INTRODUCTION
It is known that alcohol use disorder (AUD) is a major risk factor for liver cirrhosis, cancer, mental disorder, and death.1) According to the National Health Interview Survey in Korea, 24.9% of males and 7.4% of females qualify as high-risk drinkers, defined as consuming 7 or more standard drinks for men and 5 or more for women at least twice per week.2) The weekly binge-drinking rate, defined as 7 or more standard drinks on a single occasion for men and 5 or more for women, was 40.1% for males and 14.6% for females, and is considerably greater than the world average (16.1% of males, 4.2% of females).3) AUD is a common and important problem not only for individuals but also among their family members. Twenty-three percent of Americans reported that they have a first-degree relative with drinking problem and 38% reported having any relative with drinking problem.4) In almost one-third of married couples, at least one of the couple met criteria for AUD during their lifetime.5)
Several studies have shown that AUD affects family functioning. Although marriage rates are similar between alcoholics and non-alcoholics, separation and divorce rates are about four times greater for AUD-affected families.6) Recent studies have also shown an association between AUD and decreased marital satisfaction, marital adjustment, and increased conflict.7,8,9) One study reported that patients with alcohol dependence and their spouses are likely to have decreased family functioning.10) Another study of 20 couples with husbands with alcohol dependence showed that family functioning was greater during an abstinence phase than while drinking.11) Another study reported that couples with alcoholic husbands reported greater marital distress in both husbands and wives, but wives also reported significantly lower levels of marital satisfaction than their husbands.12) Additionally, one observational study reported that wives' alcohol abuse is also related to lower marital communication.13)
Family communication is how information is exchanged among family members. A family with good communication has better cohesion, can more easily meet the demands of the family members, and has higher family functioning. Families with poor communication are more likely to have lower functioning.14)
As mentioned above, several studies report negative effects associated with alcohol dependence or abuse in the family. However, there have been no large-scale studies concerning the effects of AUD on the family, and only few studies have examined the effects of AUD on family communication. This study investigated the influence of spouse's AUD on family functioning and communication. We conducted a cross-sectional study using data from a cohort of couples who visited primary care in Korea surveyed for family functioning and screened for AUD.
METHODS
1. Study Participants
The FACTS (Family Cohort Study in Primary Care) was established to investigate the relationship between familial environment and health in Koreans. This study was approved by the institutional review board of Asan Medical Center (2011-0567) and all the participants provided written informed consent. Both spouses were over 40 years of age and lived in a household of two or more generations. We collected data from couples who visited 28 family physicians in 22 general hospitals between April 2009 and June 2011 for the treatment of chronic disease such as hypertension and diabetes. A total of 1,040 subjects were enrolled. Among the participants, 57 couples with missing Family Adaptability and Cohesion Scale (FACES)-III or the Family Communication Scale (FCS) scores were excluded. Additionally, 18 couples with missing Alcohol Use Disorders Identification Test (AUDIT) scores were excluded. Altogether, 445 couples without missing data were included in analyses.
2. Measurement of Physical Activity
The tool used for measuring physical activity was the International Physical Activity Questionnaire short-form (IPAQ-SF). The IPAQ-SF has been used worldwide; we used the Korean edition of the IPAQ-SF that has been previously validated.15) The IPAQ-SF measures the amount of time spent in four categories during the last 7 days: vigorous-intensity activity, moderate-intensity activity, walking, and sitting. Participants indicated on how many days and how many minutes they spent conducting activities in each category. This was converted to metabolic equivalents (METs)-minutes by taking the sum of the amount of minutes multiplied by 8 (vigorous), 4 (moderate), 3.3 (walking), or 1.3 (sitting). Participants were classified into 3 activity groups (high, moderate, and low) by the following criteria; at least one of the criteria was required to be classified in each group. The criteria for the high group were: (1) vigorous-intensity activity on at least 3 days and accumulating at least 1,500 METs-min/wk, or (2) 7 or more days per week of any combination of walking, moderate-intensity, or vigorous intensity activity. The criteria for the moderate group were (1) 3 or more days per week of vigorous activity of at least 20 minutes per day; (2) 5 or more days of moderate-intensity activity or walking of at least 30 minutes per day; (3) 5 or more days of any combination of walking, moderate-intensity, or vigorous intensity activities achieving a minimum of at least 600 MET-min/wk. The low-activity group included those participants indicating no activity or not enough activity to meet criteria for the high and moderate groups.
