Factors Affecting Adherence to Antihypertensive Medication
Article information

Abstract
Background
Hypertension is a major contributor to the global disease burden of cardiovascular and cerebrovascular disease. The aim of this study was to determine demographic and clinical factors associated with adherence to antihypertensive medication.
Methods
From August 2012 to February 2015, we recruited 1,523 Korean patients with hypertension who visited family physicians. The study was conducted in 24 facilities located in urban and metropolitan areas. Of these facilities, two were primary care clinics and 22 were level 2 or 3 hospitals. Adherence was assessed using the pill count method; a cut-off value of 80% was used as the criterion for good adherence. Sociodemographic and lifestyle factors were compared between the adherent and nonadherent groups using the chi-square test for categorical variables and t-test for continuous variables. Binary logistic regression analysis was performed with medication adherence as the outcome variable.
Results
Of the 1,523 patients, 1,245 (81.7%) showed good adherence to antihypertensive medication. In the multivariate logistic analysis, age ≥65 years, exercise, treatment in a metropolitan-located hospital, being on ≥2 classes of antihypertensive medication and concomitant medication for diabetes, and a family history of hypertension or cardiovascular diseases were associated with good adherence. Patients who had a habit of high salt intake were less adherent to medication.
Conclusion
Multiple classes of antihypertensive medications, concomitant medication, and exercise were associated with good adherence to antihypertensive medication, and high salt intake was associated with poor adherence to antihypertensive medication. These factors should be considered to improve hypertension control.
INTRODUCTION
Hypertension is a major risk factor for the development of cardiovascular and cerebrovascular diseases such as stroke [1]. An estimated 22% of the world population over 18 years of age was affected by hypertension in 2014 [1]. According to the National Health and Nutrition Survey, Korea (2015), the prevalence of hypertension in the Korean population aged 30 years and above was 27.9%, and the prevalence among men (32.7%) was higher than that among women (23.1%) [2].
Treatment of hypertension includes antihypertensive medication as well as lifestyle modifications. Patients with uncontrolled blood pressure (BP) may need more than 1 antihypertensive medication. Studies have shown that a significant proportion of hypertensive patients fail to achieve target BP levels [3,4]. In China, only 30.3% of hypertensive patients in 2010 were estimated to have BP levels within their respective target range [5]. Poor adherence to antihypertensive medication is a major cause of poor BP control [6,7]. Adherence refers to the extent to which a patient adheres to the prescribed medication at the recommended dosage [8]. In a randomized control trial, the overall rate of discontinuation of antihypertensive medication at 6 months and 1 year was 20.3% and 28.5%, respectively [3]. The rate of discontinuation at 1 year varied from 29.4% to 64.1% depending on the class of antihypertensive medication used. Thus, it is important to identify factors that may influence adherence.
Although adherence to antihypertensive medication is an active area of clinical research [9,10], treatment adherence among patients who visit primary care physicians is not well characterized. Furthermore, studies that have examined adherence across multiple antihypertensive medications and in patients on concomitant treatment for other conditions have been limited. In this prospective cohort study, we sought to determine the sociodemographic and clinical factors that affect adherence to antihypertensive medication in patients who visit family medicine physicians.
METHODS
1. Study Participants
This was a prospective multicenter cohort study conducted in 24 facilities across Korea for a period of 30 months (August 2012 to February 2015). These facilities were located in metropolitan and urban areas. Of the 24 facilities, two were primary care clinics and 22 were level 2 or 3 hospitals. A total of 1,523 Korean patients with hypertension who visited primary physicians during this period were enrolled.
