Nicotine Dependence Evaluated by Urinary Cotinine and Heaviness of Smoking Index among Smokers, Vapers, and Dual Users: A Cross-Sectional Study Using the Korea National Health and Nutrition Examination Survey Data
Article information

Abstract
Background
Many people use both combustible cigarette (CC) and electronic cigarette (EC). We compared nicotine dependence among CC, EC, and dual users using questionnaires and urinary cotinine levels.
Methods
Data from the Korea National Health and Nutrition Examination Survey (2014–2017) databases were analyzed; 3,917 CC, EC, and dual users were administered the urinary cotinine test, and 1,045 current CC and dual users completed the Heaviness of Smoking Index (HSI) questionnaires. Weighted geometric means of urine cotinine levels were compared between exclusive CC, exclusive EC, and dual users. The distribution rate, based on time to first cigarette (TTFC), cigarettes per day (CPD), and the HSI was analyzed in two weighted groups, exclusive CC and dual users.
Results
Among those who currently use any type of cigarette, 89.4%, 1.4%, and 9.2% were exclusive CC, exclusive EC, and dual users, respectively. Weighted geometric means of urine cotinine were highest in dual users (1,356.4 ng/mL), followed by exclusive CC (1,270.3 ng/mL), and exclusive EC (867.7 ng/mL) with significant differences between all three groups (P<0.05). There were no statistically significant differences in CPD between exclusive CC and dual users (P=0.626). The proportion of TTFC ≤5 minutes was 21.5% and 29.5% in the two groups, respectively (P=0.010); however, HSI differences in the two groups was marginal (P=0.557).
Conclusion
In this study, the urinary cotinine value could distinguish the three groups, CC, EC, and dual users, but the questionnaire using HSI could not distinguish the three groups.
INTRODUCTION
Since their development in China in 2003, battery-powered electronic cigarette (EC) devices that evaporate liquid nicotine solutions have been popular in many countries, and the usage rate varies from country to country. For example, the rate of daily adult EC use is 4.2% in the United Kingdom and 2.8% in South Korea with less restrictive use policies, while it is 2.1% in Canada and 0.4% in Brazil with more restrictive policies [1]. The long-term health effects of ECs is still controversial [2]; however, their popularity is increasing in many countries. The prevalence of male adult tobacco smoking in South Korea has declined from 66.3% in 1998 to 36.7% in 2018, the lowest rate since 1998 [3]. However, the prevalence of male adult electronic cigarette use in Korea has increased from 2.0% in 2013 to 4.4% in 2017 [4].
According to previous cross-sectional studies [5,6], the most common reasons for EC use were smoking cessation and less harmful health effects than combustible cigarettes (CC). The short-term health effects of ECs are known to be less harmful than those of CCs; however, evidence is still lacking on its long-term health effects and the efficacy of ECs as a smoking cessation aid is unclear [2].
The main reason for smoking cessation failure is associated with the level of nicotine dependence, which also applies to EC users. Nicotine dependence is mainly evaluated using questionnaires and urinary cotinine levels. In previous studies that evaluated the nicotine dependence level of dual users, the difference between CC users and dual users was controversial [7,8]. According to the study, the questionnaire findings and salivary cotinine levels of 375 exclusive CC and dual users were compared [7]. Cigarette consumption and salivary cotinine levels did not differ significantly between the two groups. In contrast, another study on nicotine dependence in poly-tobacco users in the United States presented different results [8]. Poly-users showed greater nicotine dependence than sole-product tobacco users. For example, poly-users were more likely to report dependence symptoms than single type users.
Appropriate evaluation of nicotine dependence is an important part of smoking cessation consultations, the Heaviness of Smoking Index (HSI) consists of two of the Fagerström Test for Nicotine Dependence (FTND) items, cigarettes per day (CPD), and time to first cigarette (TTFC). According to a report by Pérez-Ríos et al. [9] on FTND and HSI relevance, there was considerable agreement between the HSI and FTND, with a kappa value of 0.7 and 96.2% specificity.
Cotinine is a major metabolite of nicotine, with a longer half-life (20 hours) than nicotine (2 hours), and is easily detected in the urine, plasma, and saliva. It is widely used as a biomarker for more accurate assessments of smoking status in research, including epidemiological studies [10]. Cotinine is present at a high concentration in urine and, thus, can be detected accurately [11]. The validity of the urine cotinine test for predicting nicotine dependence has been demonstrated in a previous study [12]. Therefore, the urine cotinine test can be used to evaluate nicotine dependence and complement the objectivity of the survey for both CC and EC users.
