Pelvic Floor Muscle Exercise Education and Factors Associated with Implementation among Antenatal Women in Hospital Universiti Sains Malaysia
Article information

Abstract
Background
Pelvic floor muscle exercise is effective for pelvic floor muscle dysfunction. Despite the high prevalence of pelvic floor muscle dysfunction in women in the community, pelvic floor muscle exercise recognition is low in Malaysian society; thus, this intervention is not frequently used . This study assessed the knowledge of, attitudes towards, and use of pelvic floor muscle exercise among antenatal women before and after educational classes. The study also determined factors associated with exercise practice.
Methods
An interventional study was conducted in 121 antenatal women selected through systematic random sampling between June and December 2010. Baseline knowledge of, attitude towards, and practice of pelvic floor muscle exercise were assessed using self-administered validated questionnaires at first visit and at 2 months post-partum. All participants attended two exercise education classes on their next two visits before delivery. A paired t-test and multivariate analysis were used for data evaluation.
Results
The mean pre-intervention scores for knowledge, attitudes, and practice were 24.98, 24.25, and 3.51, respectively, with statistically significant mean score increments after intervention (P<0.001). The mean differences were 4.67 (95% confidence interval [CI], 3.86–5.49), 3.77 (95% CI, 3.05–4.50) and 3.45 (95% CI, 2.90–4.00) for knowledge, attitudes, and practice, respectively. Lack of baseline information on pelvic floor muscle exercise was significantly associated with practice change following an educational class.
Conclusion
Education is effective in improving knowledge of, attitude towards, and practice of pelvic floor muscle exercise. There is a need for greater effort to increase exercise awareness in our community, especially during antenatal class.
INTRODUCTION
Pelvic floor muscle exercise (PFME) is considered first-line conservative treatment and has been proven effective for women with pelvic floor muscle dysfunction (PFMD) and urinary incontinence (UI) [1,2] or pelvic organ prolapse [3,4]. It is recommended in treating UI in the general population [5] and may prevent women from having UI during pregnancy as well as after delivery [6]. Women who practice PFME are 7 times more likely to cure or improve PFMD than those without treatment [6].
There is a high prevalence of UI in all nations around the world. The prevalence rates range from 23% to 44% in a study done in four European countries [7,8]. The prevalence was reportedly higher in pregnancy. Al-Mehaisen et al. [9] reported a rate of 45% in late pregnancy and Francis [10] reported a prevalence of 6%–31% following childbirth. In Malaysia, the prevalence was 40.4% among women in an outpatient clinic [11] and 22.1% among women at 5 months postpartum [12]. One study reported that 76.6% of women attending menopause clinic had some degree of uterine prolapse [13]. Despite the high prevalence of PFMD, few women practice PFME. Only 17% of antenatal mothers performed PFME at least once a week during pregnancy [14] and only 54% use of PFME in another study [15].
Many women have misconceptions regarding PFME. Many elderly women believe that UI and pelvic organ prolapse occur naturally with aging [16,17]. Similarly, many women acknowledge the benefit of PFME but only during pregnancy or following childbirth [18]. Many women are modest and are reluctant to express concern about PFMD as it involves the genitals [16,19]. Healthcare professionals can play an important role by encouraging patients with PFMD to perform PFME and by routinely screening high-risk women for PFMD [20].
Education on PFME can correct misperceptions, promote motivation, and improve compliance [21-23]. We agreed that antenatal class is the best place to start educating our patients regarding PFME. Therefore, this study was performed to evaluate knowledge of, attitude towards, and practice of PFME among antenatal women before and after an educational class. We also wanted to assess factors that may be associated with PFME practice. Result from this study may be used by policy makers to improve strategies related to management of PFMD. We are hoping that we can develop a proper PFME module in order to educate our patients on prevention and treatment of PFMD in Malaysia.
METHODS
This interventional study was conducted among antenatal women who attended classes in the antenatal clinic, Hospital Universiti Sains Malaysia, Kelantan. The classes were conducted twice a week. The clinic acts as a tertiary referral center from surrounding health centers, district hospitals, private hospitals, and general practitioners, as well as patients who voluntarily attended for evaluation. The study was approved by the research and ethics committee of Universiti Sains Malaysia, Health Campus (USMKK/PPP/JEPeM[220.3.(12)]).
