INTRODUCTION
Balance is an interrelated component of physical function and is defined as the ability to align body segments against gravity to maintain or move within the available base of support [1]. In particular, mechanoreceptors are located within the joint capsular tissues, ligaments, tendons, muscles, and skin of the ankle and provide essential information to enable adjustment of ankle positions, which play a major role in the maintenance and correction of balance in different directions during weight-bearing activities [2].
Superior balance ability is necessary to avoid lower limb injuries and achieve the highest competitive level. Many researchers have attempted to improve balance by applying appropriate interventions to the ankle in healthy individuals and athletes [3]. Kinesio taping (KT) is a popular elastic taping method with proposed mechanisms of action such as improved proprioception through increased stimulation of cutaneous mechanoreceptors, altered muscle function by supporting weakened muscles, and repositioned joints by mechanical correction [4].
Several application techniques of KT have been suggested according to its purpose. For instance, muscle technique is used to alter muscle activation, mechanical correction is suggested to reposition the joints, and the epidermisŌĆōdermisŌĆōfascia technique aims to improve wound healing and edema [5]. Researchers commonly used muscle techniques since they were mainly focused on investigating the effects of KT on muscle function and strength, and studies on the effects of mechanical corrections are limited. The mechanical correction method of KT on the ankle was thought to have an effect similar to that of joint mobilization [6]. Since it was proposed that articular stretching due to joint mobilization on the ankle increases sensory outputs of the mechanoreceptors, which are related to balance [7], we anticipated that mechanical correction may change balance parameters.
The effects of KT on variables such as muscle strength, pain, range of motion (ROM), and balance in people with ankle disorders have previously been investigated [8]. However, it is essential to differentiate the effects of KT from those of placebo and the normal healing process of the disease itself. To reveal the pure effects of KT, the present study was conducted in healthy individuals as a sham-controlled trial. This study aimed to determine whether the mechanical correction technique of KT applied to healthy ankles immediately affected balance, ROM, and muscle strength. We hypothesized that KT would significantly change balance in individuals with healthy ankles when compared with sham application. The results of this study would be useful for clinicians in making clinical decisions regarding the use of KT in healthy individuals and athletes when balance improvement is desired.
METHODS
1. Design
This prospective, randomized, double-blinded, sham-controlled study with a parallel design, with an allocation ratio of 1:1, was conducted between January and May 2018. The Dokuz Eyl├╝l University Ethics Committee for Non-Invasive Human Research approved this study (date 01.03.2018). The ID and protocol numbers of the ethical reports are 3538 GOA and 2018/0617, respectively. The procedures were performed in accordance with the Declaration of Helsinki. All participants provided written informed consent prior to enrollment.
2. Participants
Forty healthy students aged 18ŌĆō25 years volunteered for the study. Participants were recruited from a local university. Participants with (1) any neurological, musculoskeletal, or vascular disease; (2) previous history of surgery in any of the lower extremities; and (3) previous experience with KT were excluded.
Participants were randomly allocated to the experimental KT group and the sham KT group, and block randomization (AABB, ABAB, ABBA, BBAA, BABA, BAAB paradigm) was used. A is the experimental group and B is the sham group. Participants were assigned to one of the two groups using this paradigm by an independent investigator. To ensure blinding, the paradigm was concealed in a sealed envelope and provided to each participant. Participants were then asked to give the sealed envelope only to the researcher who would be performing KT before the intervention.
Outcome measures were evaluated by a blinded assessor before and 45 minutes after the intervention procedure in a different hall from where the interventions were applied. Participants were not informed about the intervention that would be applied during data collection. All measurements were taken at the same time of the day.
