INTRODUCTION
The mortality rate of Korean adults over the age of 20 is 31.2 per 100,000 according to Statistics Korea, 2010.1) This is double the mortality rate in Organization for Economic Cooperation and Development nations and 2.4 times the figure ten years previously.2) Actual suicide can generally be predicted from the wish to die, suicidal ideations and previous suicide attempts. Understanding the risks posed by suicide-related behavior is therefore important in preventing suicide.3) A history of psychiatric disorders4,5) and particular demographic characteristics (female, young age, unemployment, and single status) have been presumed to be risk factors for suicide completion and suicide-related outcomes.6)
Smoking is one of many factors that influence suicide and suicide attempts.7) Several studies have found a positive association between smoking and suicide attempts8-10) and others have found an association between smoking and suicide completion.11,12) However, it is not clear whether the relationship between smoking and suicide attempts is causal or correlational.7)
Smoking is positively related to almost all psychiatric disorders13,14) and psychiatric diseases are well-known risk factors for suicide attempts and suicidal ideations.15) However, some analyses of the relationship between smoking and suicidal behavior have not taken into account the effect of mental disorders;16,17) in studies that included controls for psychiatric disorders, the relationship between suicidal behavior and smoking was not significant.18-20) Moreover, many of these studies involved only teenagers; there are few studies of the adult population. In this study, we sought to examine the relationship between smoking status and suicidal behavior (suicidal ideations and suicide attempts) in the Korean adult population.
METHODS
1. Study Population
Data for the study population came from the 4th Korea National Health and Nutrition Examination Survey (KNHANES). The survey contained data on 31,705 individuals, and we approached 24,871 of these to take part in our survey. We excluded people who did not respond to our approach (1,290 people), people who answered "I don't know" to the question about whether they wished to die (51 people), and everyone under the age of 18 (6,465 people). After these exclusions, 17,065 subjects were included in the study, which was approved by the ethics committee of a university hospital in Seoul.
The Ministry of Health and Welfare of Korea set up the KNHANES to examine the general health and nutritional status of Koreans. The 4th KNHANES was conducted from July 2007 to December 2009. It used a stratified multistage sampling design for the South Korean population in multiple geographic areas, of multiple ages and both genders. Weighting the samples could therefore give a meaningful representation of the entire population.
2. Data Collection
Suicidal ideations were assessed by asking the question: "Have you wished to die at any time during the past year?" For those who answered "yes", a further question was asked: "During the past year, have you actually attempted suicide?" From the answers to the first question, we divided people into two groups: 'suicidal ideations' and 'no suicidal ideations'. From the answer to the second question, the 'suicidal ideations' group was further divided into: suicidal ideations without suicide attempts and suicidal ideations with suicide attempts.
We compared various characteristics (age, sex, height, weight, body mass index, total cholesterol, triglyceride, hemoglobin, quality of life measured by visual analog scale of Euroqol 5 dimension,21) alcohol intake, education level, and total pack years) of the 'suicidal ideations' group with those of the 'no suicidal ideations' group. We then compared the characteristics of the 'suicidal ideations' group with those of its two sub-groups.
Household income and education level were classified into four groups, alcohol intake was presented by frequency of drinking days a week (none, ≤1, 2-3, and ≥4), and we used self-reporting to categorize the smokers into three groups: current smokers, former smokers, and non-smokers. Former smoker was defined as someone who selected the question "I do not smoke now. But I smoked in the past." Stress perception levels were divided into "much" and "little" by self-reporting. Depressive mood for more than two weeks and psychiatric counseling during the past year were also assessed by self-reporting. Comorbid chronic diseases were classified into cardiovascular diseases (hypertension, hyperlipidemia, cerebro vascular accident, myocardial infarction, and angina pectoris), musculoskeletal diseases (arthritis and rheumatoid arthritis), respiratory diseases (tuberculosis, asthma, and chronic obstructive pulmonary disease), endocrine diseases (diabetes mellitus and thyroid disease), and gastrointestinal diseases (peptic ulcer, liver cirrhosis, hepatitis type B, and hepatitis type C) by lifetime prevalence.
