6%). The survey on drinking habits of adults in Korea also showed that the percentage of binge drinking in 20–29-year-olds was 24.3%, higher than in 30–39-year olds (21.3%) and 40–49-year-olds (16.8%) [19]. Considering that binge drinking is more common among younger adults than in any other age group, it is obvious that greater efforts are needed to reduce binge drinking in youth.
From a sociodemographic perspective, female students in the patient group were significantly more likely than the control group to have problem drinkers among family members. The research by Chun and Sohn [15] on college students also showed similar results that students who have problem drinkers in their families are more likely to have alcohol use disorders than those who do not. The study also showed that, among the US students, the chance of having an alcohol use disorder was 1.38 times higher for those who have heavy drinkers in their families than those who do not [20]. Furthermore, research by Chun and Sohn [15] revealed that the chance of having an alcohol use disorder can be influenced by participation in club activities and living conditions, contradicting the results of this research. It is considered that this reflects the recent trend in which forced drinking is less common in club gatherings.
Our study is limited in that it used a certain group of students in a certain university in a certain area, making it difficult to generalize the results to all college students. Despite its limitations, the study can be meaningful in that it determined an optimal cutoff point of the AUDIT in screening alcohol use disorders based on the DSM-5 and examined the drinking habits of college students.
Notes
No potential conflict of interest relevant to this article was reported.