INTRODUCTION
Referred or secondary otalgia is a challenging symptom, with the burden on the physician to identify the source. It occurs in up to 50% of adult patients who consult a general physician for otalgia1) and because of the nature of the ear's sensory innervations, a wide variety of disorders can produce referred otalgia. The ear receives an extensive sensory innervation via four cranial nerves (V, VII, IX, and X) and two spinal segments (C2 and C3).2) The most common causes are temporomandibular joint syndrome, pharyngitis, dental disease, and cervical spine arthritis.3) The severity of the pain is not indicative of the seriousness of pathology.4) If the patient presenting with otalgia has no local pathology, only by careful patient history and physical examination can all causes in this extensive differential diagnosis be excluded.
Herein, we report an unusual case of large tonsillolith presented with acute otalgia and review the literature on this interesting disease entity. Since tonsil and tonsillar fossa are supplied by the glossopharyngeal nerve, any irritation or pain can be referred to the ear along the tympanic branch of the glossopharyngeal (Jacobson's) nerve.5)
CASE REPORT
A previously healthy 35-year-old woman presented with acute left ear pain lasting for 4 hours. The pain was dull, continuous, with moderate intensity and aggravated during chewing and swallowing. There were no other associated symptoms such as tinnitus, hearing loss, or vertigo. The medical and family histories including recurrent throat infections were insignificant.
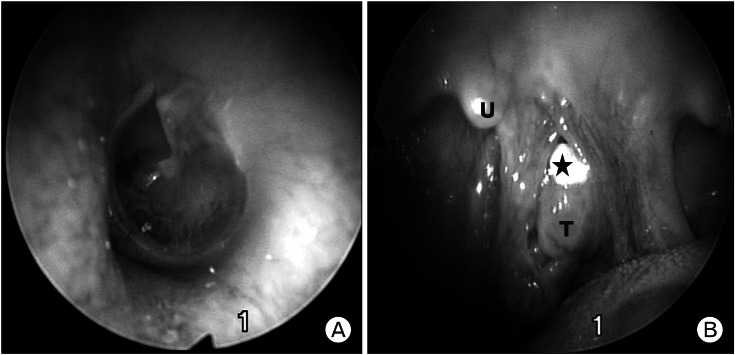
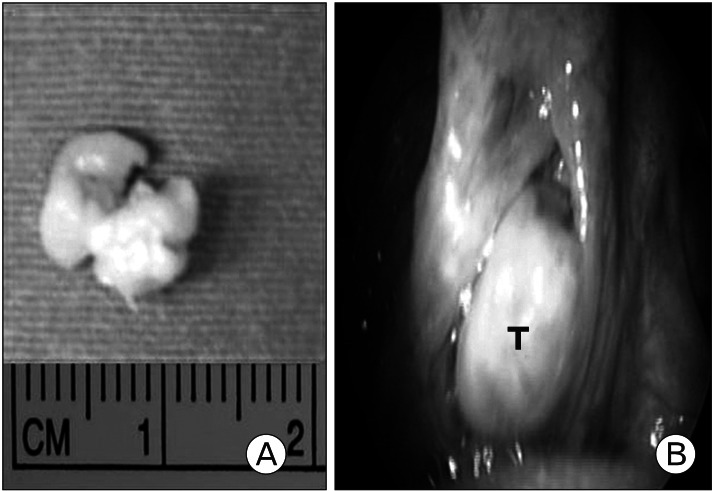
On examination, the ear canal and the ear drum were intact (Figure 1) and there was no evidence of infection. However, she still had persistent pain in the left ear. Because a provisional diagnosis of referred otalgia was made, we performed a further assessment to identify the source of referred pain. On oral examination, a large tonsillolith was observed lodged in the upper pole of the left palatine tonsil (Figure 1). On palpation the mass was hard and nontender. The rest of the nose and throat examination did not reveal any abnormalities. There was no cervical lymphadenopathy. A clinical diagnosis of referred otalgia due to a tonsillolith was made. The tonsillolith was easily and completely removed from the tonsil without any anesthesia (Figure 2). It was yellowish white in color and measured 1.2 ├Ś 0.4 ├Ś 0.7 cm (Figure 2). She reported prompt relief of her otalgia.