3. Statistical Analysis
The analysis used weighted values of the stratified samples from the KNHANES. The characteristics of the study subjects were compared using a Student t-test. Household income, education, stress perception, depressive mood for more than two weeks, psychological counseling, comorbid diseases, suicide attempts, suicidal ideations, and smoking status were compared using Pearson's chi-square test. Student t-test and the chi-square test were used to compare variables between groups. Adjusted odds ratio (OR) and 95% confidence intervals (CIs) were calculated by multiple logistic regression analysis to assess the relationship between suicidal ideations and smoking status in all the study subjects, as well as to evaluate the relationship between suicide attempts and smoking status in the 'suicidal ideations' group. A P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Baseline Characteristics of Study Subjects
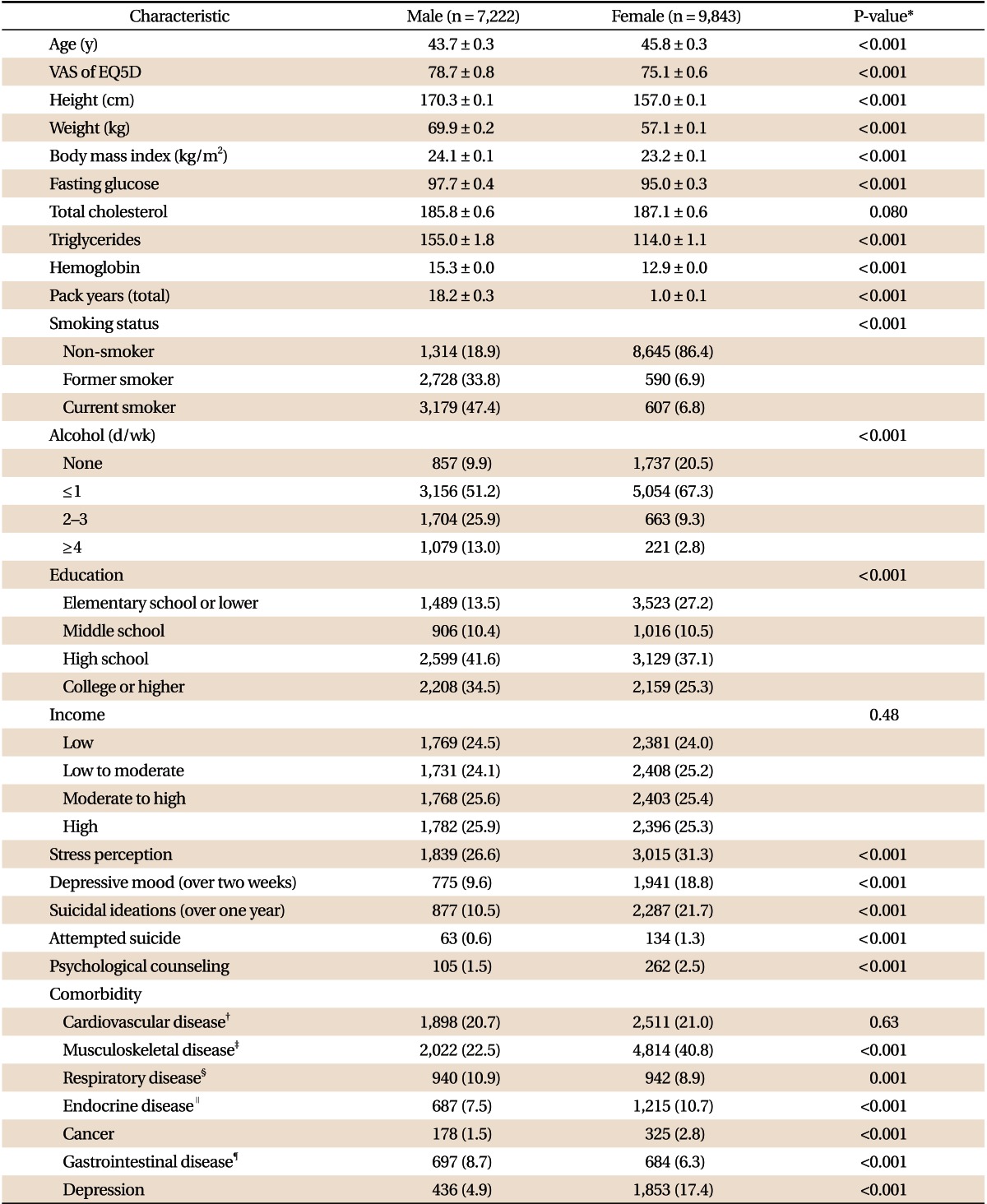
Table 1 shows the descriptive statistics of all the study subjects, by gender. A total of 17,065 subjects (weighted 37,170,000) were included; mean age was 43.7 years for men and 45.8 years for women. Of the men in the study, 18.9% were non-smokers, 33.8% were former smokers, and 47.4% were current smokers. The respective figures for the women were 86.4%, 6.9%, and 6.8%. The total number of pack years was 18.2 for men and 1.0 for women.