3. Procedures
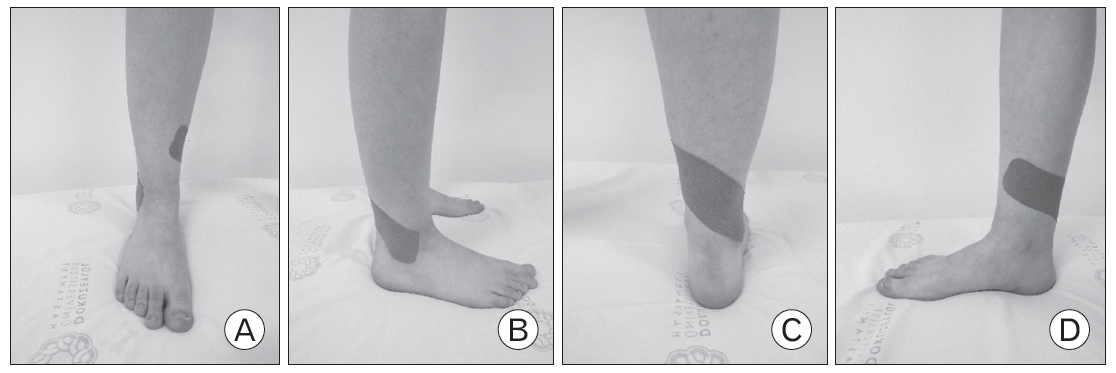
KT was applied according to the procedures recommended by Kase et al. [5]. A 5-cm wide, pink Kinesio Tex tape was used for both groups. For the experimental KT group, a posterosuperior glide was first manually applied to the distal end of the fibula (lateral malleolus). To sustain this glide, the mechanical correction technique of KT was used for both ankles [5]. For each ankle, participants were asked to stand barefoot, and the foot that would be taped was positioned on a tool 30-cm high in neutral position. An I-shaped Kinesio tape with 75%ŌĆō100% stretch (20 cm in length) was applied around the lower leg, attaching from the lateral malleolus to the middle third of the medial tibia (Figure 1). A tension of 75%ŌĆō100% has been suggested to provide sensory stimulation and mechanical assistance to facilitate motion [5]. Once applied, the physiotherapist warmed the tape by rubbing his hand three times throughout the tape to maximize tape adhesion.
To simulate the experimental taping technique with an eliminated mechanical effect for the sham KT group, the tape was applied in the same manner, but without tension and any glide to the fibula. A longer I-shaped tape (28 cm in length) was used as it was not stretched and did not cover the same distance on the skin of participants in the experimental KT group. The same technique was applied to other ankles.
4. Baseline Measurements
The demographics of participants were noted. Leg dominance was determined by instructing participants to kick a soccer ball. In this study, the physical activity (PA) level of the participants was evaluated as it could be a confounding factor for the results. Therefore, the Turkish version of the International Physical Activity Questionnaire Short Form was used to determine PA levels. The short form has nine items and provides data on PA in the last 7 days at four intensity levels: (1) vigorous-intensity activity such as aerobics, (2) moderate-intensity activity such as leisure cycling, (3) walking, and (4) sitting.
5. Primary Outcomes
1) Balance parameters
Balance was assessed using the Biodex Balance System (BBS) SD (12.1-inch [30.7-cm] display, 115 VAC; Biodex Medical Systems Inc., Shirley, NY, USA). The BBS measures stability indices, which represent the variance of foot platform displacement in degrees for motion in different planes. The platform is fixable and movable. The participants stood barefoot and were not permitted to touch the handrails during the tests. The platform was locked, and the participants were asked to control themselves while keeping the indicator in the center of the target on the screen. To eliminate the learning effect, three familiarization test trials, each consisting of 20 seconds, were applied to individuals the day before the first assessment. Three different tests (Limits of Stability [LoS], Athlete Single Leg [ASL], Clinical Test of Sensory Interaction of Balance [CTSIB]) were selected. The test results were interpreted using the software of the device. The stability and sway indices extracted from the BBS have been shown to be reliable measures of postural control and balance [9].
2) Limits of stability
This test assesses dynamic postural control and challenges participants to move and control their center of gravity within their base of support. Participants were asked to shift their weight to move the cursor from the center target to a blinking target and back as quickly and with as little deviation as possible. The same process was repeated for each of the eight targets. Targets on the screen blinked in a random order. The test was repeated three times with 10-second rest in between trials. The test duration and overall scores were recorded. The maximum score for the test was 100. Higher scores indicated better balance and greater control of the participantsŌĆÖ stability.
3) Athlete single leg test
The ASL assesses single-leg dynamic balance. Participants were asked to stand barefoot with their dominant foot centered on the balance platform. In the single-leg stance, sway in the platform causes the participant to move, and the degrees of the motion on the platform are recorded as the participant attempts to balance on the moveable surface. Subjects were instructed to keep the cursor in the middle of the target as they balanced without any support from the upper extremities or non-dominant foot. Participants were allowed to receive simultaneous visual feedback of the balance platformŌĆÖs position and movement by a cursor on a target where the center was the optimal neutral position. Three 20-second dynamic trials were performed, and the average value of three trials was recorded for each participant. Balance ability was measured in units of the stability index (StI). The lower the StI, the better the single-leg dynamic balance.