This study aims to compare nicotine dependence among exclusive CC, EC, and dual users using the HSI and urine cotinine as a biological marker. The Korea National Health and Nutrition Examination Survey (KNHANES) database, which includes a nationally representative sample, provides the opportunity to assess dependence among the three groups.
METHODS
1. Research Plan
This study used raw data from the sixth (2014–2015) and seventh (2016–2017) KNHANES surveys of a representative sample of the Korean population, conducted by the Korea Centers for Disease Control and Prevention since 1998, using a two-stage stratified sampling method [13]. The sampling plan for the KNHANES is based on a stratified, multi-stage, clustered probability design to create a group representative of the Korean population. The KNHANES collects data annually on 23 target households from each of the 192 primary sampling units. A total of about 10,000 household members, aged 1 or older, are surveyed. This method uses systematic sampling based on sex, age, and geographic area. The total number of respondents was 31,207 for KNHANES-VI (second year: 2014, 7,550; third year: 2015, 7,380) and KNHANES-VII (first year: 2016, 8,150; second year: 2017, 8,127). Questionnaire surveys related to ECs have been included since 2011, and the assessment of nicotine dependence was included in 2016 only. For the present study, ethical approval was not required because the KNHANES data are publicly available.
2. Study Participants and Data Collection
Among the questionnaire respondents, those who indicated that they used CCs or ECs were included. A total of 1,916 people without smoking history information, and 5,980 people without urine cotinine values were excluded; thus, 23,311 people were analyzed. Current smokers were categorized into three groups: exclusive CC, exclusive electronic cigarette, and dual users. For the analysis of urine cotinine values, 82 people who received nicotine replacement therapy (NRT) within 5 days were excluded. An additional 19,312 never- and former smokers were also excluded. As a result, 3,917 people were included in the urine cotinine analysis with further analyses of smoking cessation attempts and motivation to quit smoking using the transtheoretical model (TTM) [14]. For the CPD analysis, 52 exclusive EC users were excluded. A total of 2,820 people who did not complete the TTFC survey (only conducted in 2016) were excluded from the HSI analysis (Figure 1).
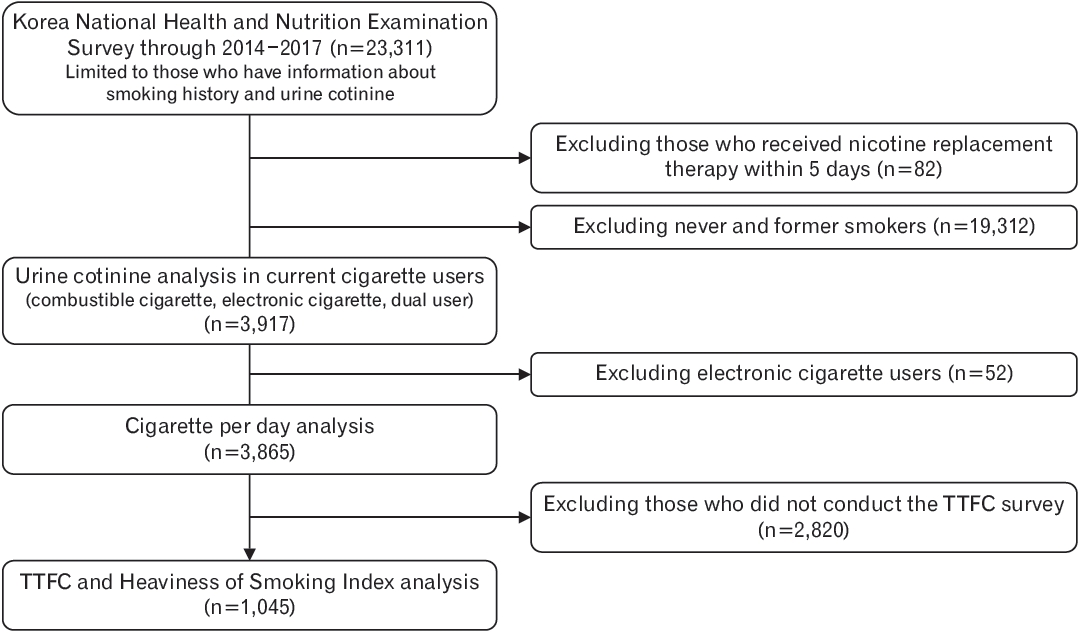
Flowchart: study population. TTFC, time to first cigarette.