Eligible patients were selected by the physicians and counseled regarding the study objectives. All patients who consented to participate were recruited. Eligible patients were those who were ≥20 years of age at diagnosis and were prescribed angiotensin II receptor blockers (ARBs) for the first time. These included both newly treated hypertensive patients and those who were already on antihypertensive medication other than ARBs. Patients were considered newly treated if they had not received ARBs prior to their enrollment. ARB was prescribed either as monotherapy or was added to other classes of antihypertensive medication as multi-therapy due to poor BP control. We subcategorized the participants based on the number of classes of antihypertensive medication. If a patient was taking one pill containing two different classes of antihypertensive medication, it was recorded as 2 classes.
We included both loss to follow-up and an adherence ratio of <0.80 as poor adherence. Of 278 participants, 218 dropped out of the study and 60 had an adherence ratio of <0.80. The most common reason for study drop out was loss to follow-up. Of the 218 participants who dropped out, 191 did not return to the clinic for follow-up prescriptions, 14 declined to take the medicine, eight had an adverse response to the medication (e.g., leg edema, headache, insomnia, dizziness, and hypotension), and five dropped out due to lack of effect.
2. Study Questionnaire
Data were collected using structured questionnaires. The questionnaires were used to obtain information on sociodemographic variables, lifestyle habits, comorbid conditions, family history of hypertension and diabetes, and number of classes of antihypertensive drugs prescribed. The numbers of prescribed and residual pills were counted and recorded at every visit.
Patient age at baseline was determined based on the date of birth registered in medical records. Body mass index (BMI) was calculated using the following formula: weight/height2. Patients were stratified into three groups based on BMI: BMI <23.0 kg/m2; 23.0–24.9 kg/m2; and >25.0 kg/m2. According to monthly income, patients were stratified into three groups: >8; 4–7.9; and <4 in million Korean won (KRW, also equivalent to 1,000 US dollars).
Participants consuming alcohol were divided into three groups: non-drinker; moderate drinker; and high-risk drinker. Moderate drinker implied the consumption of 8 glasses of alcohol or less per week for men. For women and men aged >65 years, moderate drinker implied the consumption of 4 glasses or less per week. One standard glass contains 14 g of alcohol that is equivalent to 1 bottle of beer (approximately 350–360 mL) or 500 mL of draft beer; 1/4 bottle of ‘soju’; and 1 glass (approximately 45 mL) of hard liquor [11]. ‘High-risk drinker’ referred to patients who consumed more than 8 glasses of alcohol per week for men. For both women and men aged >65 years, ‘high-risk drinker’ referred to patients who consumed more than 4 glasses of alcohol per week.
Salt usage behavior was evaluated using three validated questionnaires: “Do you usually eat salty?”; “Do you add salt or soy sauce to cooked dishes?”; and “Do you eat pan-fried or deep-fried food with soy sauce?” [12] The scoring criteria used in the first questionnaire were: very salty=12; a little salty=9; modestly salty=6; little salty=3; and not salty=0. For the second questionnaire, the scoring criteria were: always=12; frequently=8; seldom=4; and never=0. For the third questionnaire, the scoring criteria were: always=12; sometimes=6; and never=0. A total score of >18 for men and >16 for women was defined as high salt usage behavior [12,13]. Concomitant medication was assessed as per medications taken by the patient at the time of the survey.
3. Definition of Good and Poor Adherence
For measurement of adherence, we used the pill count data. Pill count is the indirect, objective measurement of adherence. The pill count method can be used to assess adherence in case of tablets, capsules, and actuated inhalers [14]. We counted the number of tablets that were taken between two clinic visits and compared it with the total number of tablets prescribed to calculate the adherence ratio. The period of time between clinical visits was different for each patient. For each clinical visit, we used the following formula for the calculation of adherence rates: [15] adherence ratio (%)={(number of prescribed pills–number of residual pills)/number of prescribed pills}×100.
The cutoff value for differentiating adherence and nonadherence was set arbitrarily [14].
In our study, the cut-off value for good adherence was set at 80%, which is commonly used in health research [10]. Adherence was calculated only for antihypertensive medications, and concomitant medication, such as for diabetes or dyslipidemia, were not taken into account. A cut-off value of 80% or above was considered good adherence. An adherence ratio of <80%, or a patient not attending the follow-up appointment, were considered indicative of poor adherence.
