Impact of Sleep Duration on Decline in Kidney Function in Adult Patients with Hypertension: A Community-Based Prospective Cohort Study
Article information

Abstract
Background
Sleep duration is associated with various health conditions, including chronic kidney disease. However, the association between sleep duration and decline in kidney function in the South Korean population remains unclear. We aimed to investigate the impact of sleep duration on kidney function decline in adult patients with hypertension.
Methods
This cohort study was performed using data obtained from the Korean Genome and Epidemiology Study; 2,837 patients with hypertension who initially had normal kidney function were included. Glomerular filtration rates (GFRs) were estimated at baseline and throughout the 16 years of follow-up. A person was considered to have a decline in kidney function if they had a GFR <60 mL/min/1.73 m2. Sleep duration data were obtained through interviewer-assisted questionnaires. Sleep durations were classified as short (<6 hours), normal (≥6 hours but <9 hours), and long (≥9 hours). The Cox proportional hazards model was applied, with adjustments for covariates.
Results
After adjusting for covariates, sleep duration was not associated with a decline in kidney function. However, among men with poorly controlled hypertension at baseline, compared to men with normal sleep durations, men with sleep durations <6 hours had a significantly higher risk of kidney function decline (hazard ratio, 1.56; 95% confidence interval, 1.02–2.36).
Conclusion
Short sleep duration did not seem to be associated with an increased risk of decline in kidney function; however, it may be a risk factor for the decline in kidney function in men with poorly controlled hypertension.
INTRODUCTION
Sleep disorders are common worldwide. In one study, the occurrence of insomnia was reported in 17% of a representative sample of the general South Korean population; in another study, the prevalence of insomnia among an elderly population aged between 65 and 84 years living in a city in South Korea was found to be 57.7% [1,2]. Sleep disorders have been proven to be risk factors for the development of medical conditions such as hypertension, diabetes, and chronic kidney disease (CKD) [3-5].
Hypertension is a common disease worldwide, and according to the 2019 Korea National Health and Nutrition Examination Survey, the prevalence of hypertension among people aged >30 years is 32.9% and that among people aged >65 years is 64.4% [6].
CKD is a complication of hypertension defined as glomerular filtration rate (GFR) <60 mL/min/1.73 m2 for more than three months [7]. CKD can decrease quality of life and increase medical expenses [8]. Therefore, risk factors should be identified to prevent the decline in kidney function in adults with hypertension.
Previous research has shown that among adult patients with hypertension, black people and people with underlying kidney disease have an increased risk of CKD [9]. In addition to genetics and comorbidities that are not modifiable, we believe that sleep disorders can affect the progression of CKD. Sleep disorders activate sympathetic nerves that increase blood pressure and cause systemic inflammation, resulting in glomerular endothelial injury and proteinuria [10-15]. However, with respect to the South Korean population, it remains unclear whether sleep disorders are a risk factor for a decline in kidney function in patients with hypertension.
In this study we investigated kidney function decline based on the sleep duration of patients with hypertension who initially had normal kidney function.
METHODS
1. Data Source and Study Population
This prospective cohort study was conducted using data regarding sleep history for the Anseong and Ansan cohorts included in the Korean Genome and Epidemiology Study (KoGES) [16].
Between 2001 and 2002, 10,030 participants were recruited, 5,012 and 5,018 participants were recruited from Ansan, and Anseong, respectively. The participants were followed up 8 times (at 2-year intervals) until 2018. However, in this study, we used data from seven follow-ups.
In this study, a participant was considered to have hypertension if it had been diagnosed by a doctor, or if upon measuring the average blood pressure in the patient’s left and right arms, either the average systolic or diastolic blood pressure was found to be ≥140 mm Hg and ≥90 mm Hg, respectively. Initially, 3,261 participants were included in the study.
Participants who did not answer questions regarding sleep duration, did not have blood creatinine levels measured, and did not provide data regarding their weight or age were excluded from the study. Participants with an estimated GFR (eGFR)<60 mL/min/1.73 m2 , participants who had urinary protein dipstick test values greater than 1+, and participants who had already been diagnosed with CKD were also excluded from the study. A total of 424 participants were excluded, and the remaining 2,837 patients were included (Figure 1).
