INTRODUCTION
Age-related changes of body composition are well-documented with increases in fat mass and decreases in muscle mass.1-3) Sarcopenia, the age-related decrease in muscle mass, negatively impacts health as it leads to reduced mobility and functional disability.3) In addition, postmenopausal women experience hormone changes that are associated with an accumulation of central body fat, leading to the development of insulin resistance and the metabolic syndrome.4,5)
Recently, sarcopenia and obesity in the elderly due to the increase of average life expectancy, and the westernization of diet and lifestyle have become a prominent health concern. Especially, as postmenopausal obesity increases, many tools such as exercise machines and dietary supplements are being used without medical evidence of their benefit. One of these tools, whole body vibration (WBV), operates by conferring a continuous vibration stimulus to the whole body and is widely-used in sports centers.
Hip and lumbar-spine bone mineral density can improve significantly after WBV in postmenopausal women.6,7) Furthermore, WBV exercise can increase muscle mass in older women.8,9) Other studies about the beneficial effects of WBV reported that WBV exercise increases muscle strength8,10-13) and improve balance.14) These studies have clearly indicated that WBV can affect body composition. In animal studies, WBV suppressed adipogenesis in young adult mice15) and reduced fat accumulation in rats.16) Verschueren et al.13) found that WBV and resistance training can be altered by decreasing fat mass, but training did not significantly change lean body mass.
Yoo et al.17) reported WBV exercise in young Korean adults has no effect on reducing body weight and fat mass, and on increasing muscle mass. Little is known of the effects of WBV on body composition in Korean postmenopausal women. Therefore, the aim of this pilot study was to evaluate the effects of WBV on body composition in Korean postmenopausal healthy obese women.
METHODS
1. Study Design and Subjects
We performed a pilot study for an 8-week intervention trial to evaluate the effect of WBV on the changes of body weight, waist circumference, body composition including muscle mass, fat mass, and some metabolic markers in postmenopausal healthy obese women. All subjects provided with informed consent before they were enrolled. Thirty postmenopausal women aged over 50 years working in one university hospital in Suwon, Korea, were recruited voluntarily using an advertisement posted from March to October, 2010. Exclusion criteria were an age Ōēż 50 years; and a body mass index (BMI) < 25 kg/m2; diagnosis of diabetes, hypertension, cardiovascular disease such as angina pectoris, myocardial infarction, or history of cerebrovascular diseases; history of female hormone replacement therapy, osteoporosis, knee osteoarthritis, and any muscle disease who could not endure the WBV. Fifteen subjects dropped out due to various personal issues. The remaining 15 subjects completed the entire 8 weeks of this study and the data before and after WBV were compared.
2. WBV Intervention
All subjects exercised for 8 weeks on a vibration platform (Body master EOS-6600; MEDIEOS, Gwangju, Korea). WBV exercise was performed for 10 minutes twice per week in the Health Promotion Center of our institution. All training sessions were performed between 12:00 and 13:00 hours. Each exercise was performed in the upright position and was observed by a trained research nurse. The training intensity was low amplitude (2 mm) and low frequency (22 Hz) of vibration.
During exercise, no overall adverse reactions or side effects were reported. But, one healthy subject without any disease ceased exercise due to mild knee pain. All other subjects concluded the exercise program without side effects or adverse reactions. In addition, all subjects were requested not to change their dietary intake, lifestyle behaviors such as daily activity, exercise, an usual sleep at night during the study.
3. Anthropometric and Laboratory Measurements
All subjects completed a self-administered questionnaire to assess past history and social history. History included hypertension, diabetes, drinking alcohol, smoking, and other such factors. The height and body weight of the participants were measured while they wore light clothing without shoes. Weight was measured to the nearest 0.1 kg, and height was measured to the nearest centimeter. BMI was calculated as the weight divided by height squared (kg/m2). Trained nurses measured the waist circumference (WC) between the lower rib and the iliac crest and electrically measured blood pressure after the participants had been at rest for at least 15 minutes using a model TM-2655P apparatus (PMS Instruments, Tokyo, Japan). The body composition of each participant was analyzed using the Body Impedance Analysis, InBody 720 (Biospace, Seoul, Korea). Additionally, all of the subjects underwent automated blood testing using a TBA-200FR apparatus (Toshiba, Tokyo, Japan); measurements included standard enzymatic measurements of total cholesterol, high-density lipoprotein cholesterol, triglycerides, and fasting glucose in fresh serum samples. All tests were done before intervention and were repeated after 8 weeks intervention.