4. Statistical Analysis
Data were analyzed using IBM SPSS Statistics ver. 24.0 (IBM Corp., Armonk, NY, USA). Comparisons of demographic and lifestyle factors between adherent and nonadherent groups were analyzed using the chi-square test for categorical variables and t-test for continuous variables.
Binary logistic regression analysis was performed with medication adherence as the outcome variable. Logistic regression analyses were performed to identify correlates of adherence, and the associated odds ratios (OR) and 95% confidence intervals (CI) were calculated. Only significant covariates (P<0.05) identified on univariate analysis were included in the multivariate logistic regression analysis. A P-value of <0.05 was considered statistically significant.
RESULTS
1. Participant Characteristics
Table 1 presents the baseline characteristics of the study population (N=1,523). Participants were predominantly male (59.6%), married (88.1%), and had a monthly income that ranged from 4 to 7.9 million KRW (52.4%). Over half the participants (52.7%) were obese (BMI ≥25.0 kg/m2). The majority of the hypertensive participants (43.1%) were in the age-group of 50–64 years. Overall, 17.3% were current smokers and 23.3% were high-risk drinkers. A total of 699 patients (59.7%) had a habit of high salt usage. Overall, 761 patients (50.0%) were on ARB monotherapy, 550 (36.1%) were on dual therapy, and 212 (13.9%) were on multidrug therapy with ≥3 classes of antihypertensive medications. Approximately 24.9% and 51.4% of patients were also receiving medication for diabetes and dyslipidemia, respectively. A total of 104 participants had concomitant disease such as coronary artery disease (42, 2.8%), cerebral vascular disease (53, 3.5%), and vascular disease involving major arteries (19, 1.2%). The types of clinics where patients were treated were primary care clinics, secondary hospitals (537, 35.3%), and tertiary hospitals (986, 64.7%). The clinics where patients were treated were mostly located in metropolitan (1,075, 70.6%) areas; the remaining patients received treatment in urban areas (448, 29.4%).

Baseline characteristics of the study population (n=1,523)
2. Comparison of Sociodemographic, Lifestyle, and Disease-Related Factors for Good and Poor Adherence
Of the 1,523 participants, 1,245 (81.7%) showed good adherence to antihypertensive medication, while 278 (18.3%) showed poor adherence (Table 2). The duration of follow-up for each participant was different between both groups. For patients who showed good adherence to antihypertensive medication, the mean follow-up duration was 181.9±83.5 days, and for those with poor adherence, the follow-up duration was 190.9±83.5 days (P=0.287). Age, monthly income, location of clinic where patients were treated, exercise, habit of salt intake, classes of antihypertensive medication, concomitant medication for diabetes or dyslipidemia, and family history of hypertension or cardiovascular disease were significantly associated with adherence (P<0.05).