Ten point five percent of men and 21.7% of women answered "yes" to the question "Have you wished to die at any time during the past year?" Zero point six percent of men and 1.3% of women answered "yes" to the question "During the past year, have you actually attempted suicide?" Suicidal ideations and suicide attempts were therefore both twice as high in women as in men. Depression, which is a high risk factor for suicide and suicidal behavior, occurred in 4.9% of men and 17.4% of women.
2. Comparison of Characteristics between the Suicidal Ideations Group and Other Groups in Female Subjects
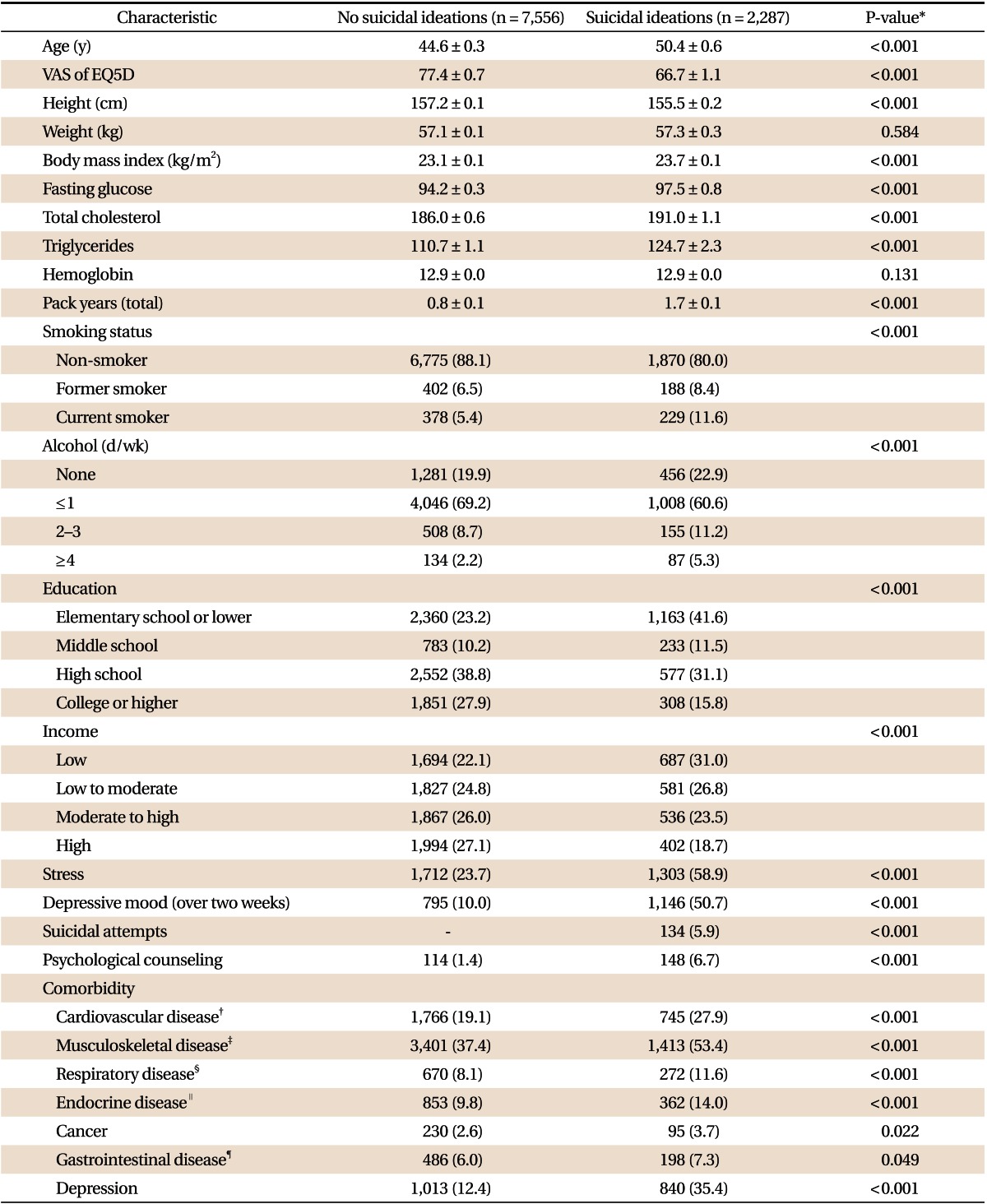
The mean age was 50.4 years in the 'suicidal ideations' group and 44.6 years in the 'no suicidal ideations' group. In the 'suicidal ideations' group, 80.0% were non-smokers, 8.4% were former smokers, and 11.6% were current smokers; in the 'no suicidal ideations' group, 88.1% were non-smokers, 6.5% were former smokers and 5.4% were current smokers. In the 'suicidal ideations' group, 35.4% had experienced depression compared with 12.4% in the 'no suicidal ideations' group. Of those with suicidal ideations, 5.9% had attempted suicide (Table 2).
3. Comparison of Characteristics between the Suicidal Ideations Group and Other Groups in Male Subjects
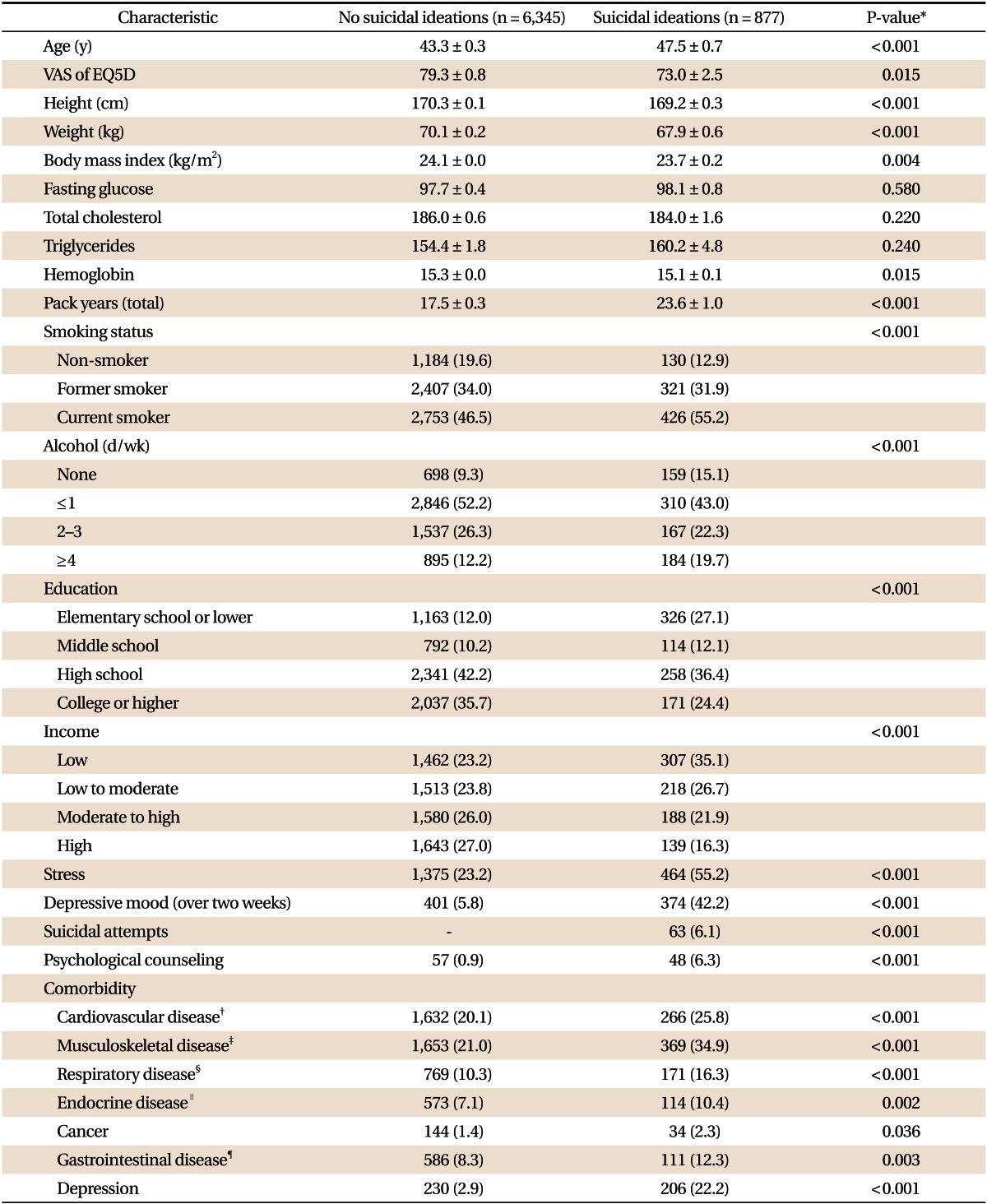