4. Statistical Analyses
The data are presented as mean ┬▒ standard deviation (SD). All measures were normally distributed, as determined by the Kolmogorov-Smirnov test. Paired t-test was used to compare the changed of pre- vs. post-intervention. Pearson correlation was used to calculate the correlation coefficient between skeletal muscle mass change and the change of other variables. Also we used linear regression analyses to assess the relationship between skeletal muscle mass change and significantly related weight change, percent (%) body fat change, white blood cell count change and low-density lipoprotein cholesterol change. Statistical calculation was performed using the SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA). All significant P-values were < 0.05.
RESULTS
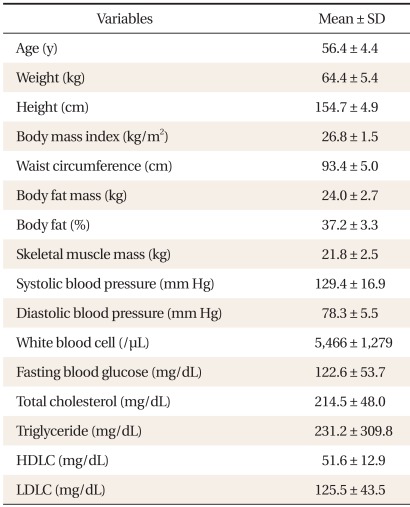
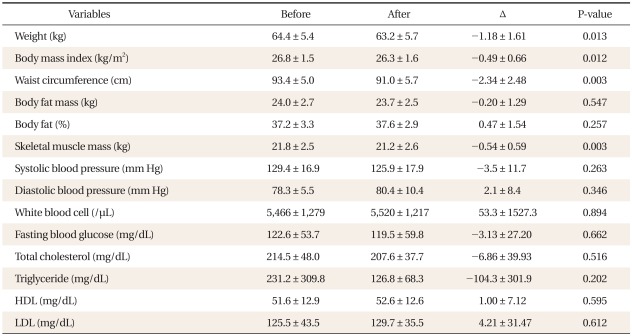
Baseline characteristics of the study subjects are shown in Table 1. Mean age, body weight, BMI, and WC were 56.4-years-of-age, 64.4 kg, 26.8 kg/m2, and 93.4 cm, respectively. After WBV exercise, the changes of mean body weight (Δweight, -1.18 ± 1.61 kg; P = 0.013), BMI (ΔBMI = -0.49 ± 0.66, P = 0.012), and WC (ΔWC, -2.34 ± 2.48 cm; P = 0.003) were significantly decreased. Unfortunately, muscle mass also significantly decreased (Δmuscle mass, -0.54 ± 0.59 kg; P = 0.003). Other body composition index and laboratory markers were not significantly changed after exercise (Table 2).
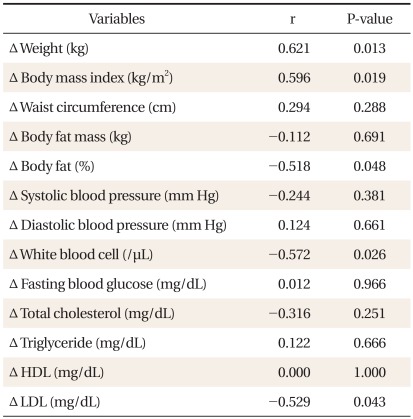
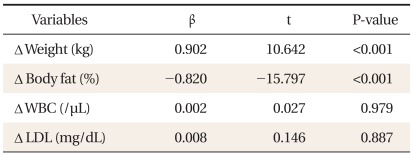
We also evaluated the relationship between the change of muscle mass and other body composition, as well as laboratory markers by the Pearson correlation method. The change of muscle mass positive correlated with weight (r = 0.621, P = 0.013) and BMI (r = 0.596, P = 0.019), and negatively correlated with % body fat (r = -0.518, P = 0.048) (Table 3). Using the significant values in correlation method, we examined the linear relationship between the muscle mass change and other values. The changes of muscle mass showed a significant linear relationship with body weight change positively and body fat % change negatively (Table 4).
DISCUSSION
In this 8-week pilot study, we demonstrate that WBV exercise had a weak but positive effect on WC and body weight reduction in postmenopausal women. Concerning body weight reduction, the present data indicate a possibility of the reduction of muscle mass after WBV exercise in this short duration pilot study.