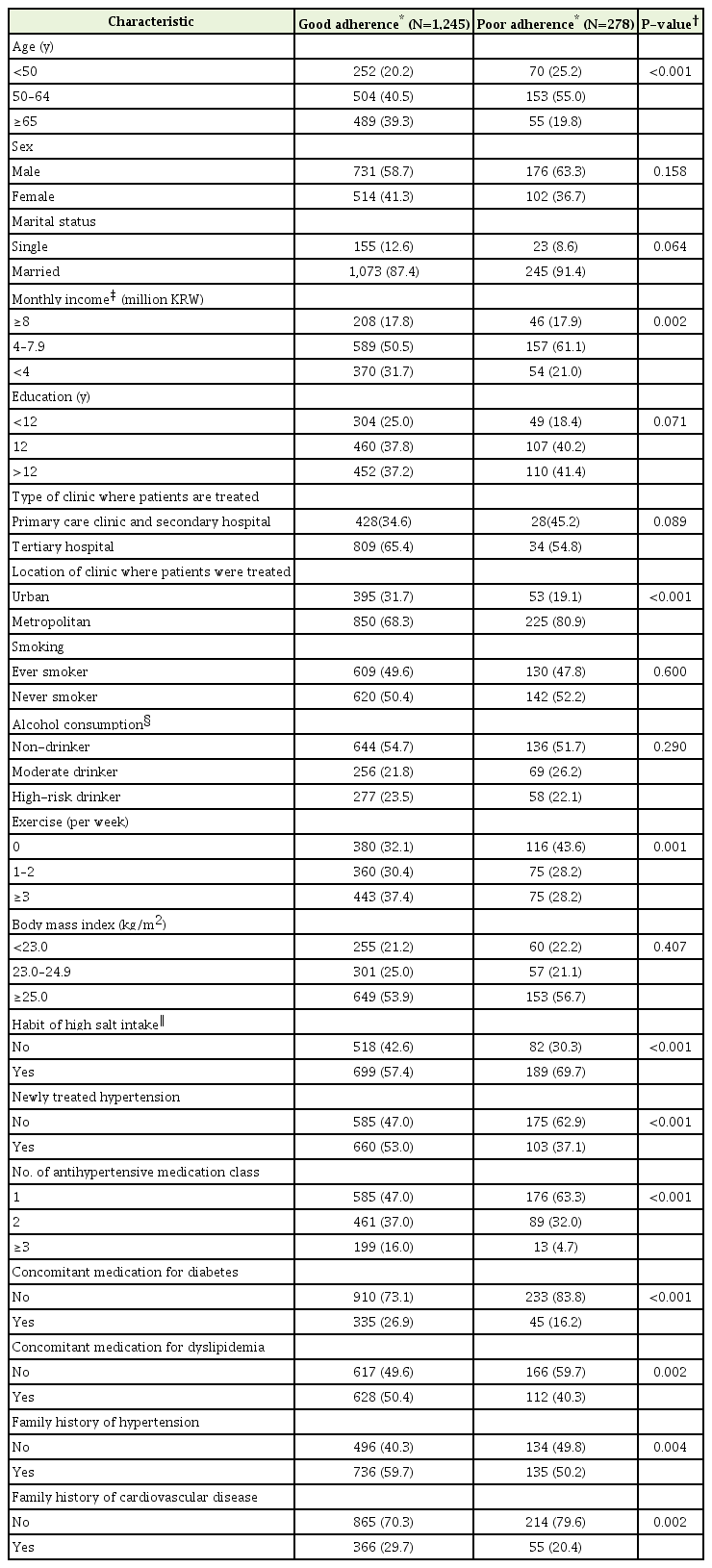
Comparison of demographic and lifestyle factors between the adherent and nonadherent groups
3. Predictors of Medication Adherence
The variables listed in Tables 3 and 4 were assessed for their association with good adherence to antihypertensive medication. Binary logistic regression was performed with adjustment for age and sex. Variables that showed a significant association with adherence were included in the multivariate logistic regression analysis as candidate variables. After adjustment for relevant baseline factors, participants who were ≥65 years of age (OR, 1.83; 95% CI, 1.18–2.83), who were treated at a metropolitan-located hospital (OR, 1.86; 95% CI, 0.78–2.36), and who exercised 1–2 times (OR, 1.43; 95% CI, 1.02–2.01) or ≥3 times (OR, 1.57; 95% CI, 1.12–2.20) per week showed good adherence (Table 3).