Sample size calculation indicated a requirement for 138 participants for the study. Systematic random 1:3 sampling was applied with a sampling frame in accordance with clinic attendance for follow-up within an 8-week period. Those who fulfilled the inclusion and exclusion criteria were selected. The inclusion criteria were antenatal mothers at 28–32 weeks of gestation with a singleton pregnancy and age greater than 16 years old. The exclusion criteria were illiteracy and inability to understand the Malay language. The selected antenatal women were briefed about the study using an information sheet. After a briefing, signed consent was required to participate in the study.
Data was collected using self-administered validated questionnaires. The questionnaires were divided into two sections. The first section collected sociodemographic data and the second section was on knowledge, attitude, and practice (KAP). The knowledge questions had two sub-domains. The first knowledge domain was about pelvic floor muscle anatomy, function, and the benefits of PFME (12 questions). The second knowledge domain was on the PFME regime (five questions). The attitude domain had eight questions and the practice domain had four questions.
The questionnaire validation study was carried out among 56 antenatal women for face, content, and constant validity. Cronbach alpha was 0.929, 0.877, 0.818, and 0.728 for first knowledge domain, second knowledge domain, attitude, and practice, respectively. Categorical responses (true, false, and don’t know) were used for the knowledge items. For attitude items, a 5-point Likert scale (strongly agree, agree, neutral, disagree, strongly disagree) was used, and similar ordinals (never, seldom, usually, frequent, always) were applied for the practice items.
At baseline, all participants at 28–32 weeks of pregnancy were assessed for knowledge of, attitude towards, and practice of PFME with these questionnaires. The participants then attended two PFME educational classes on their next two antenatal visits at 34–36 weeks and 37–38 weeks, respectively. The class included lectures, demonstrations, and practical sessions. However, techniques of PFME were not examined objectively during the session to ensure correct muscle contraction. Brochures on PFME were distributed for the respondents to take home. At 2 months postpartum, participants had a follow-up visit and the same questionnaires were used for reassessment. Those who were interested were referred to a physiotherapist for objective measurement of muscle strength. Only five patients were referred to the physiotherapist at follow-up. Many participants preferred to practice PFME at home and declined referral.