Many studies have focused on WBV exercise. Machado et al.8) reported that WBV exercise increase muscle mass in older women. Verschueren et al.13) found that WBV and resistance training were altered by decreasing fat mass, but both training did not significantly change lean body mass. Von Stengel et al.18) reported in a study that used a training and training with vibration group that both approaches favorably affected lean body mass, total body fat, and abdominal fat, but that no additive effects were generated by the vibration stimulus. In addition, no significant changes were determined for body weight, but there was a tendency toward a gain in the control group. Compared with our study, the WBV group did not solely employ WBV exercise, but also engaged in aerobic dance and functional strength training. Similar to that results, Fjeldstad et al.19) reported that vibration plus resistance training produced significant increases in total bone free lean tissue mass, and significant decreases in total % body fat. But, body weight did not differ significantly from the control group. This was not solely due to the vibration effect, because the training group was vibration plus resistance training. Vissers et al.20) reported intervention groups including diet plus WBV group displayed significantly decreased weight. Furthermore, visceral adipose tissue changed most in the diet plus vibration group compared to the control group and other intervention groups including a diet only group and fitness only group. However, previous studies evaluating only WBV exercise have been rare.
In a previous Korean study, Yoo et al.17) reported WBV exercise had no significant effect on reducing body weight and fat mass, visceral fat area, and on increasing muscle mass. But, these results were in young adults. There have been no previous studies about WBV effects on body composition in older patients. Because of the rarity of studies, our study is meaningful in its assessment of only WBV effects on body composition in postmenopausal women.
Compared to the previous studies, our study has shown that WBV exercise can produce small but significantly decreases of body weight and WC. Especially, WC reduction was evident. As for central obesity, WC reduction may be a good indicator of improved health benefits.21-23) In other words, a short duration of this WBV exercise can be a good modality of reduction of WC in centrally obese postmenopausal women. Unfortunately, however, we also noticed muscle mass decrease in parallel with the body weight reduction. This can be a weak point of WBV exercise. Why this pattern of muscle mass decrease was shown? Actually, we are not sure, but we educated all study subjects not to perform other types of exercise including resistance exercise or any other aerobic exercise with the exception of WBV, the body weight reduction might be partially due to the muscle mass decrease. Nonetheless, we may guess this study subjects would not change their daily life style, though we didn't measure accurately, because their daily hospital jobs were composed of routine works and all the subjects were post-menopausal women, who can hardly change their eating and exercise (Most subjects mentioned that they did not change their daily activity, exercise and eating pattern). However, we cannot conclude these changes are resulted from the effect of WBV due to the several limitations such as small study subjects, lack of control group. Therefore, we should have a careful assess the effect of this short duration intervention but, it may be reasonable to consider a combination exercise regimen including resistance exercise, so as not to waste muscle mass in the WBV exercise.
Our study has several limitations. The first is the small sample size and short intervention duration and frequency. This small sample size gave us several limitations such as no control group with random allocation, so we did not compare the intervention with a control group. In addition, we didn't apply different vibration modality to study subjects due to small sample size. The second is that subjects were working in a hospital located in Suwon, Korea, so these subjects would not represent the total population. The third is that the exact evaluation and control about diet and physical activity was not done, although we recommended that their life style not change. This study subjects were a hospital staff with contraction, which also gave a marked limitation to record dietary habit and physical activity and other lifestyle due to their busy schedules and relative lack of responsibility for those records. Therefore, these effects of WBV on body composition changes were not differentiate from the usual visit. The fourth is that exercise posture during WBV may be relatively difficult for postmenopausal women. In previous studies, WBV training sessions were lead by a physiotherapist. Their sessions typically included squatting, deep squatting, calf raises, lunges, curl-ups, and push-ups, as some examples. But our study was not conducted by a physiotherapist and study subjects might have adopted an insufficient posture. In addition, we did not acquire information concerning total caloric intake, even though we educated subjects to intake the usual calories.
Despite these limitations, this study is the first report that WBV exercise has a positive effect on the reduction of WC in Korean postmenopausal healthy obese women. This finding is meaningful because the previous Korean study for the WBV exercise did not show a positive effect and did not include postmenopausal women, although the prevalence of obesity in this age group was high. However, the WBV exercise without any resistance exercise or other beneficial nutritional supplement to maintain muscle mass can result in the decrease of muscle mass.
In conclusion, in this small pilot study, WBV exercise may help in the reduction of body weight and WC in postmenopausal healthy women. However, attention should be paid not to decrease muscle mass with the inclusion of proper resistance exercise and nutrition in postmenopausal healthy obese women. Further study to evaluate the effect of WBV on body composition will be needed in near future.