INTRODUCTION
Avoidable hospitalizations are those hospitalizations that could have been prevented through timely and effective primary health care services [1]. Adequate accessibility and quality of primary health care services reportedly result in decreased avoidable hospitalizations [2-5]. Hospitalizations for chronic conditions such as diabetes, asthma, and hypertension, and acute diseases, such as pneumonia and complicated appendicitis, are considered as avoidable hospitalizations [1,6]. Other factors, such as demographic characteristics, socioeconomic status, health status, and biology, can also affect hospitalizations [3,5,7,8]. For instance, differences between men and women in biology, health status, and healthcare-seeking behaviors can affect hospitalizations [9-11]. Age is a frequently reported factor significantly related to hospitalization, and its influence should be considered alongside gender [5,12]. Simultaneously, exploring the relationship between the population’s demographic characteristics, access to primary health care services, and avoidable hospitalizations can provide policymakers with a comprehensive picture of the effectiveness of policy interventions related to primary health care and evidence regarding the performance of firstlevel healthcare services.
In the Islamic Republic of Iran, public, private, quasi-public, and charity sectors provide healthcare services. Over 93% of second and third level healthcare services are provided by clinics, centers, and hospitals affiliated to the Iran Ministry of Health and Medical Education (MOHME), with other centers affiliated to the Social Security Organization and the private sector [13].
Primary health care networks provide the population with access to public primary health care services, free of charge [14]. Actions towards universal health coverage, first introduced in 2005, resulted in the implementation of the rural family physician program in rural areas and cities with a population of less than 20,000. This reform led to primary care services—provided by family physicians—becoming available for rural residents [15]. Some physicians and midwives were added to the primary health care network over three years as part of the program that was intended to improve access to a more comprehensive, preventive, and outpatient care. Family physicians manage patients referred to them by the “behvarz,” a community health worker at firstline of service that provides and offers primary health care services, including vaccinations, prenatal and postnatal care, growth monitoring, family planning, management of common infectious and chronic conditions, and environmental health services.
Access to primary health care physicians is unequal across rural areas and depends on an area’s geographic distance from the main village. The main villages with rural health care centers have a resident primary health care physician. However, in smaller or farther villages, typically those with health houses instead of healthcare centers, resident physicians are lacking, and primary health care physicians provide services once or twice a month, with an accompanying health team. Residents of satellite villages are forced to travel to villages with health houses to use their primary health care services. Remote villages have the lowest access to primary health care physicians, and can only use the services of physicians who travel to these villages once a month. Therefore, avoidable hospitalizations in the rural areas of Iran’s health system can be an acceptable indicator of access to primary health care physicians and the effectiveness of their services.
The effect of access to family physicians on total and avoidable hospitalizations in Iran has been explored in two previous studies [16,17], but there have been no studies on the differences in the impact of the family physician reform on avoidable hospitalizations in the first year of the program compared to the following years. This study aimed to simultaneously explore the relationship between access to primary health care physicians, demographic characteristics, and avoidable hospitalizations among the rural population in different years following the implementation of the family physician program.
METHODS
A retrospective time-series study was used to determine the relationship between avoidable hospitalizations and age, gender, and access to a primary health care physician. Data on rural resident’s hospitalizations during the 8 years following the family physician program implementation (2006–2013) were gathered in the rural areas of Tehran province, the capital of Iran. The list of diagnostic codes related to avoidable hospitalizations had not been previously determined in any study in Iran; therefore, the literature was reviewed to determine the avoidable hospitalization codes [6,18]. Experts were consulted regarding the correctness of these codes and ways to avoid admissions falling in the category of avoidable hospitalizations. These diagnostic codes were then used as markers of avoidable hospitalizations in other studies in Iran [16,17]. The avoidable hospitalizations’ diagnostic codes used in this study are presented in Appendix 1 and are considered as determinants of the effectiveness and accessibility of primary health care services.