DISCUSSION
Referred otalgia or pain that is sensed by the ear but originates from a nonotologic source poses a difficult diagnostic challenge to even the most experienced otolaryngologist. A negative otologic exam and persistent otalgia should suggest the possibility of referred otalgia. The neuroanatomic basis of referred otalgia rests within one of five general neural pathways listed above. One of these general pathways is via the glossopharyngeal nerve (cranial nerve IX).2)
Jacobson's nerve, a derivative of the glossopharyngeal nerve (cranial nerve IX), joins with the caroticotympanic branches from the sympathetic plexus to form the tympanic plexus. This plexus provides sensation to the middle ear, upper eustachian tube, and medial surface of the tympanic membrane. Referred otalgia transmitted by the glossopharyngeal nerve may be secondary to lesions and/or inflammatory processes of the nasopharynx, palatine tonsil, soft palate, or posterior one-third of the tongue.6) Acute pharyngitis, tonsillitis, peritonsillitis, and peritonsillar abscess are common diseases that may cause referred otalgia. Also, patients frequently complain of otalgia after tonsillectomy. In these cases, referred otalgia subsides when the pharynx heals. Lingual tonsillitis and foreign bodies, such as fish bones or chicken bones embedded in the base of the tongue or tonsillar area, are other common causes of referred otalgia.4)
Tonsilloliths are white or yellow colored stones composed of calcium salts such as hydroxyapatit, calcium carbonate apatitie, oxalates, or other magnesium salts, and may contain ammonium radicals.7) Although the exact pathogenesis is not known, fibrosis near the openings of the tonsillar crypts due to repeated inflammation may result in accumulation of bacterial and epithelial debris and formation of retention cysts which can subsequently calcify.8) Recent studies revealed that tonsilloliths exhibit biofilm structure and the formation of chemical gradients through physiological activity.9)
Tonsilloliths may occur singly or in multiples and may be unilateral or bilateral in their presentation. The larger tonsilloliths seem to occur alone whereas the smaller calculi are often seen in multiple.10) Clinical presentations can vary widely depending on the size. Small concretions may be asymptomatic, while more severe forms may present with pain and foreign body sensation in the throat, swelling in the tonsillar fossa, odynophagia, otalgia, peritonsillar abscess, and halitosis.11)
Tonsilloliths may be diagnosed by simple inspection of both tonsillar crypts and can be occasionally confirmed by a panoramic radiograph or computed tomography (CT) without contrast. Because they are composed primarily of calcium and other minerals such as phosphorus, ammonia, carbonate, and magnesium, the imaging findings are usually hyperdense lesions. CT might sometimes be necessary, especially when the lesion is covered by mandibular ramus in plain film.8,12)
The differential diagnosis of tonsilloliths includes radiopacities such as an elongated styloid process, a large maxillary tuberosity, calcifications of arteries, lymph nodes and salivary glands, phleboliths, prominent hamulus of the pterygoid, foreign bodies, abnormalities of the mandibular rami, and a displaced tooth.11) Most tonsilloliths are small and asymptomatic and require no treatment. Small, symptomatic tonsilloliths can be removed manually under local anesthesia, while large, symptomatic tonsilloliths associated with pain, swelling and dysphagia should be removed surgically.12)
In conclusion, I suggest that normal otoscopy should be followed by inspection of the nasal cavities, oral cavity, and oropharynx, with particular note given to the floor of mouth, teeth, tongue, and tonsils, because the identification of a causative etiology is necessary to successfully treat referred otalgia. Also, for better understanding of referred otalgia, the physician should first familiarize his or herself with the anatomic distribution of nerves associated with the ear. Irritation of these nerves, as well as irritation of distant branches of these nerves, may cause the perception of pain within the ear.