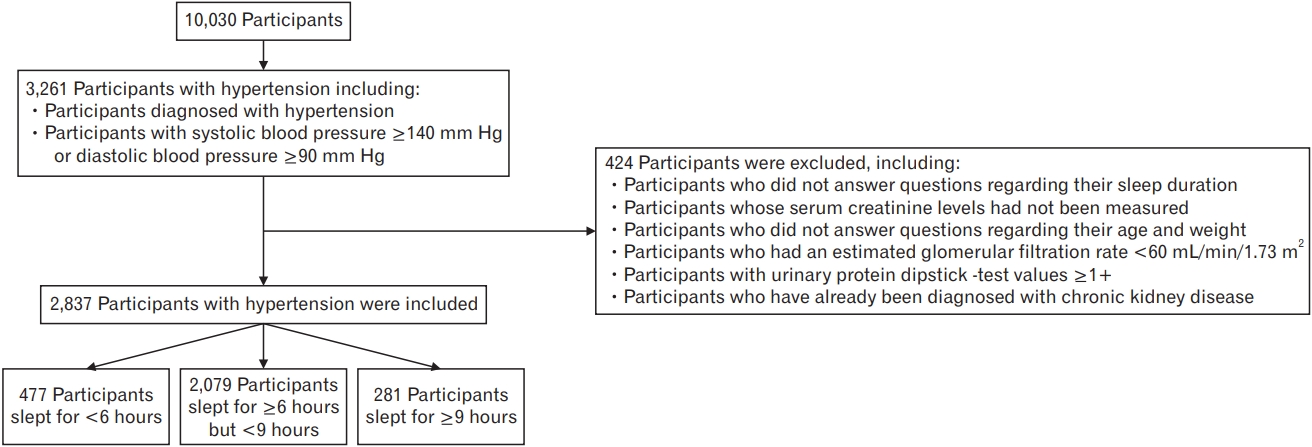
Flowchart depicting the participant-selection process.
An institutional review board (IRB) determined that this study was exempt from ethical approval (IRB no., X-2105/686-903). Informed consent was obtained from all participants included in the study.
2. Outcome Definition
Each patient’s eGFR was calculated using the equation from the Modification of Diet in Renal Disease Study, which is the most commonly used equation for the calculation of eGFR. It was also used in a previous study in which data obtained in the KoGES had been used [17,18].
For female participants, 186×(serum creatinine)-1.154 ×(age)-0.203 was multiplied by 0.742. We calculated age to minimize follow-up loss as follows: age=(follow-up visit date–baseline visit date)/365+baseline age. The outcome was defined as the occurrence of decline in kidney function when a participant’s eGFR fell below 60 mL/min/1.73 m2 for the first time during the follow-up period; if decline in kidney function occurred in a patient, follow-up was terminated for that patient.
3. Evaluation of Sleep Duration
A trained interviewer asked the participants about the number of hours they usually slept daily; in response, the participants stated only their sleep hours. Participants were divided into three groups based on their sleep duration. The average sleep duration for Koreans is 6.8 hours on weekdays and 7.5 hours on weekends, and the recommended sleep duration is known to be 6–8 hours [6,19]. Participants who slept for <6 hours were included in the short sleep duration group; ≥6 hours but <9 hours were included in the normal sleep duration group; ≥9 hours were included in the long sleep duration group.
4. Covariates
Covariates included age, sex, systolic and diastolic blood pressure, eGFR, diabetes, dyslipidemia, cancer history, body mass index (BMI), smoking (never, former, current), alcohol consumption status (never, former, current), duration of daily moderate physical activity (0 minute, <30 minutes, ≥30 minutes), snoring, and Epworth Sleepiness Scale (ESS) score.
Data regarding demographic characteristics, sleep history, underlying diseases, smoking, alcohol, physical activity, snoring, and ESS score were obtained through a trained interviewer-assisted questionnaire. Each participant’s blood pressure was measured by an interviewer using a mercury sphygmomanometer. Blood pressure was measured at least twice for each participant after a rest period of at least 5 minutes. The next measurement was taken after at least 1 minute had passed. If the two blood pressure values differed by more than 5 mm Hg, more measurements were taken until the two values were similar. The mean of the last two measurements was calculated. Each participant’s BMI (weight in kilograms [kg] divided by the square of height in meters [m]) was calculated. Blood samples were collected in serum separator tubes and two ethylenediaminetetraacetic acid tubes.