4) Clinical test of sensory integration of balance
The CTSIB provides information about the ability to stand upright under several sensory conditions: (1) eyes open, firm surface (EO-firm); (2) eyes closed, firm surface (EC-firm); (3) eyes open, foam surface (EO-foam); and (4) eyes closed, foam surface (EC-foam). Each condition lasted 30 seconds, and a 10-second break was given between them. For each of the four conditions, participants were instructed to stand as still as possible for each condition. While performing the tests under foam surface conditions, a foam pad (provided with the Biodex system; Biodex Medical Systems Inc.) was placed on the platform that contained the same markings as the firm surface, allowing the participant to reposition their feet into their previously instructed placement. The sway index (SwI) was recorded for each condition of each trial. Lower SwI scores indicated greater balance.
6. Secondary Outcomes
1) Dorsiflexion range of motion
Ankle dorsiflexion ROM (DFROM) was measured using the weight-bearing lunge test (WBLT). Participants were instructed to stand in front of a wall with the second toe, center of the heel, and knee kept in a plane perpendicular to the wall and keep the heel on the ground during the test. Participants were asked to lunge forward until the knee touched the wall so that maximum dorsiflexion could be obtained. The distance between the second toe and wall was measured. Participants performed three trials for each foot, and the average value was used for statistical analysis.
2) Muscle strength
Dorsiflexor muscle strength was measured using a hand-held dynamometer (Lafayette Hand Held Dynamometer, model 01165; Lafayette Instrument, Lafayette, IN, USA). Participants were asked to sit on a bedside (height=100 cm) with the hip and knee at 90┬░ flexion. All participants warmed up before the test to perform it correctly. They were first shown the movement to be tested and then asked to perform it. After bringing the ankle to dorsiflexion, the dynamometer was placed over the metatarsal heads on the dorsum of the foot. Then, the participants gradually increased their muscle force to a maximum that had to be sustained for 6 seconds against the dynamometer. Three measurements were performed, and the highest score was used for analysis. Two-minute rest was given between measurements.
7. Statistical Analyses
All data were analyzed using the IBM SPSS ver. 20.0 for Windows (IBM Corp., Armonk, NY, USA). Descriptive statistics are presented as frequencies and percentages for categorical variables, while continuous variables are presented as means and standard deviations. The variables were investigated using visual (histograms and probability plots) and analytical methods (Shapiro-Wilk test) to determine if they were normally distributed. The results are reported as baseline, post-intervention, and change (╬ö) values. The distribution of demographic and clinical characteristics between the groups was analyzed using the chisquare test. Since the normality assumption was violated, non-parametric tests were used for statistical analysis. The Mann-Whitney U test and Wilcoxon test were applied for between-group and within-group analyses, respectively. A 5% type-I error level was used to determine statistical significance (P<0.05). The effect size for each non-parametric comparison was calculated as r=Z/ŌłÜN, where Z is the Z score of the comparison and N is the number of total observations.