3. Measurement of Alcohol Consumption
Alcohol consumption was classified into two groups using the Alcohol Use Disorders Identification Test in Korea (AUDIT-K). The AUDIT was developed by the World Health Organization (WHO) as a simple method of screening for excessive drinking.16) AUDIT-K is the Korean edition of AUDIT and has been validated for Korean populations.17) AUDIT-K consists of 10 items scored from 0 to 4. Following the WHO's guidelines,16) participants whose AUDIT-K scores were 8 or greater were classified into an AUD group and others were classified into the low-risk group.
4. Measurement of Family Functioning
We evaluated family functioning using the Korean version of the FACES-III. The reliability and validity of the Korean translation of FACES-III has been also established.18,19) FACES-III consists of 20 questions, 10 about adaptability and 10 about cohesion. Each item is scored from 1 to 5 and the sum of these items is the total score. Adaptability and cohesion were classified into 4 groups by total score. The two central groups indicated balanced adaptability or cohesion, while the groups at the extremes indicated unbalanced adaptability or cohesion. Through the combination of adaptability and cohesion, participants were classified into three family types (balanced, mid-range, and extreme).18)
5. Measurement of Family Communication
We investigated family communication using the FCS of the FACES-IV. The Parent-Adolescent Communication Scale (PAC) is composed of two scales. One scale measures the openness of family communication and the other assesses family communication problems. In response to demands for a shorter version of the PAC, Olson and Barnes developed the FCS, a 10-item scale concerning only the extent of open family communication. The FCS has been evaluated for reliability and validity,20) and a Korean version of the FCS has also been validated.21) Each FCS item is scored from 1 to 5 and the sum of these items scores constitutes the total score. We classified family communication into 3 groups by total score. The high group scored 40-50 points; the moderate group scored 36-39 points; the low group scored 10-35 points. Higher scores represent better family communication.
6. Statistical Analyses
The IBM SPSS ver. 21.0 software package (IBM Co., Armonk, NY, USA) was used to perform statistical analyses. All data were separated by gender to investigate any sex-specific effects of alcohol consumption. General characteristics were compared between the spouse-AUD and the spouse-low-risk groups using chi-square tests. The relationships between family type, family communication, and spouse's AUD were analyzed using chi-square tests and logistic regression. For binominal logistic regression, balanced and midrange family groups were combined into one 'appropriate' family-type group, compared to the 'extreme' family types. In the same manner, high- and moderate-communication families were combined into a 'good' communication group, compared to the low or 'poor' communication group. Potential confounds were identified from a comparison of general characteristics using chi-square tests. P-values less than 0.05 were considered statistically significant.