1. Data Sources
Our data, including the diagnostic codes of avoidable hospitalizations based on the 10th revision of the International Statistical Classification of Diseases, gender, age, and address of the hospitalized population and their degree of access to a primary health care physician, were gathered using the various databases of Iran Health Insurance Organization. The individual’s national number was the common factor that allowed us to link the data in these different databases. The Primary Health Care Networks Development Plan of MOHME was used to determine the level of physician access in each village. Villages were divided into four categories based on their level of family physician access. Villages with rural health care centers had the highest physician access, followed by villages with health houses and satellite villages. Remote villages had the lowest level of physician access.
2. Analysis
For a descriptive investigation of avoidable hospitalizations between 2006 and 2013, the percentage of avoidable hospitalizations (out of total hospitalizations) was calculated. This was calculated based on age groups, gender groups, and four different categories of access to a primary physician. Trend series were plotted using Microsoft Excel software version 2016 (Microsoft Corp., Redmond, WA, USA).
To explore the relationship between demographic characteristics, access to a primary health care physician, and avoidable hospitalization, binary logistic regression was estimated separately for each year. We included gender, age, and access to a physician as independent variables and hospitalization as the categorical dependent variable, in the model. The observed outcome for this dependent variable has two possible types (happen or not happens avoidable hospitalization). Some diagnostic tests were conducted after developing the model. The link test was used to ensure that there was no specification error in the estimated model. Additionally, Hosmer-Lemeshow test was used to test the model’s goodness of fit. Collinearity among the various dependent variables was also explored. All analyses were conducted in STATA software ver. 13.0 (Stata Corp., College Station, TX, USA).
RESULTS
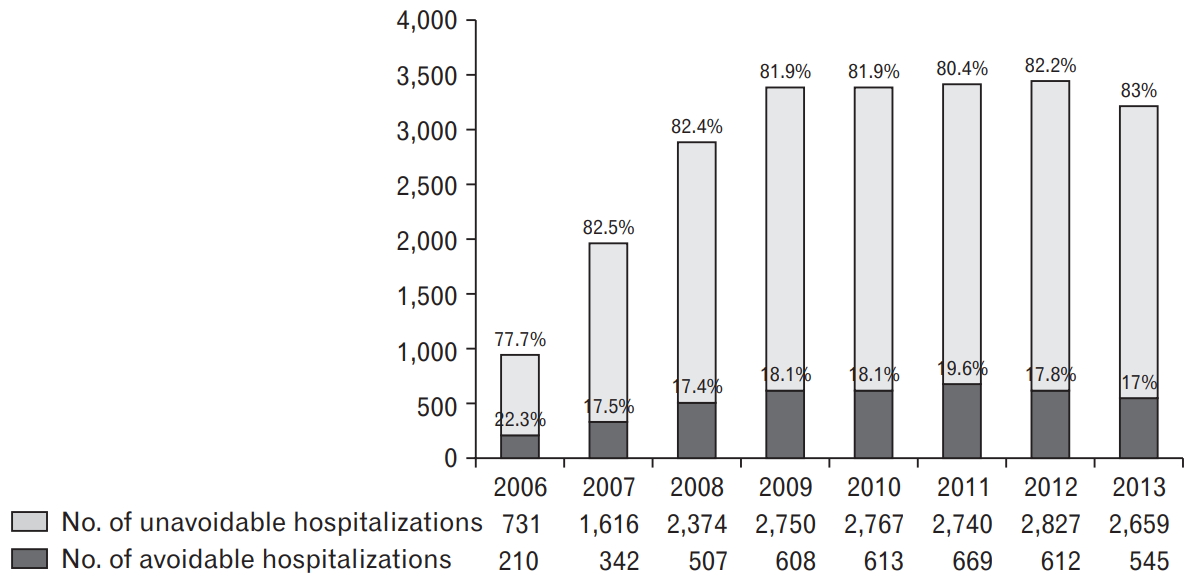
Total and avoidable hospitalizations increased during the study period, especially during the first 3 years of study. However, avoidable hospitalizations, as a percentage of total hospitalizations, did not change significantly throughout the study years. This value was 22.3% during the first year of study and varied between 17% and 19.6% from 2007 to 2013 (Figure 1).