RESULTS
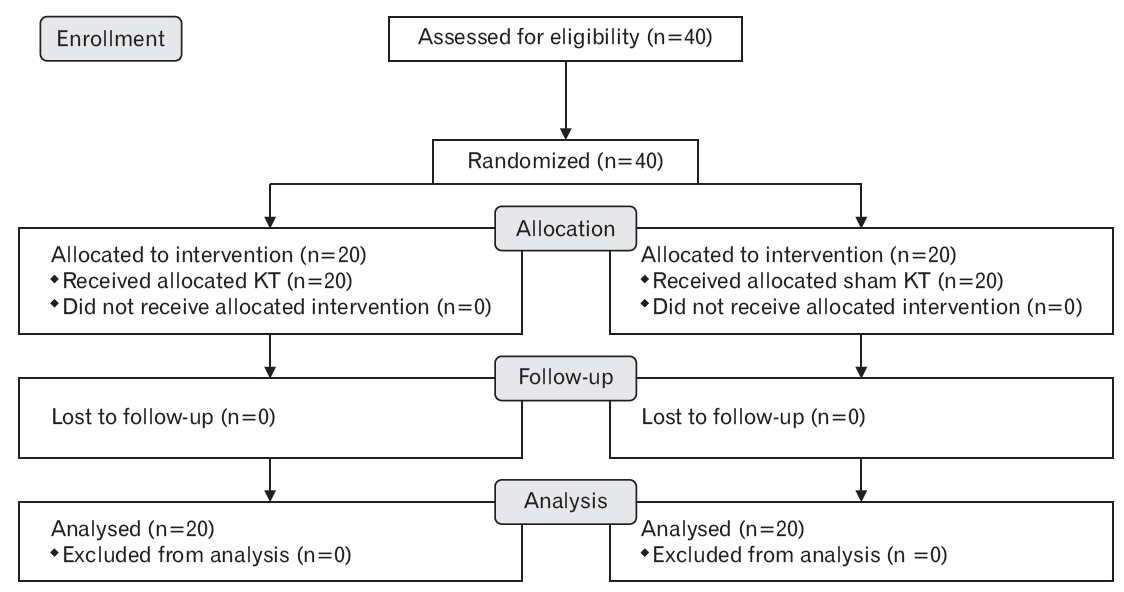
The groups were analyzed for all outcomes (Figure 2), and the analyses were performed by the original assigned groups. Post hoc power analysis with 5% type-I error was performed using effect sizes of the ASL score, revealing 82% power.
There were no statistically significant differences in the distribution of demographic and clinical characteristics between the groups (P>0.05) (Table 1). No significant differences were found between the groups in terms of age, body mass index, and baseline values of the measured variables after the initial assessment (P>0.05) (Table 2).
LoS scores increased significantly in both groups (P<0.05), with a 7.5-point median change in the experimental KT group and a 7.0-point median change in the sham KT group. However, the ASL score showed a significant improvement only in the experimental KT group (P=0.02). SwIs for all four conditions in the CTSIB test, DFROM, and dorsiflexor muscle strength for both ankles did not change in any of the groups after intervention (P>0.05) (Table 3).
Statistical analyses of between-group mean differences showed that there was no superior intervention over the other in improving any of the variables (P>0.05) (Table 3).
DISCUSSION
The results of this study showed that KT could be useful in increasing the single-leg dynamic balance in healthy individuals. However, although both experimental and sham application of KT significantly increased dynamic postural control (LoS), neither caused a significant change in DFROM, muscle strength of ankle dorsiflexors, and sensory interaction of balance. In addition, KT had no superior effect on any of the variables compared to the sham application.
KT influences postural balance by enhancing proprioception due to increased stimulation of sensory receptors, facilitation of muscle contraction, or support of joints without restricting the ROM in patients with stroke and individuals with functional ankle instability [10-12]. In relevant studies, researchers mostly used tendon correction and muscle activation/inhibition techniques of KT. However, this study intended to determine the effects of the KT mechanical correction technique and was conducted only in healthy individuals to reveal the pure effects of KT by comparing a sham application.
Previous studies reported that a single application of KT to the ankle improved balance in people with ankle disorders [2-4]. Rojhani-Shirazi et al. [10] applied KT to the affected ankle in the direction of dorsiflexion and eversion to correct ankle deformities in patients with stroke. They found that KT improved the scores of reach tests, Berg Balance Scale, and center of pressure (COP) in these patients [10]. Mohamed et al. [11] found that KT had a superior effect on dynamic postural control in the Star Excursion Balance Test compared to no tape and athletic tape. Shields et al. [12] applied the lateral ankle sprain technique of KT to college-aged participants and reported that KT did not significantly improve postural control.
According to relevant studies conducted in healthy individuals, the effect of KT on balance appears to be controversial [13,14]. Nakajima and Baldridge [14] applied the tendon correction technique of KT and found that overall dynamic postural control did not improve initially compared to that seen in the placebo group. Parallel to this study, Wilson et al. [13] applied KT to the gastrocnemius to facilitate the muscle and concluded that KT did not improve dynamic single-leg balance evaluated using the ASL test of the BBS compared with a sham application. Although the results of the current study contradict those reported by Wilson et al. [13], they are consistent with those reported by Nakajima Baldridge [14]. However, it should be noted that a comparison of the results of these three studies may not be optimal because different KT techniques were used in each study.