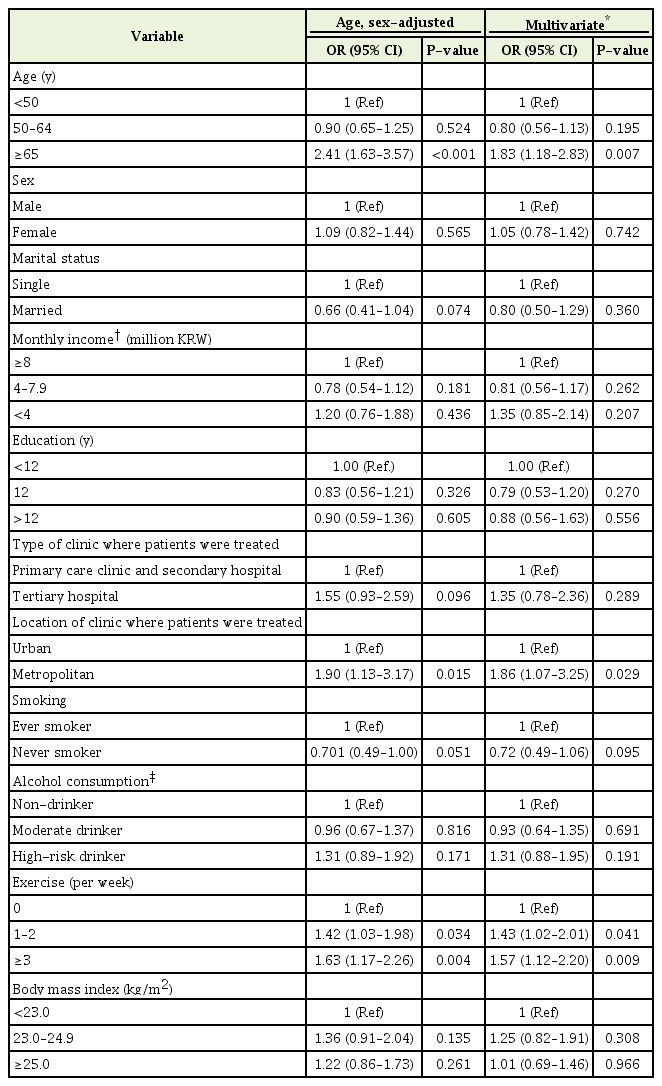
Association of sociodemographic and lifestyle factors with adherence to antihypertensive medication

Association between hypertension-related factors and adherence to antihypertensive medication
On multivariate logistic regression analysis of disease-related factors after adjustment for age, sex, monthly income, and exercise (Table 4), treatment with 2 classes (OR, 1.55; 95% CI, 1.14–2.12) and ≥3 classes of antihypertensive medication (OR, 3.82; 95% CI, 2.06–7.10), concomitant treatment for diabetes (OR, 1.67; 95% CI, 1.16–2.40) or dyslipidemia (OR, 1.48; 95% CI, 1.12–1.97), and family history of hypertension (OR, 1.72; 95% CI, 1.29–2.30), or cardiovascular disease (OR, 1.70; 95% CI, 1.21–2.39) were significantly associated with good adherence. Patients who had a habit of high salt intake were less adherent to antihypertensive medication (OR, 0.64; 95% CI, 0.48–0.67).
DISCUSSION
Of the 1,523 participants in the present study, 1,245 (81.7%) showed good adherence to antihypertensive therapy. Patients who were ≥65 years of age, who were treated at a metropolitan hospital, and those who exercised ≥1 time per week showed good adherence to antihypertensive medication. However, patients with a high salt intake were less adherent to medication. Patients with good adherence were more likely to be on ≥2 classes of antihypertensive medication and concomitant medication for diabetes and dyslipidemia and were likely to have a family history of hypertension or cardiovascular disease.
The adherence rate was higher than that reported in previous studies in China (51.7%) and the United States (67.6%) [16,17]. Because our study was conducted primarily in level 2 or 3 hospitals, which enrolled participants with relatively higher income and education status than the average Korean adults, this could account for a higher adherence rate [17]. Older age was shown to be associated with better treatment adherence among hypertensive patients due to perceived susceptibility and severity of the disease [18-20]. Although most studies are conducted based on the residence of patients, the finding in this study suggests that a regional barrier of heath care provision between urban and metropolitan areas may affect medication adherence [21]. Medical services are focused around metropolitan areas, which may enhance competition between clinics to provide better services for patients. We suggest that this positively affected medication adherence in patients who were treated in metropolitan rather than in urban clinics.