RESULTS
1. Participants Characteristics
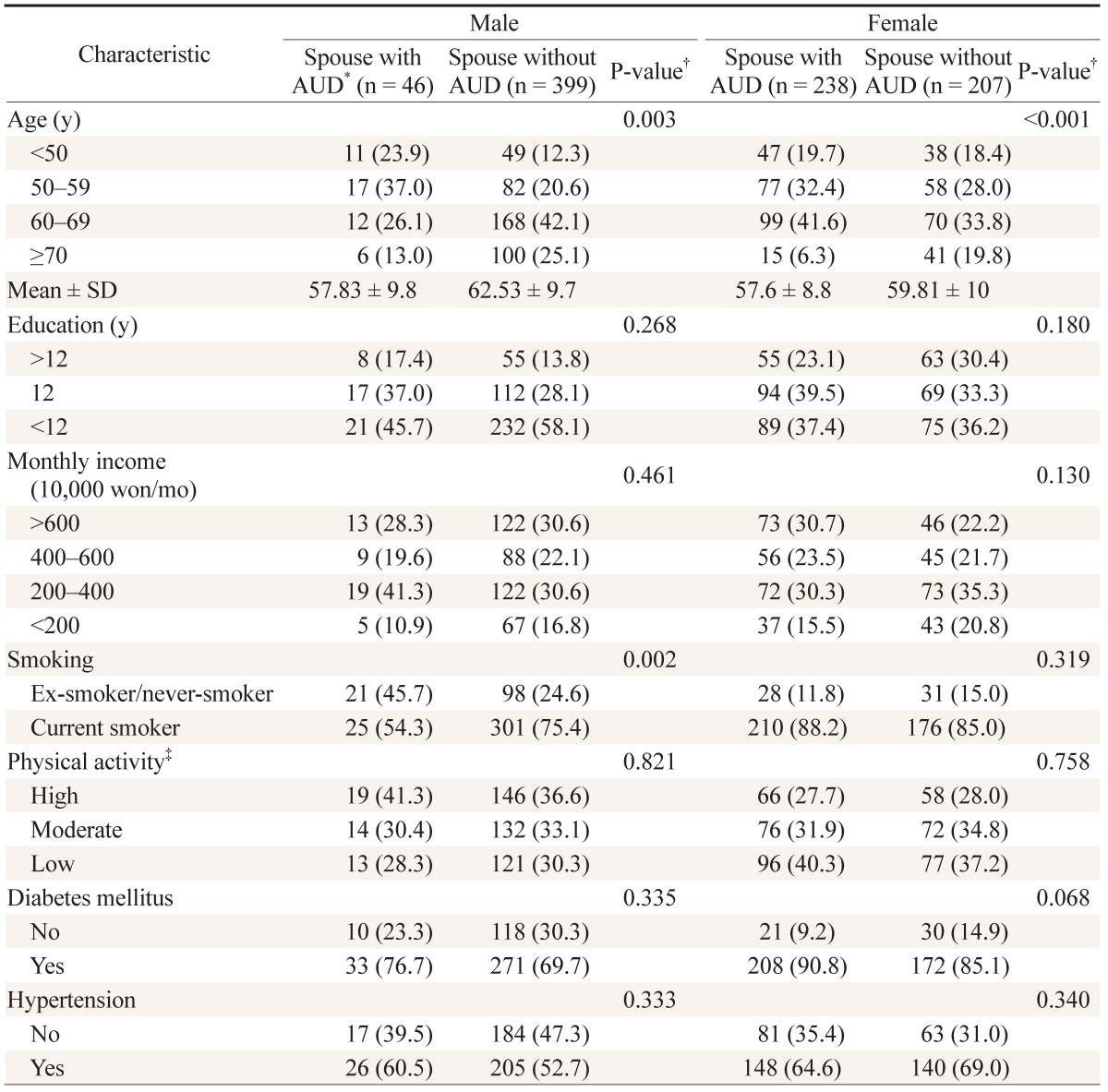
Table 1 shows the baseline characteristics of the participants. Participants with a spouse with AUD were younger than participants without a spouse with AUD for both males and females (mean ┬▒ SD: males, 57.8 ┬▒ 9.8 vs. 62.5 ┬▒ 9.7; P = 0.002; females, 57.6 ┬▒ 8.8 vs. 59.8 ┬▒ 10; P = 0.014). Male participants with a spouse with AUD were more likely to be current smokers than participants without a spouse with AUD (P = 0.01).
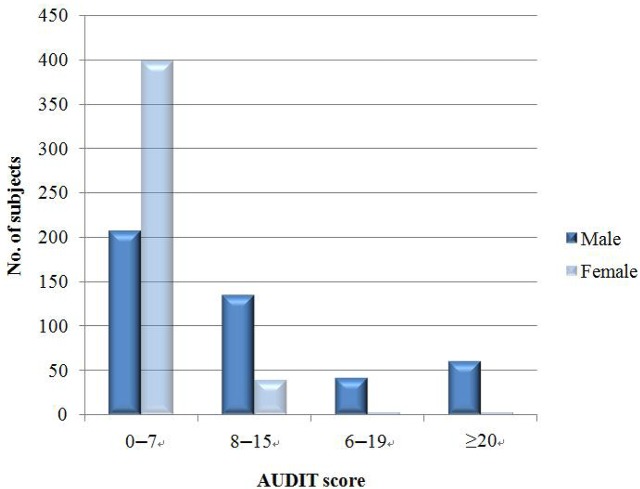
AUD was more frequent among males than females (53.5% vs. 10.3%). To identify the distribution of AUD, we classified participants based on AUDIT scores into low-risk drinkers (scores 0-7), risky drinkers (8-15), hazardous drinkers (16-19), and high-risk drinkers (20 or greater). The proportion of males was greater in the all three AUD groups (Figure 1).