Some studies have investigated the effects of similar mechanical correction techniques using different taping materials [6,15-17]. Most of these had no beneficial effects on dynamic postural control; however, the current study showed that both experimental and sham KT were effective in improving dynamic postural control. These findings suggest that the elastic properties of KT might have been more effective than the desired mechanical effects such that dynamic postural control had also improved in the sham group, in which no tension was applied. The results of this study would be applicable in clinical decisions regarding the use of KT in healthy individuals and athletes when LoS improvement is desired. Due to supported joints and increased stimulation of sensory receptors, KT to the ankle could be effective in improving balance parameters in conditions such as ankle sprains. The results of KT application to the ankle were shown to be controversial in improving balance in athletes and non-athlete individuals with ankle disorders/injuries [10-12,18,19].
Extreme positions such as standing on a single leg on an unstable surface require balance control and dependence on the ankle complex for support. The results showed that single-leg dynamic balance improved only in the experimental KT group; however, dynamic postural control (LoS) improved in both groups. Two different factors may have contributed to this. First, in the LoS test, both feet were in contact with the ground, and the body weight was transferred to the ground through them. Therefore, the total weight was distributed almost equally on both legs. However, in the ASL test, one foot is in contact with the ground, and the whole weight is transferred to the ground through that foot [20]. When more load is placed on one leg, the migration of the fibula in the anteroinferior direction also increases accordingly [21]. The larger migration of the fibula might have caused greater tensile force on the Kinesio tape, thereby increasing stimulation to cutaneous mechanoreceptors and enhancing the mechanical correction effect. Second, while the platform is fixed and the participant leans in eight directions in the LoS test, in the ASL test, the platform is movable and the participant tries to maintain balance on one leg. This may indicate that KT to the ankle may be more effective in improving balance parameters in conditions where the ground is unstable and COP is relatively less displaced. However, further studies are needed to confirm these hypotheses.
The sensory interaction of balance is also crucial in daily physical activities and is usually evaluated by measuring postural sways in altered conditions of surface and visual input, such as firm/foam surface or eyes open/closed [22]. KT did not significantly alter the sensory interaction of balance when applied to healthy individuals. One possible reason could be that the participants in this study were healthy and had no major proprioceptive or vestibular deficits.
Previous studies have shown that KT can be beneficial in increasing ankle ROM [23,24]. Merino-Marban et al. [23] applied the KT muscle technique to calf muscles of athletes with calf pain and showed that ankle DFROM measured using the WBLT increased immediately. Similarly, Eom et al. [24] used the muscle technique for calf muscles in healthy university students and reported a significant increase in both ankle DFROM and plantarflexion ROM. Instead of the muscle technique, the mechanical correction technique of KT was applied to the fibula in the current study, and this KT technique appeared to be ineffective in causing a significant change in DFROM immediately after application.
Some studies have investigated whether KT can alter muscle strength in people with or without ankle disorders. Kristian et al. [25] reported that the KT muscle technique had no effect on improving the muscle strength of both ankle dorsiflexors and plantar flexors in unstable ankles. Similar to this finding, Lee et al. [26] showed that the application of muscle technique kinesiology tape from insertion to origin or origin to insertion did not significantly change plantar flexor muscle strength in healthy individuals. However, it should be noted that the material of the kinesiology tape is different from that of the Kinesio tape. In the present study, neither mechanical correction technique nor sham application of KT altered muscle strength. This result suggests that tactile input generated by mechanical correction was not strong enough to modulate the dorsiflexor muscle strength of healthy individuals because it was not specifically applied along the dorsiflexor muscles.
This study has several strengths. A computer-assisted balance measurement device (BBS) was used to assess balance-related outcomes, which is more sensitive and reliable than other non-computerized methods used in relevant studies. Another distinctive feature is that the effects of the mechanical correction technique of KT were examined on balance and compared to those of a sham application.
The limitations of this study are as follows. The results should not be generalized since only healthy, pain-free individuals were included. In addition, the implications of laboratory or clinical findings on function and performance are essential; therefore, it might have been useful if performance was measured using vertical jump or single hop tests. In this study, the immediate effects of KT were examined in a relatively small sample, and future studies including a larger sample size and long-term follow-ups would more clearly elucidate the effects of ankle KT on balance.
In conclusion, the mechanical correction technique of KT was useful in providing an immediate improvement in the single-leg dynamic balance of healthy individuals. However, it did not significantly change the sensory interaction of balance, DFROM, and muscle strength. Although both experimental and sham KT were effective in improving postural control, no intervention was superior over the other.