Data were entered and analyzed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were reported using descriptive statistics including mean and standard deviation or median with interquartile range for non-normally distributed data. Categorical variables were expressed as frequencies and percentages. The results were presented as rho, and a P-value <0.05 was statistically significant. The outcome (dependent) variable was numerical. A paired t-test was used to analyze and compare the mean of KAP pre- and post-intervention. A P-value <0.05 was again statistically significant. Multivariate analysis was used to evaluate sociodemographic factors and the change in practice scores was analyzed using multiple linear regression.
RESULTS
1. Sociodemographic Characteristics
Of 138 women recruited, 17 did not return for follow-up at 2 months, and only 121 completed the study. The response rate for the study was 87.7%. Table 1 shows the descriptive analysis of the sociodemographic data.
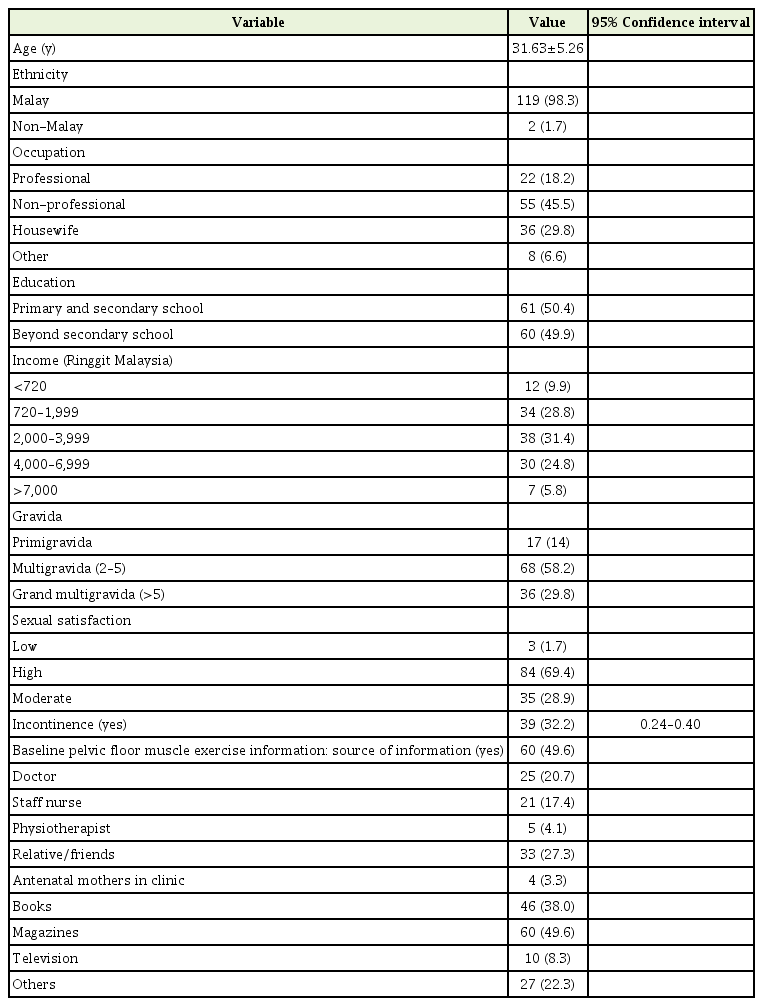
Descriptive profiles of antenatal mothers (n=121)
2. Effect of PFME Education on Knowledge, Attitude, and Practice
Table 2 shows the mean scores for KAP at baseline and 2 months after intervention. The mean±standard deviation (SD) scores for KAP were 24.98±4.56, 24.25±4.92, and 3.51±3.51, respectively, before intervention. The mean±SD scores significantly increased to 29.66±2.73, 28.03±3.09, and 6.90±2.81, respectively, after intervention (P<0.001) (Table 2).

Mean score of knowledge, attitude, and practice before and after pelvic floor muscle exercise intervention (n=121)
3. Knowledge
Table 3 shows the mean knowledge score for PFME on each questionnaire at pre- and post-intervention. The percentage of correct answers and changes in mean knowledge scores are also shown. A significant change was seen in almost all items except for the importance of PFME in sexual activity.

Pre- and post-intervention knowledge score for PFME (n=121)
4. Attitude
Table 4 shows the mean attitude score and the change in mean attitude score by item at pre- and post-intervention. A significant change in attitude was seen from this intervention.
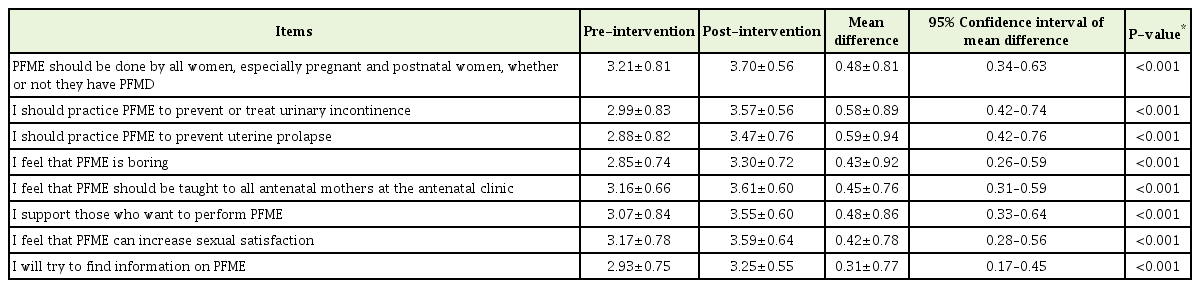
Pre- and post-intervention mean attitude score and change in mean score by item (n=121)
5. Practice
The mean practice score and the change in mean practice score is shown in Table 5. Table 6 shows factors associated with the change in practice score after intervention, using multivariate linear regression.

Pre- and post-intervention mean practice scores and change in mean scores by item (n=121)

Factors associated with change in practice score after intervention, using multivariate linear regression (n=121)
DISCUSSION
1. Sociodemographic Characteristics
The ethnicity of Malaysia is very diverse but the main population is Malay, Chinese, and Indian. Most Chinese and Indians populate the western part of Peninsular Malaysia, whereas Kelantan, situated on the east part of the peninsula, is populated mainly by Malays. A feature of this study is over-representation by the Malay population (98.3%), as the study was done in Kelantan. Therefore, comparison of data cannot be done and the results could not be generalized to all ethnic groups in Malaysia. Similarly, a study in Australia also showed low numbers of non-Caucasian respondents at only 1.3% [15], and 6% in Canada [17].