Respondents who answered, “daily or sometimes” to the question, “Do you currently smoke?” were categorized as CC users. Respondents who answered “yes” to the question, “Have you used electronic cigarettes in the last month?” were categorized as EC users. Respondents who answered “yes” to both questions were categorized as dual users. Given the above classifications, CC and EC users were classified as “current,” “former,” and “never use,” respectively. When the three types of usage in these two groups are combined, respectively, we obtain a total of nine cases, depending on CC and EC usage status. Based on the number of cases above, we classified them into three groups; exclusive CC user, exclusive electronic cigarette user, and dual user.
3. Definitions of Variables
1) Urine cotinine
Urine cotinine analyses were performed in the three groups. Urine cotinine concentration (ng/mL) was measured using gas chromatography-mass spectrometry, using the Clarus 600/600T (Perkin Elmer, Waltham, MA, USA), and the detection limit was less than 0.27399 ng/ mL [15]. Eighty-two respondents who answered “yes” to the question, “Did you use a nicotine replacement product such as a nicotine patch, nicotine gum, or nicotine candy in the last 5 days?” were excluded from the analysis because NRT may affect urine cotinine levels. Never and former smokers (n=19,312) were also excluded. A total of 3,917 respondents were analyzed for urinary cotinine values. The samples were not normally distributed; therefore, the results are presented using geometric mean (GM) values to compare the weighted mean among exclusive CC, exclusive EC, and dual users.
2) Nicotine dependence
This study excluded exclusive electronic cigarette users from the HSI analysis because the CPD unit measure is based on CC use and does not include a measurement unit for EC use. When asked, “How many cigarettes do you smoke per day?”, the CPD item was divided into four groups: 10 cigarettes or less, 11 to 20 cigarettes, 21 to 30 cigarettes, and more than 30 cigarettes. The groups were scored from 0–3 points, respectively. To evaluate TTFC values, those who did not conduct the TTFC survey were excluded (n=2,820) as the TTFC question was only included in the 2016 survey. The TTFC item was assessed by asking, “How soon after you wake up do you smoke your first cigarette in the morning?” and was also divided into four groups: within 5 minutes, 6 to 30 minutes, 31 minutes to 1 hour, and more than 1 hour. The TTFC was scored from 3–0, respectively. The HSI item is calculated as the sum of CPD (0–3 points) and TTFC (3–0 points) scores and is divided into three categories: mild (0–1 points), medium (2–4 points), and high (5–6 points), according to the criteria set forth by the National Institute on Drug Abuse in the United States [16].
3) Smoking cessation attempts and motivation to quit smoking according to the transtheoretical model
Additional smoking-related variables, smoking cessation attempts, and motivation to quit smoking were evaluated using the TTM. Smoking cessation attempts were evaluated in response to the question, “Have you stopped smoking for more than a day (24 hours) in an attempt to quit smoking in the past year?” Motivation to quit smoking was evaluated using the question, “Do you have plans to quit smoking in the next month?” Respondents who answered, “I have plans to quit smoking in 1 month” were categorized as “preparation stage” and the rest as “others.”
4) Sociodemographic factors
Age, sex, education level, income level, marital status, and high-risk alcohol use were analyzed. High-risk alcohol use was defined as an average of more than seven glasses for men or more than five glasses for women more than twice a week, according to the KNHANES standards [17]. The high-risk alcohol use rate for each type of cigarette user was compared.
4. Statistical Analysis
Chi-square tests were used to identify the relationship between the type of tobacco product and smoking-related sociodemographic factors such as sex, education, quartile of monthly household income, marital status, and high-risk alcohol drinking. One-way analysis of variance (ANOVA) was used for the average age of each group. Because the urine cotinine values were not normally distributed, the GM was used and an ANOVA test was conducted. The chi-square test was used to analyze the nicotine dependence questionnaires (CPD, TTFC, and HSI) between exclusive CC and dual users. STATA ver. 15.0 (Stata Corp., College Station, TX, USA) was used for statistical analyses, and P-values <0.05 were considered statistically significant.
RESULTS
1. Characteristics of Participants
The respondents’ demographic characteristics are presented in Table 1. Out of 3,917, 89.4% were exclusive CC users, 1.4% were exclusive EC users, and 9.2% were dual users. Exclusive CC users were the oldest, followed by exclusive EC and dual users. The majority of exclusive CC users (about 69.2%) were in their 30s to 50s, while the majority of exclusive EC users (about 68.0%) and dual users (about 68.4%) were in their 20s to 30s. Males accounted for more than 80% of all three groups. The three groups of current cigarette users were analyzed by sex. The results showed that exclusive EC users accounted for 1.4% of male current cigarette users and 1.9% of female current cigarette users. Dual users accounted for 9.4% of male current cigarette users and 7.6% of female current cigarette users. Male exclusive EC and dual users were mainly in their 20s and 40s, while female exclusive EC and dual users were in their 20s and 30s.