5. Statistical Analysis
All statistical analyses were performed using Stata ver. 16.0 (Stata Corp., College Station, TX, USA). Categorical variables were analyzed using the chi-square test, and analysis of variance was used to analyze mean and standard deviation (SD) values of continuous variables. Statistical significance was set at P<0.05.
Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using a Cox proportional hazards model. The reference group was the normal sleep duration group of participants who slept for ≥6 hours but <9 hours. Two models were created to adjust for covariates, which we named model 1 (adjusting for age, sex, baseline eGFR, and baseline systolic and diastolic blood pressure that were thought to have profound effects on kidney function) and model 2 (additional adjustment for diabetes, dyslipidemia, cancer-history, BMI, smoking, alcohol consumption, physical activity duration, snoring, and ESS score). We chose model 2 as our main model because it was adjusted for all covariates that could affect kidney function.
RESULTS
1. Baseline Characteristics
Of the 2,837 participants, 477, 2,079, and 281 were included in the short, normal, and long sleep duration groups, respectively. The mean±SD sleep durations of the participants in the short, normal, and long sleep duration groups were 4.6±0.7 hours, 7.0±0.8 hours, and 9.4±0.7 hours, respectively.
The mean±SD baseline eGFR of the participants in the short, normal, and long sleep duration groups were 93.8±20.0 mL/min/1.73 m2 , 95.0±20.3 mL/min/1.73 m2 , and 96.1±19.01 mL/min/1.73 m2 , respectively; in this regard, there were no significant differences among the three groups. The additional baseline characteristics of the participants are shown in Table 1.

Baseline characteristics of participants according to sleep duration
2. Incidence of Decline in Kidney Funtion
During the 16-year period, 307 of the 2,837 participants had never been followed up, and those lost to follow-up were right-censored. The mean±SD follow-up period was 9.17±5.34 years, with 26,015 person-years of follow-up. Of the 2,530 participants who had been followed up, 642 (25.3%) developed decline in kidney function, and the incidence rates in the short sleep, normal sleep, and long sleep duration groups were 27.0 (per 1,000 person-years), 23.3 (per 1,000 person-years), and 31.8 (per 1,000 person-years), respectively.
Compared to the participants in the reference group, the participants in the short sleep and long sleep duration groups had HRs of 1.18 (95% CI, 0.96–1.45) and 1.34 (95% CI, 1.05–1.70), respectively. However, after using models 1 and 2 to adjust for covariates, long sleep duration was not found to be associated with an increased risk of kidney function decline.
When analyses were stratified by sex, the men in the short sleep duration group had an HR of 1.74 (95% CI, 1.25–2.41) in the crude model and an HR of 1.52 (95% CI, 1.08–2.14) in model 1, which was significant when compared to the men in the reference group. However, with respect to model 2, the short sleep duration group had an HR of 1.37 (95% CI, 0.95–1.97). The women who slept for ≥9 hours had an HR of 1.36 (95% CI, 1.03–1.78); however, this ratio was not significant after adjusting for covariates (Table 2).