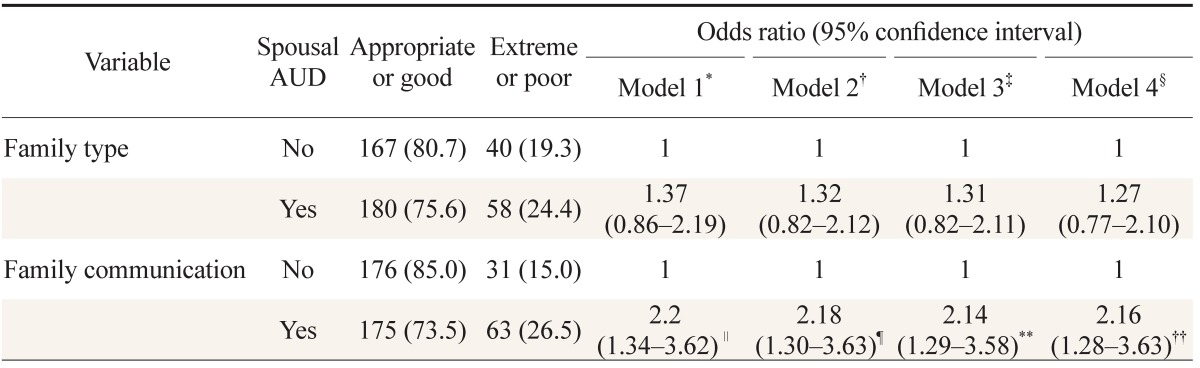
2. Association between Alcohol Use Disorder and Family Functioning and Family Communication
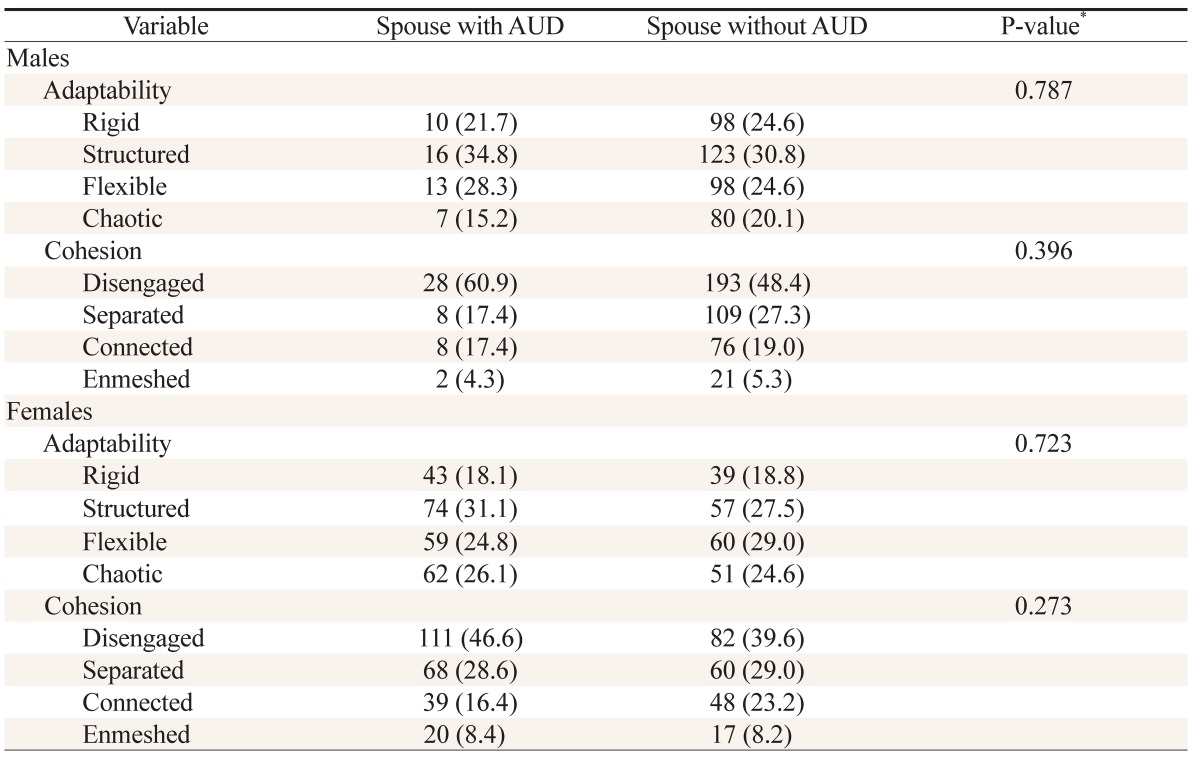
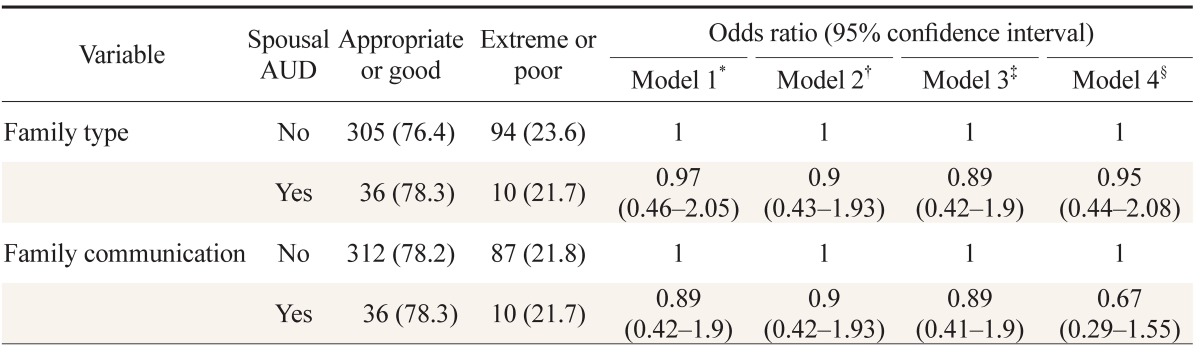
Table 2 shows the comparison of adaptability and cohesion scores between the two AUD groups. There was no significant difference in adaptability and cohesion between participants with a spouse with AUD and participants without a spouse with AUD in both sexes. Tables 3 and 4 show results of multivariate binominal logistic regression for family type and family communication. Variables with significance levels Ōēż 0.1 in the comparison of baseline characteristics between the two groups were considered potential confounds (Table 1). Model 1 was adjusted for age only in both sexes, and model 2 was adjusted for confounds differing by gender. In the case of male participants, model 2 included age and smoking as covariates. Model 2 for females included age and diabetes mellitus. Model 3 adjusted for each participant's own AUD status for both sexes to exclude effects due to one's own AUD on the family. Model 4 adjusted for all possible confounds including factors that could have an effect on family functions. There was no significant difference in family type and communication status between the two groups among males. In females, however, there was a significant increase in odds of lower family communication among women having a spouse with AUD compared to a spouse without AUD (adjusted odds ratio [OR], 2.18; 95% confidence interval [CI], 1.3 to 3.63). Furthermore, after adjusting for each participant's own AUD, this association remained (adjusted OR, 2.14; 95% CI, 1.29 to 3.58). Even after adjusting for all possible confounders (model 4), there remained a significant difference in family communication associated with spousal AUD (adjusted OR, 2.16; 95% CI, 1.28 to 3.63). There was a significant trend of decreasing family communication with increasing spousal AUD score among female participants (P < 0.001; data not shown).