Characteristics of study populations
Regarding participants with education beyond high school, 56.6% were exclusive EC users, 38.8% were exclusive CC users, and 39.1% were dual users. Among dual users, the rate of those in the top 50% income level was 75.3%, which was higher than that of exclusive CC users (61.7%) and exclusive EC users (61.0%). A higher percentage of participants were married in all three groups. The rates among the three groups of high-risk drinking (P=0.131), smoking cessation attempts (P=0.116), and TTM for motivation to quit smoking (P=0.080) were no statistically significant. The weighted GM of urine cotinine was highest in dual users, followed by exclusive CC and exclusive EC users (P<0.001) (Table 1).
2. Comparison of Nicotine Dependence Using Urine Cotinine Values
The weighted GM of urine cotinine was highest in dual users (1,356.4 ng/mL), followed by exclusive CC users (1,270.3 ng/mL, standard error=17.9), and exclusive EC users (867.7 ng/mL) (Figure 2). The missing standard error is due to the stratum with a single sampling unit in the exclusive EC and dual user group. The GM of urine cotinine, based on the type of cigarettes used, was significantly different between the three groups, according to an ANOVA test (P<0.001). The unweighted median GM of urine cotinine was highest in dual users (1,248.1; interquartile range [IQR], 756.5–1837.0), followed by exclusive CC users (1,164.2; IQR, 613.4–1,735.6), and exclusive EC users (356.7; IQR, 4.9–1,694.0).
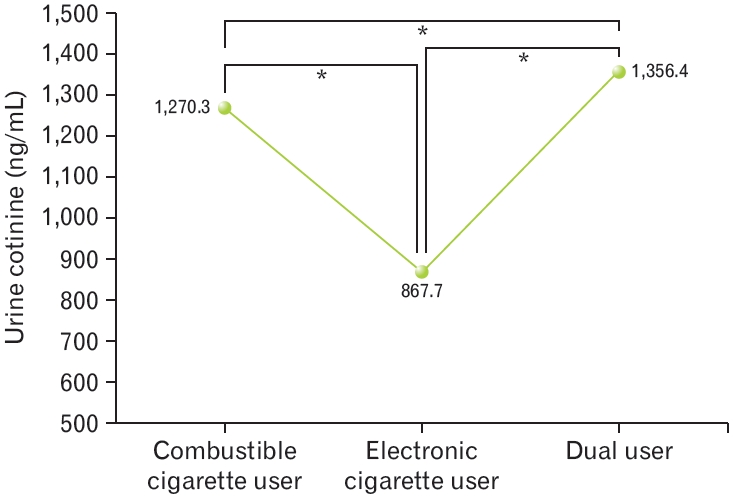
Geometric mean of urine cotinine analysis in current cigarette users. P-value from analysis of variance for urine cotinine geometric mean. *P<0.05.
3. Nicotine Dependence Analysis Using the Heaviness of Smoking Index Questionnaires
In the exclusive CC and dual user groups, more than 90% of respondents used less than a pack of CPD. The proportion of the two groups who smoked more than 30 cigarettes was similar, with 1.7% for exclusive CC users and 1.5% for dual users; however, the CPD item score was not significantly different (P=0.626).
Among 29.5% of dual users and 21.5% of exclusive CC users, the TTFC was within five minutes of waking (P=0.010). When the HSI was divided into three categories according to score (mild, medium, and high), approximately 4.3% of CC users and 5.5% of dual users had a high score (Table 2). Analysis of urine cotinine, cigarette per day, TTFC, and HSI by gender is presented in the supplementary table (Supplementary Table 1).

Comparison of nicotine dependence using Heaviness of Smoking Index between exclusive cigarette smokers and dual users of cigarette and e-cigarette
DISCUSSION
The GM of urine cotinine was highest among dual users, followed by exclusive CC users and exclusive EC users, and the differences between the three groups were statistically significant. The differences in the average CPD and HSI scores were not statistically significant among exclusive CC and dual users. Although the urine cotinine analysis showed differences in nicotine dependence between the three groups, the differences were not clear in the survey questionnaire.
Both the HSI questionnaire and urine cotinine test have validity in assessing nicotine dependence; therefore, the survey results, indicating no difference between the three groups, could be questioned. This may be due to the fact that the KNHANES does not contain a detailed questionnaire on EC use. (e.g., EC use frequency, number of puffs, nicotine concentrations, vaporizing power, flavors, etc.). When we analyzed the correlation coefficient between urine cotinine and CPD, TTFC, and HSI scores (the correlation analysis results of the GM of urine cotinine and CPD, TTFC, and HSI were not provided in the results), we found that the correlation coefficient between urine cotinine and CPD (β=0.4093, P<0.001) was the lowest compared to that of TTFC (β=0.4312, P<0.001) and HSI (β=0.4435, P<0.001). In the HSI questionnaire, the TTFC is likely to be relatively useful in developing nicotine dependence over a short period of time.