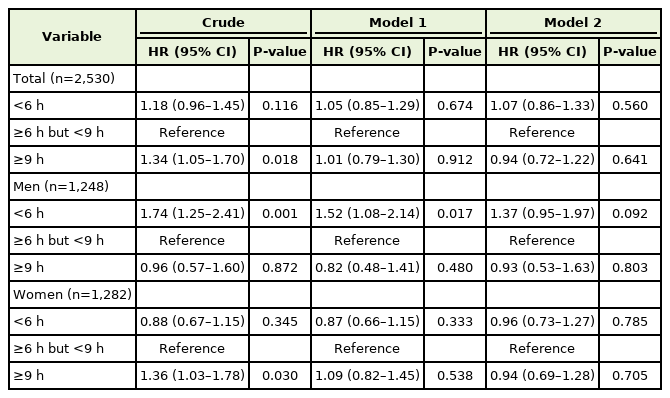
Hazard ratios for the decline in kidney function according to sleep duration in adult patients with hypertension
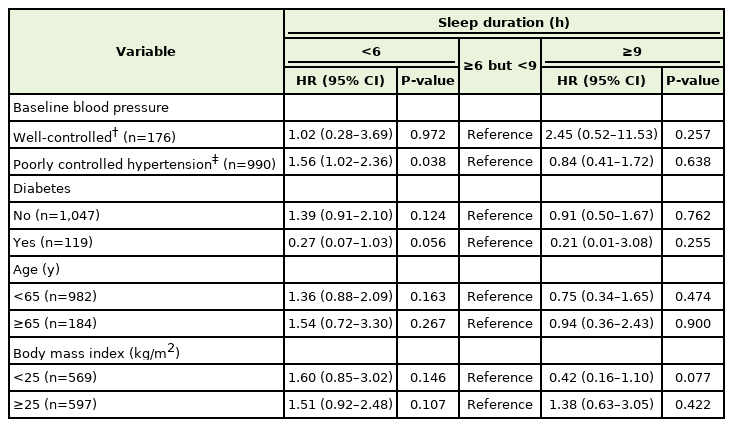
Using model 2, we conducted a subgroup analysis of the male and female participants. Among the male participants who had poorly controlled hypertension (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg) at baseline, men who slept for <6 hours had an increased risk of decline in kidney function (HR, 1.56; 95% CI, 1.02–2.36) when compared to men with normal sleep durations (Table 3). However, a subgroup analysis of the female participants revealed that there was no significant association between the kidney function decline and sleep duration (Table 4).

DISCUSSION
In this study, we found that among a population of South Korean individuals with hypertension, short or long sleep durations did not seem to increase the risk of decline in kidney function. However, we found that male participants with hypertension who slept for short durations had a high risk of kidney function decline, especially when the initial control of hypertension in such patients was poor.
Several studies on the association between sleep duration and CKD have been conducted. In a cohort study conducted in Taiwan, compared to participants who slept for 6–8 hours, those who slept less than 6 hours and more than 8 hours were found to have an increased risk of CKD. When a subgroup analysis of patients with hypertension was conducted, only those who slept for >8 hours had an increased risk of developing CKD. However, when a subgroup analysis of patients with diabetes was conducted, there was no significant difference between the three groups [4]. In a Japanese prospective cohort study, it was found that the risk of progression of CKD to end-stage renal disease in patients with short or long sleep durations was significantly greater than that in patients with normal sleep durations [20].
In a previous cross-sectional study in which data obtained in the KoGES were used, sleep duration was found to be associated with CKD only among female participants with long sleep durations [18]. In another study conducted in Korea, sleep duration was found to be associated with CKD in both female and male participants with long sleep durations [21].
In a Japanese retrospective cohort study, compared to participants with normal sleep duration, men with short sleep duration were found to have a decreased risk of CKD. The authors of this study suggested that the average sleep duration of Japanese people is shorter than that of other ethnic groups, and this difference in average sleep duration could have resulted in inconsistency between the findings of this study and those of other studies [22]. In this study, only male patients with poorly controlled hypertension in the short sleep duration group had a high risk of decline in kidney function. We believe that Korean male insomnia patients had more social stress factors than women, causing more sympathetic nerve activation and inflammatory reactions. The reason the results were significant when participants’ blood pressure control was poor is that there was no protective effect of antihypertensive medicine.
To the best of our knowledge, our study is the first Korean cohort study to investigate the association between sleep duration and the decline in kidney function in patients with hypertension. However, this study had some limitations. First, we did not investigate whether there is an association between sleep quality and CKD incidence. Second, in this study, sleep duration was analyzed through the administration of a questionnaire rather than objective analysis or measurements. However, objective measurements are not cost-effective in epidemiological studies, and a previous study showed that sleep durations determined using a questionnaire were similar to those objectively measured [23]. Third, we considered only baseline sleep duration and failed to analyze sleep duration changes over time. However, sleep disorders are chronic diseases, and participants in the short or long sleep duration groups are likely to have sleep disorders later. Fourth, the study population was not representative of the general South Korean population because only individuals from Ansan and Anseong were considered. Despite these limitations, in this study, we attempted to investigate whether there was an association between sleep duration and the decline in kidney function in patients with hypertension. To overcome the limitations of this study, subsequent research should be performed.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.