Respondent mean±SD age was younger at 31.63±5.26 years, as the study was done during pregnancy. This was similar to another study, in which the mean±SD age of respondents was 27.40±6.0 years [15]. Most studies on PFME were done in a non-pregnancy period, in which the main objective was to determine the effect of PFME on UI or KAP in those with UI. Therefore, the age groups were older. Liao et al. [24] in 2006 reported a mean±SD age of 50.3±10.92 and Geoffrion et al. [17] in 2009 reported a mean±SD age of 61.6±11.0.
Of the 121 respondents, 18.2% were professional workers (doctors, lawyers, teachers accountants, architects, etc.), 45.5%% were non-professional workers (clerks, nurses, medical assistants, paramedics), and 29.9% were housewives and others (waitresses, cleaners, babysitters). The proportions of respondents with primary and secondary school educations and those with education levels beyond secondary school were similar. In Malaysia, education is provided until 17 years of age. The proportions with education up to and beyond secondary school in this study were similar to those reported by Whitford et al. [15] However, Geoffrion [25] and Subak et al. [26] reported that a majority of respondents had an education level more than high school. Monthly income was categorized into five levels, based on the poverty line index for West Malaysia in the 9th Malaysia Plan. Only 9.9% of participants were categorized as poor as they had income less than Ringgit Malaysia (RM) 720.
Most respondents in this study were multiparous or grand multiparous, at 56.25% and 29.8%, respectively. This again was expected, as many Malaysian women have more children, in contrast with the findings by Whitford et al. [15], who reported that the proportion of multiparas and primigravidas was the same. This is important, as pregnancy is a major risk factor for PFMD. Being parous, respondents were assumed to know about or practice PFME to a certain extent, but only about half (49.9%) of the respondents in this study had baseline information on PFME before intervention. Many had obtained information from reading. A higher percentage was found by Whitford et al. [15], who found that 90% of antenatal women had some knowledge of PFME from reading magazines and books.
2. The Effect of Pelvic Floor Muscle Exercise Education on Knowledge, Attitude, and Practice
In this study, the mean KAP score was significantly increased at 2 months after intervention (Table 2), showing that an educational class on PFMD and PFME for antenatal mothers is important. Similar improvement of knowledge after an educational class was observed in other studies discussed below. However, few studies on PFME knowledge are available for comparison, and only a few examined the effect of education on PFME knowledge.
3. Knowledge
The knowledge score in the present study improved for most respondents in all aspects of the questionnaires (Table 3). The highest correct answer before intervention was on the importance of pelvic muscles on sexual activity (84.3%). After the intervention, all respondents (100%) answered correctly that PFME may treat or prevent UI and that the exercise can be done at any time.
The highest change in knowledge score was in the response to “PFME is important in controlling urinary bladder function.” The second and third highest score changes were on methods of performing PFME, i.e., “PFME should be done at least 3 times a day, in the morning, afternoon, and night,” and “PFME can be done during routine daily activities.” Other high knowledge score changes were in response to “muscles involved in PFME should be contracted for 8 seconds before being release.” From the highest knowledge score changes, we can conclude that the majority of respondents had poor knowledge of the benefits of PFME in preventing or treating UI, even though many had baseline information on PFME. They also had a low level of knowledge on methods of performing PFME before the intervention. Many were not aware that PFME can be done at any time or place, and in any position.
This study result was supported by Geoffrion et al. [17] Knowledge on pelvic floor health and quality of life improved after 2.5 hours in a pelvic floor health workshop [17]. It was noted that knowledge scores were significantly higher immediately after the workshop (P<0.001) and 3 months late (P< 0.001), when compared with scores before the workshop. Baseline symptoms and quality of life scores significantly improved at 3 months.
Liao et al. performed a study on Taiwanese women with UI. Self-administered questionnaires were completed before and at 8 weeks after a 4-hour educational program that included training on PFME. There was a significant increase in the knowledge score and a decrease in UI symptoms with frequent practice [24].
Another study in Michigan, United States, evaluated the impact of a 2-hour group educational program on the knowledge and practice of PFME among women without PFMD. The participants were followed up after 12 months, and 86% correctly completed the questionnaires [27]. However, as no pre-intervention questionnaires were given in that study, no improvement in the knowledge score can be confirmed and it is unclear whether the high percentage of correct answers was due to the educational class.
4. Attitude
Although, the practice of PFME was low in the present study, the majority of participants had a positive attitude toward learning. In pre- and post-intervention studies, the highest score was for the same item, i.e., “PFME should be done by all women, especially pregnant and postnatal women, whether or not they have PFMD,” with mean scores of 3.21 and 3.70, respectively (Table 4). The highest attitude score changes after intervention were in response to “I should practice PFME to prevent uterine prolapse,” followed by “I should practice PFME to prevent or treat UI.”