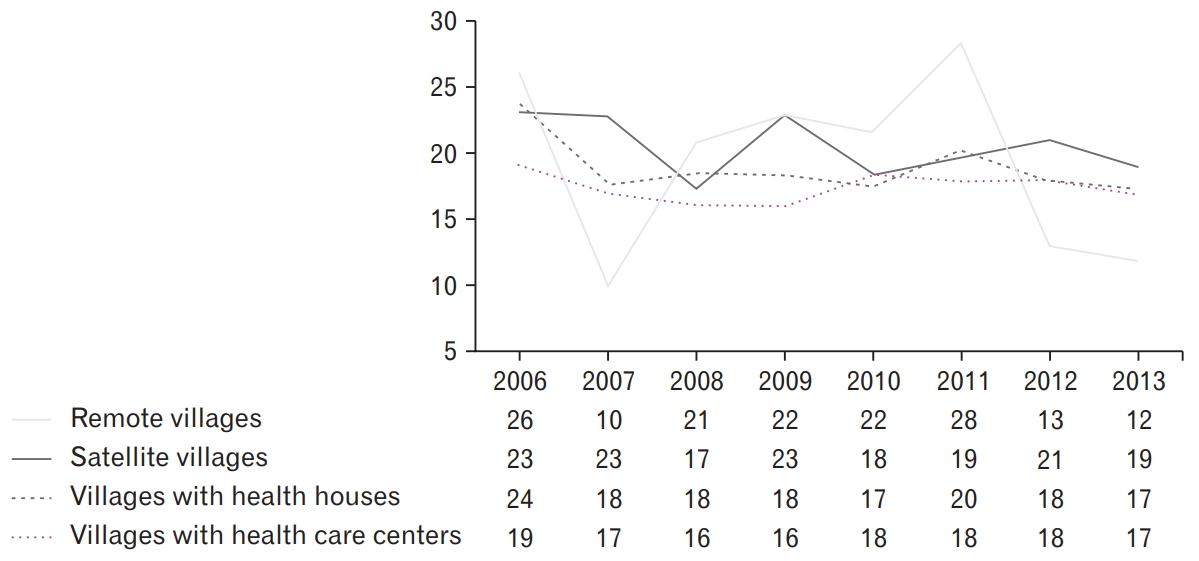
Results show that among the four categories of villages, remote villages had the highest variation in the percentage of avoidable hospitalizations during the study period. It is necessary to mention that the populations of these villages are considerably lower than in other rural areas; therefore, small changes in hospitalizations can have a large effect on the shape of the figure trend. Figure 2 presents the percentage of avoidable hospitalizations among total hospitalizations in different rural areas.
Comparing the percentage of avoidable hospitalizations between men and women showed that this value is higher among men. During the study years, this percentage remained relatively stable among men, while showing a decrease among women. This decrease began one year after the implementation of the family physician program. However, this percentage remained stable for 8 years after the reform implementation (Figure 3).