The mean age was 47.5 years in the 'suicidal ideations' group and 43.3 years in the 'no suicidal ideations' group. In the 'suicidal ideations' group, 12.9% were non-smokers, 31.9% were former smokers, and 55.2% were current smokers; in the 'no suicidal ideations' group, 19.6% were non-smokers, 34.0% were former smokers and 46.5% were current smokers. In the 'suicidal ideations' group, 22.2% had experienced depression compared with 2.9% in the 'no suicidal ideations' group. Of those with suicidal ideations, 6.1% had attempted suicide (Table 3).
4. Comparison between People Who Attempted Suicide and Those with Suicidal Ideations in Female Subjects
The mean age of people who had attempted suicide was 48.6 years and the mean age of those with suicidal ideations but who had not attempted suicide was 50.3 years. In the 'suicide attempt' group, 62.7% were non-smokers, 11.4% were former smokers and 25.9% were current smokers. In the group who had not attempted suicide these figures were 81.0%, 8.2%, 10.8%, respectively. Comorbid depressive disorder was more prevalent in the suicide attempt group (53.5%) than in those who had suicidal ideations but had not attempted suicide (34.4%), and this difference was statistically significant (Table 4).
5. Comparison between People Who Attempted Suicide and Those with Suicidal Ideations in Male Subjects
The mean age of people who had attempted suicide was 50.1 years and the mean age of those with suicidal ideations but who had not attempted suicide was 47.3 years. In the 'suicide attempt' group, 13.8% were non-smokers, 29.9% were former smokers and 56.3% were current smokers. In the group who had not attempted suicide these figures were 12.8%, 31.8%, and 55.4%, respectively. Comorbid depressive disorder was more prevalent in the suicide attempt group (48.1%) than in those who had suicidal ideations but had not attempted suicide (20.3%), and this difference was statistically significant (Table 5).
6. Relationship between Suicidal Ideations and Smoking Status in All Study Subjects
After adjusting for other covariates among all the study subjects, current smokers (OR, 1.66; 95% CI, 1.34 to 2.05) and former smokers (OR, 1.39; 95% CI, 1.13 to 1.72) were found to be more prone to have suicidal ideations than the non-smoking group. Similar results were seen for women: current smokers (OR, 2.00; 95% CI, 1.47 to 2.72) and former smokers (OR, 1.48; 95% CI, 1.11 to 1.99) were more likely to have suicidal ideations than non-smokers. However, for men, there was no significant connection between smoking status and having suicidal ideations (Table 6).