In our study, patients with high salt intake showed poor adherence to antihypertensive medication. In an observational study conducted in India [22], poor adherence to treatment was noted in persons with unrestricted dietary habits and a high salt intake of >5 mg per day. According to another study [20], among patients who were treated for both diabetes and hypertension by family physicians, those who exercised regularly or had a healthy diet with a low salt intake or both were more likely to have good adherence to medication. These results suggest that interventions aimed at lifestyle modification can reinforce good adherence to medications.
Known cardiovascular risk factors (i.e., diabetes mellitus and dyslipidemia) showed a significant association with good adherence to antihypertensive medications; this is consistent with a previous study [23]. The association of a family history of hypertension or cardiovascular disease with adherence has also been shown in other studies [23,24]. Patients with concomitant comorbid conditions, especially those related to cardiovascular risk factors, are more likely to be aware of being at a higher risk and, therefore, more likely to adhere to a therapeutic regimen [23].
A previous descriptive study showed a positive association between adherence and the number of pills [25]. This association is consistent with that observed in our study, although in our study, we analyzed the variable disaggregated by the number of classes of antihypertensive medication rather than by the number of antihypertensive drugs. It could be partially explained by the possibility that patients who are prescribed multiple pills tend to be more motivated to take medications due to the perception of the severity of the disease [25]. A second explanation may be that patients who are prescribed multiple medications daily are less likely to forget them compared to those prescribed only 1 pill [25]. Moreover, as patients may visit family physicians more frequently for medication refills, this may strengthen adherence [20].
There were several limitations in this study. First, our population may not reflect the general population of Korea as baseline demographic characteristics show that participants were relatively educated with high income. However, patients were recruited from various hospitals and different areas of Korea, making the study population heterogeneous. Second, adherence was measured indirectly using the pill count method. The direct method includes measurement of the concentration of the drug or its metabolite in body fluids (i.e., urine or blood) or measurement of biological markers [14]. However, direct methods are expensive, invasive and can also induce bias if the patient only takes medication just before the upcoming test. Also the pill count method has been shown to be more accurate compared to other subjective methods [14]. Third, the habit of salt usage was evaluated using a questionnaire rather than a precise quantification of salt intake. However, dietary surveys require fewer resources and enable the identification of dietary sources of salt that can be used for public health interventions [26,27]. There are different patterns of sodium consumption in different populations. For instance, in Western countries, most intake is from sodium content in processed food [26], but in some countries such as Korea, most of the salt is added during cooking through salt or sauce or added at the time of consumption. Dietary questionnaires may better reflect this pattern of salt usage behavior. Moreover, in a study conducted in Australia [28], a scored sodium questionnaire showed a significant correlation with 24-hour urine sodium. Fourth, we only included sociodemographic and lifestyle factors, whereas other factors such as patient, provider, family context, social or occupational conditions, and health system can have effect on adherence. Fifth, inherent in every observational study, there may have been residual confounding effects due to unmeasured or unrecorded factors.
This study has several strengths. First, the number of participants included in this study is large. Consequently, the results of our study seem notable. Second, participants of this study were recruited from various facilities by primary care physicians. Thus, the findings of the present study may be applied in family medicine clinical situation.
In conclusion, patients who showed good adherence to antihypertensive medication were on ≥2 classes of antihypertensive medication and other concomitant medications such as those for diabetes and dyslipidemia. High salt intake was associated with lower adherence. Among these factors, salt intake and exercise are modifiable factors. As such, we may employ these findings to identify patients who are less likely to adhere to medication for those who visit family medicine physicians to enhance adherence to medication.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was supported in part by the Daiichi Sankyo Company in Korea.