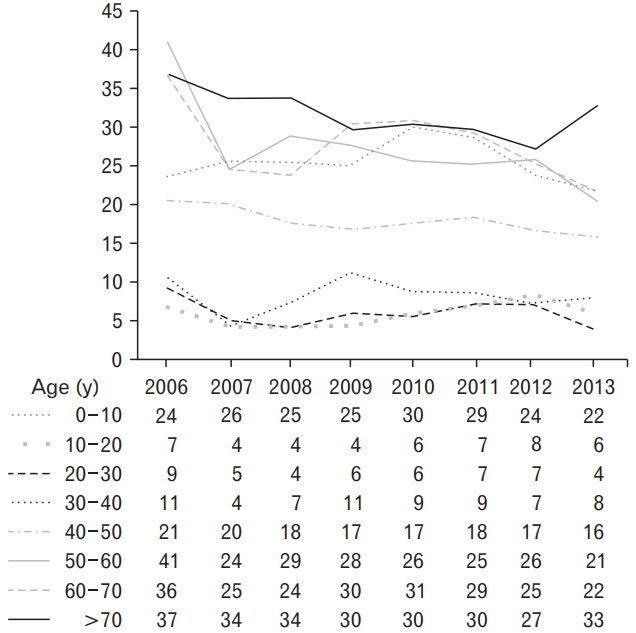
Figure 4 displays the comparison of the percentages of avoidable hospitalizations among different age groups. The highest percentage of avoidable hospitalizations is seen in the >70 age group, while it is lowest in people aged between 10 and 30 years.
Table 1 presents the logistic regression analysis for each year. In this model, the dependent variable is the occurrence of avoidable hospitalizations, and the independent variables are age, gender, and level of access to a primary health care physician. No statistically significant relationship was found between avoidable hospitalization occurrence and physician access during the study years. Throughout the study, the probability of avoidable hospitalizations in the >70 years age group was higher as compared to 10–50 years. In some time periods, the probability of avoidable hospitalizations among those aged >70 years was higher than the 1–10 years and 50–70 years age groups. Exploring the relationship between gender and avoidable hospitalizations showed that the probability of avoidable hospitalization among women was lower than men in the years 2009, 2010, and 2012 (Table 1).
DISCUSSION
This study explored the relationship between access to a primary health care physician and avoidable hospitalization among the rural population during the 7 years following the implementation of the rural family physician program. No significant relationship was found during the study years. Simultaneously, the relationship between demographic characteristics and avoidable hospitalization was investigated, which showed that avoidable hospitalizations were significantly higher among >70 years age group than younger age groups throughout the study. Avoidable hospitalizations were also higher among men than women; however, this finding was only significant in three of the study years.
Another study conducted in Tehran province to explore the relationship between family physician access and avoidable hospitalization following the rural family physician program showed that access to a physician is not related to avoidable hospitalizations [17]. In our study, this relationship was explored over several years, however, the results had not been segregated based on year in the previous study. Both studies yielded similar results.
Theories suggest that health systems that rely more on primary health care and primary care physicians result in better health outcomes for the population and also decrease the costs of unnecessary and avoidable hospitalizations [19]. However, based on the results of these two studies, it appears that the gate-keeping function of the primary health care physician aimed at preventing unnecessary services such as avoidable hospitalization has not been implemented accurately in the family physician program. Therefore, investigating the flaws in the implementation of this program that led to this effect may be worthwhile.
Additionally, our results differ from other studies that evaluated the effects of the rural family physician program on total hospitalizations across Iran and showed a significant increase in both short- and long-term hospitalizations [20]. This difference in results may be because the nationwide study did not separate the effect of the family physician program on avoidable and referral sensitive hospitalizations, or due to the previous study’s quasi-experimental design.
Besides, our results are in contrast with other before-and-after studies conducted in one of the counties in Tehran. Study results at the county level revealed that increasing access to primary care physicians resulted in a decrease in avoidable hospitalizations [16]. Therefore, a difference exists in the relationship between access to a primary care physician and avoidable hospitalizations at the province and county level. This may be due to the differences in the demographic, social, and economic characteristics of the rural population in the studied county in comparison with the whole of Tehran province. Therefore, it is better to consider other factors that may influence this issue.
Studies exploring the relationship between avoidable hospitalizations and access to a primary care physician in other countries show different results. In Ukraine, pediatric hospitalization rates for some preventable conditions were positively related to the availability of a primary care physician [21]. In Canada, after adjusting for age, sex, and comorbidity, an increased rate of emergency department use was associated with the lack of a primary physician among people aged 65 years and older [22]. In the United States, physician supply was not associated with avoidable hospitalizations in rural areas [23]. In another study conducted in the United States, physician supply and distribution had little effect on avoidable hospitalization rates [24]. Based on these studies, the effect of access to a primary health care physician on avoidable hospitalizations appears to be different in various health care systems with different financial systems, different payment methods to providers, and different populations under study.