The assessment of nicotine dependence in dual users is likely to be affected by the type of cigarette (CC, EC, or dual use) the respondents use at the time of analysis. However, measuring the frequency of use of each cigarette type is important when assessing nicotine dependence. Martinez et al. [18] observed changes in nicotine dependence in dual users through self-reported data of CC and EC use and retrospective recall of pre-vaping smoking. Interestingly, after dual-use, nicotine dependence was evaluated by the sum of cigarettes and vaping sessions per day. The study findings of Martinez et al. [18] are similar to that of the present study, where dual users reduced the number of CCs, but total nicotine use and dependence increased. Meanwhile, a study by Morean et al. [19] evaluated nicotine dependence of CCs and ECs among dual users using the four-item Patient-Reported Outcomes Measurement Information System (PROMIS) Nicotine Dependence Item Bank and the four-item PROMIS Nicotine Dependence Item Bank for E-cigarettes (PROMIS-E). Their analysis found that the nicotine dependence of CCs and ECs was related, but separate from each other (r=0.35); meaning, dual users use the two products separately. Increased nicotine dependence in the cigarette they mainly used has been shown in relation to an increased frequency of that cigarette’s use. Additionally, in a report by Vogel et al. [20] on nicotine dependence associated with ECs among adolescents, the frequency of EC use (session per month; r=0.58, P<0.001), and the level of addiction (EC Addiction Severity Index; r=0.51, P<0.001) to ECs, had higher correlation with urine cotinine than other factors.
This study has several limitations. First, it is difficult to identify whether dual use causes greater nicotine dependence or vice versa as this was a retrospective, cross-sectional study. Also, since the transition of cigarette use could not be identified, it was not known whether an EC user switched from CCs in the past or started ECs anew. In this study, “Help quit smoking tobacco” was the first reason for the use of ECs analyzed for exclusive EC users (56.3%) and dual users (43.0%). In terms of dual users, 64.7% have tried to quit smoking for more than 24 hours in a year. In future research, longitudinal studies on cigarette use patterns, including transition, are needed to understand the causal effect of dual use on nicotine dependence.
It is meaningful to assess nicotine dependence on each cigarette type using the KNHANES data, considering the growing number of dual users among EC users. Several studies have evaluated EC users’ nicotine dependence; however, nicotine dependence has not been assessed using biochemical markers [21-23]. In contrast, in this study, urine cotinine was tested so that nicotine dependence could be assessed more objectively than would have been possible with a questionnaire alone.
Currently, EC technology is developing gradually, and future devices are likely to deliver high-concentration nicotine more efficiently. Moreover, the number of new types of cigarettes, including electronic cigarettes and heat-not-burn tobacco products, is increasing. Developing new evaluation tools to measure nicotine dependence among dual and poly-users is essential. In a report of Vogel et al. [20], frequency measurement, such as days per month, was useful in evaluating EC users’ degree of addiction more easily. In a report of Martinez et al. [18] in order to compare the change in nicotine dependence after the onset of vaping, the pre-vaping CPD measurement was used. They added the value of vaping sessions per day on the CPD item during post-vaping. Dual users tend to discriminate their use of each product [20]; therefore, it is necessary to assess nicotine dependence by frequency and severity on each type of cigarette used by dual or poly-users, separately.
In conclusion, this study compared and analyzed nicotine dependence according to urine cotinine values and the HSI questionnaire, using KNHANES data, among exclusive CC, exclusive EC, and dual users. Dual users had significantly higher urine cotinine levels than the others. The differences in nicotine dependence among the three groups were revealed by the urine cotinine analysis; however, the difference was not clear in the survey questionnaire. It may not be possible to distinguish differences in nicotine dependence through the HSI questionnaire alone. However, the TTFC item in the HSI items can be useful in developing nicotine dependence in dual users over a short period of time. The smoking cessation consultations for dual users need to be more strategic. New evaluation tools are needed to assess the amount of smoking and nicotine dependence of dual users or poly-users more efficiently.
Notes
CONFLICT OF INTEREST
No potential conflicts of interest relevant to this article were reported.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4082/kjfm.20.0056.
Analysis of urine cotinine, cigarette per day, TTFC, and Heaviness of Smoking Index by gender