DISCUSSION
In this study, the quality of family communication was worse when having a spouse with AUD among females but not males. The trend was for decreasing family communication with increasing spousal AUD score among females (P < 0.001). To our knowledge, this is the first study showing the effects of AUD on family communication in Korea.
Balanced family type was not significantly associated with spousal AUD for either sex. This is not consistent with previous studies, which have reported an association between AUD and family dysfunction.9,10,11,12) However, these previous studies have evaluated family dysfunction using scales different from those used in our study, such as the Family Assessment Device (FAD) and Dyadic Adjustment Scale. It is possible that our result differ due to discrepancies in the reliability and validity of these family-functioning scales.
It is known that alcoholics are more negative and less positive in their conversations and nonverbal behaviors than their non-alcoholic spouses.22) However, male participants with spouses with AUD did not show worse family communication in our study. This finding is not consistent with a previous study showing a relationship between female problem drinking and distressed communication among couples.13) However, that study recruited analyzed 67 couples, with only 19 couples having an alcoholic wife, and used videotaped communication to assess family communication instead of questionnaires. There are several hypotheses explaining the sex difference of family communication in our results. Because of socioeconomic imbalances between the wife and husband, females and males may have different levels of marital dissatisfaction.23) It is possible that the effects of AUD on communication also differ between males and females. Alternatively, O'Farrell et al.24) reported that couples with an alcoholic husband experienced lower sexual satisfaction and more sexual dysfunction. This phenomenon may lead couples with a husband's AUD, but not with a wife's AUD, to have marital distress and lower family communication. More data should be collected to assess couples with female AUD with proper statistical power.
Our finding that spousal AUD worsened FCS, but not FACE-III, implies a greater sensitivity of the FCS than the FACE-III for assessing family dysfunction. Because we included relatively mild drinkers in our AUD group (AUDIT scores Ōēź 8), it is possible that scales with lower sensitivity could not detect the mild dysfunction in those families.
The prevalence of AUD was greater in males (53.5%) than females (10.3%), as reported in previous literature.5,25) Participants with spousal AUD were younger than participants without spousal AUD for both sexes. This reflects a higher prevalence of AUD in younger groups, which has also been reported in previous studies.26) The proportion of current smokers was greater among participants with a spouse with AUD in males. This is consistent with previous studies showed the association between smoking and heavy drinking.27)
Family functioning is a multidimensional construct reflecting a family's activities and interactions, but there is no consensus on the essential dimensions of family functioning.28) Although FACES-III focused on only the dimensions of family cohesion and adaptability, family communication is also a crucial component of family functioning. Other questionnaires, such as the FAD, contain family communication as one of the dimensions of family functioning. When using FACES-III, dysfunction of a family may be missed due to the absence of this communication dimension, whereas FACES-IV incorporates the FCS.
The strengths of our study include a relatively large number of participants (N = 890) compared to previous studies. Moreover, because we used data from a large cohort consisting of patients visiting a department of family medicine in various hospitals, our study likely reflects the population receiving primary care in Korea. Although several studies have shown the negative effects of AUD on families,9,10,11,12,13) it has not been shown that this association between spousal AUD and family functioning is present among Asians, including Koreans. This is the first study showing a relationship between family communication and spousal AUD in Korean participants.
This study has several limitations. First, because participants were selected from a cohort of participants visiting family physicians, our study has limited generalizability to the general population. Second, the small number of male participants with a wife with AUD (18 participants) is another limitation. For this reason, the effects of a wife's AUD on a husband's family functioning may be underestimated. Moreover, ethnicity and religion could affect patterns of family communication and drinking culture, so the findings of our study may not apply to other regions. In addition, because our study was cross-sectional in nature, the longitudinal effects of spousal AUD are unknown.
In conclusion, among participant families visiting Korean family physicians, a husband's AUD was associated with a wife's lower family communication. However, family type was not associated with AUD. FCS might be a valid and useful tool for detecting family problems, such as AUD. Because of its simplicity, FCS can be implemented easily in clinical settings. Finally, the influence of female drinkers on the family needs to be investigated in further studies.