The majority of them agreed that all women should practice PFME, even in the absence of PFMD. They also agreed that PFME should be taught to all antenatal mothers by healthcare providers. In contrast to the findings of Liao et al. [24], there was no change in attitude after a 4-hour educational program. Education can change attitude towards PFME and is another key factor that can promote patient motivation and improve compliance with PFME practice. Women also need to know that there is no shame in having PFMD and should seek treatment [28].
One study aimed at improving healthcare provider KAP on reproductive health in Romania showed a significant increase in scores on four out of five selected training themes after a 5-day training course. Improvements from pre-test to post-test were observed in the areas of prenatal care, healthy lifestyles, and breast cancer screening [29]. Even though the study was not on PFMD, it showed that KAP in all aspects of medical care can be improved with an intervention program.
5. Practice
Although the majority of respondents were multiparous in this study, only 5.8% practiced PFME regularly before the intervention (defined as at least 3 times a week, i.e., frequently or always). After the intervention, more respondents practiced PFME regularly, at 37.2% (Table 5). Many factors accounted for a low practice score before the intervention, including lack of information or encouragement from medical staff in promoting PFME during antenatal checkups or before discharge from the postnatal ward.
Before the intervention, most respondents never discussed PFME with friends and never sought information regarding PFME. After the intervention, most began to perform PFME and even performed PFME after delivery. The highest practice score change was in response to “I spent time performing PFME,” followed by “I performed PFME when I was not pregnant.”
Our findings are similar to those of previous studies. Less than 17% of antenatal mothers performed PFME at least once a week during pregnancy [14] and only 54% of participants practiced PFME during pregnancy despite the high number with knowledge of PFME [15]. Chiarelli et al. [18] found that 91% of responders had good knowledge of PFME but only 15.7% performed PFME before pregnancy, while 54.5% had done so during pregnancy.
This study showed that respondents without baseline information on PFME before intervention had a significantly higher practice score change than those with baseline information (Table 6). Women who knew about PFME before the intervention were not interested in practicing PFME more, as they were not motivated by the information given or may had tried PFME in the past with no effect [15]. Baseline information was only reported in a few other studies [15,18]. Most of their respondents had a higher percentage with PFME information but with low practice rates. No practice change was observed in those cross-sectional studies that were limited to knowledge and practice.
Other factors including age, race, occupation, income, education level, gravida status, presence of UI, and level of sexual satisfaction were not found to be significant with regard to practice score changes. This again supports the need for healthcare professionals to educate patients in clinical practice. As we do not know which patients have baseline information on PFME, we need to target all groups of women regardless of sociodemographic background. All women need to attend PFME class during antenatal checkups.
In this study, a higher education level was not associated with greater changes in practice score, similar to the findings of Alewijnse et al. [30] This contradicts the findings of Bo et al. [14], who studied the association between practice of PFME and demographic data. The authors found that those with more education were more likely to practice PFME, while those who smoked daily or were delivered by caesarean section were less likely to exercise [14]. In our study, smoking data were not included, because of the low prevalence of female smokers in Kelantan. We also did not assess the type of delivery that could predispose our respondents to a higher practice score change. In another study, women who reported practicing PFME were also significantly more educated, older, and in paid employment [15].
As many of the respondents were parous antenatal mothers, the probability of having UI or any PFMD was expected to be high. However, the results indicated that being parous was not associated with greater practice of PFME [30]. Similarly, Whitford et al. [15] reported that higher parity was not a good indicator of PMFE practice. However, Bo et al. [14] found that having more children is associated with more PFME practice.
6. Conclusion
The study result was a good indicator of the need for antenatal women to learn and practice PFME. Education is effective in improving KAP of PFME. We recommend greater effort toward increasing awareness of PFME among antenatal women. As healthcare providers, we need to emphasize PFME during antenatal visits as preventive and therapeutic for PFMD. Since a majority of antenatal classes in Malaysia still do not implement PFME programs, we recommend development of a good clinical practice guideline for PFME, to ensure that all healthcare providers are well trained and informed for the benefit of the public.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was funded by an educational grant from the School of Medical Sciences, Universiti Sains Malaysia, Malaysia. The authors thank all the staff in the antenatal clinic and a physiotherapist who was involved in the study.