7. Relationship between Suicide Attempts and Smoking Status among People with Suicidal Ideations
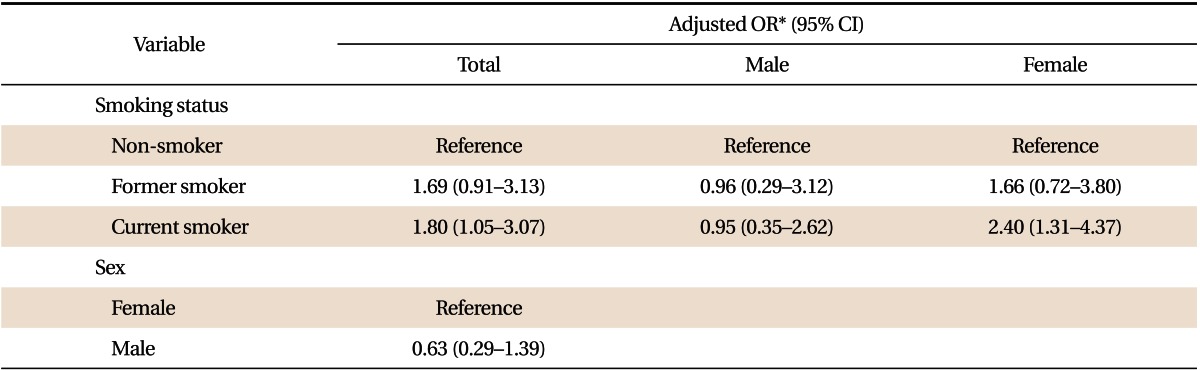
Among people with suicidal ideations, for the study subjects overall (OR, 1.80; 95% CI, 1.05 to 3.07) and for the women alone (OR, 2.40; 95% CI, 1.31 to 4.37), there was a significant relationship between current smoking and suicide attempts. However, for men, there was no significant connection between smoking status and suicide attempts (Table 7).
DISCUSSION
In this study, smoking status was significantly related to suicidal ideations and suicide attempts in the general population, especially in women, independent of comorbid chronic disease and depression. Current smokers and former smokers were more likely to have suicidal ideations than non-smokers, and current smoking was related not only to suicidal ideations but also to suicide attempts.
Our findings are consistent with the theory that nicotine has a biological effect that predisposes people to suicidal behavior,22) based on studies of serotonin and monoamine oxidase (MAO) enzyme activity. Chronic nicotine use lowers serotonin levels23) and MAO enzyme activity,24) and low serotonin levels and low MAO activity are associated with suicidal behavior.25)
A link between smoking and suicidal ideations has also been observed in other studies,26,27) in which current and former smokers were found to be prone to suicidal ideations. However, those studies did not analyze the results by gender. The relationship between smoking and suicidal behavior depends on gender: in men, neither suicidal ideations nor suicide attempts were significantly related to smoking status, but in women, there was a significant relationship between current smoking and both suicidal ideations and suicide attempts; and former smoking in women was related to suicidal ideation. A study by Han et al.10) showed a significant relationship between smoking and suicidal behavior in both men and women. Although that study involved adolescents only, it again found a stronger relationship between smoking and suicidal behavior in women than in men.
Differences in the relationship between smoking and suicidal behavior by gender may be related to differences in the prevalence of smoking and smoking behavior in the population. The majority of men (81.2%) were current and former smokers, whereas the majority of women (86.4%) were non-smokers. However, there might be confounding variables among men that render their results not statistically significant. Some workers have described gender differences in smoking behavior: Marqueta et al.28) reported that the factors contributing to stopping smoking differed by gender, and Anda et al.29) reported that women had less success in stopping smoking than men.
Some studies that analyzed interactions between smoking and brain gamma-aminobutyric acid levels30) support the idea that smoking-related behavior depends not only on social effects but also on biological effects such as gender. However, there have been few studies of the biological relationship between smoking and suicidal behavior by gender; further studies are needed.
In many studies that controlled for psychiatric comorbidity, the relationship between smoking and suicidal behavior was not significant. The 4th KNHANES did not obtain information about any comorbid mental disorders apart from depression, which may be a limitation of our study. In some groups (the group as a whole, and the group of women only) we found a significant relationship between smoking status and suicidal behavior, even after controlling for depression and comorbid chronic physical disease. Hence smokers who have shown suicidal behavior may be regarded as a high-risk group, with respect to suicide attempts and, ultimately, suicide completion. This emphasizes the need for careful observation and follow-up to prevent suicide.
However, the main limitation of this study was the cross-sectional design, so that only associations rather than causal relationships between smoking and suicidal behavior can be inferred. Also, we did not adjust marriage status, job, religion, or life events which could influence suicidal behavior. Further investigations involving quantitative analysis of smoking and suicidal behavior and long-term follow-up are warranted.