The Health Information System in Iran does not hold data on the presence of simultaneous diseases, patient’s disease history, their income and job situation, or their economic classification. Considering these variables alongside demographic variables can present a more comprehensive picture in determining the relationship between access to a physician and hospitalizations. However, it can be said that rural areas with lower access to physicians have a lower economical and welfare status in this study, although this cannot be claimed confidently.
In our study, we did not consider the structural and organizational aspects of the primary health care physician program through which the physicians provide services when exploring the relationship between physician access and hospitalization. However, according to the results of other studies, these characteristics may affect avoidable hospitalizations. For example, in Sweden, general practitioner visit rates were negatively associated with hospitalization rates, considering the country’s socioeconomic status health care structure [25]. In Taiwan, which has a system with higher access to health care, continuity of care resulted in decreased avoidable hospitalizations [26]. In Canada, high continuity of care was associated with reduced odds of ambulatory care-sensitive hospitalizations controlling for demographic and self-reported, health-related measures [27]. Based on a systematic review, a powerful primary health care system with access to primary care physicians and long associations between the physician and patient reduce the probability of avoidable hospitalization [3].
Therefore, health policymakers need to consider the structural and organizational aspects (such as disease management guideline development, continuity of care by physicians, types of service providers, etc.) when developing similar programs. Examples include the urban family physician program, which is the current agenda in Iran. This may help health policymakers to decrease costs and hospitalizations.
In our study, we found that elderly people (>70 years) were more likely to undergo avoidable hospitalizations. Our results were consistent with other studies. In the United States, avoidable hospitalizations in people younger than 65 years were significantly lower than older age groups [28]. In Italy, avoidable hospitalizations were higher among the elderly and increased with lower levels of access to primary care physicians [29]. Higher avoidable hospitalizations among the elderly may be reasonable, given the higher rates of chronic conditions among this age group. Therefore, access to a primary care physician can reduce the need for hospitalization among older adults. Health policymakers should, therefore, pay special attention to provide the elderly with primary health care services to prevent future costs related to avoidable hospitalizations. This issue is of special importance in rural areas, where access to higher levels of health care is more complex.
In our study, a statistically significant difference was found in hospitalization among the sexes, with avoidable hospitalizations being higher in men compared to women throughout the study. A previous study in Tehran assessing the relationship between hospitalization, demographic characteristics, and access to physicians reported higher avoidable hospitalizations among men. However, these relationships were not simultaneously explored based on a time-series [17]. In Norway, elderly women were hospitalized less frequently than men, while elderly women in Finland were more likely to use all health care services than men, except for hospital care services [30]. In both Spain and Italy, avoidable hospitalization rates among men were reportedly higher than women [1,11].
Previous studies generally report higher use of health care services among females during their reproductive years. This is later reversed, with elderly men using health care services more than women. These results could be explained by differences in health status, care-seeking behavior, and care provisions among men and women. Their working time as farmers could be another cause of higher avoidable hospitalizations among rural men in comparison with women in this study. Time limitations imposed on males by their jobs in farming implies that they have less time to access services provided by primary health care physicians.
Our study provides valuable evidence that can be used when developing similar reforms in Iran and other developing countries. Implementation of the urban family physician program is currently on the agenda, and our results suggest that policymakers should pay greater attention to the urban population’s demographic characteristics and their possible effects on the patients’ use of physician and hospital services.
In conclusion, data analysis over several years following the primary health care reforms revealed that increasing access to primary health care physicians cannot, by itself, result in decreased avoidable hospitalizations. Therefore, policymakers need to consider the different factors and aspects of structure and organization when developing and implementing new interventions in primary health care to promote the performance of this level of health service provision.