INTRODUCTION
The number of cancer survivors is increasing because of early detection and advances in treatment. In Korea, 5-year relative cancer survival rates improved to 68.1% in 2008ŌĆō2012 from 41.2% in 1993ŌĆō1995.1)
In cancer survivors, the diagnosis of a new cancer as a second primary cancer (SPC) is an important issue.2) SPCs are a leading cause of mortality among long-term survivors and are more likely to occur in survivors.3,4) Common etiologic factors such as lifestyle, environmental exposures, and genetics, as well as late effects of prior treatment, can influence SPC development.4) Therefore, cancer survivors need to have more thorough and regular cancer screening than people without cancer.5,6,7) However, the few studies that have provided SPC screening rates had limitations such as not considering the effect of sex or the cancer site, or having limited information about cancer sites.8,9,10) Research on SPC screening behavior in female cancer survivors is lacking. As the life expectancy of women increases, cancer incidence and cancer survival rates in women increase. In women, breast cancer is the second most common cancer in Korea. The age-standardized incidence rate of breast cancer in 2012 was 50.7 per 100,000 people, which represents a 5.9% annual increase since 1999. The age-standardized incidence rates for cervical cancer have continuously decreased in Korea, but they are higher than those in developed countries.1) The National Cancer Screening Program (NCSP) provides women over 40 years of age with breast cancer screening and women over 30 years of age with cervical cancer screening biannually.11) The NCSP set a goal of achieving a screening rate of 70% by 2015.12) Although high cancer screening rates were expected, the SPC screening rate was only 37.7% in 2009, which is much lower than those in other developed countries.13)
We investigated the screening rates for breast and cervical cancer in Korean female cancer survivors compared to women without cancer, and we investigated factors associated with breast and cervical cancer screening behavior.
METHODS
1. Study Population
Data were obtained from the fourth and fifth Korean National Health and Nutrition Examination Surveys (KNHANES), 2007ŌĆō2012. KNHANES is a national representative survey that is carried out by the Korea Centers for Disease Control and Prevention. The survey includes approximately 10,000 individuals annually with data collected by multistage probability sampling.14,15) Among 35,996 adults over 19 years of age, we selected 18,135 women who were 30 years of age or older. Participants were divided into two groups: cancer survivors and non-cancer controls. Cancer survivors were defined as those individuals reporting ever being diagnosed with any solid or hematologic cancer by a doctor. Among the remaining participants, we selected non-cancer controls who were not diagnosed with any cancer. This study was approved by the institutional review board of Samsung Medical Center (IRB no. 2015-12-020).
2. Data Collection
Screening behavior for breast and cervical cancer was obtained through self-reported questionnaires. Screening methods were defined as a mammogram or Papanicolaou test. The interval period of cancer screening was limited to within 2 years.
The sociodemographic variables included marital status, education level, household income, employment, and medical history of cancer or other comorbidities, which were obtained though face-to-face interviews. Health behaviors, such as smoking and alcohol use, were assessed using a self-administered questionnaire.
Education level was defined by the highest level achieved: less than high school, high school, or college and above. Monthly household income was classified according to quartiles: Q1 (lowest), Q2 (lower intermediate), Q3 (higher intermediate), or Q4 (highest). Smoking status was classified into 3 groups: never smoker, former smoker, or current smoker. Alcohol drinking status was defined as Ōēź1 time/mo or <1 time/mo. Comorbidity was defined as hypertension, hyperlipidemia, stroke, angina, myocardial infarction, osteoarthritis, rheumatic arthritis, asthma, renal insufficiency, hepatitis B or C, diabetes, or liver cirrhosis, as determined by a doctor's diagnosis. The time since cancer diagnosis in the survivor group was classified into 3 groups; less than 5 years, 5ŌĆō10 years, or more than 10 years.
3. Statistical Analyses
The general characteristics and prevalence of breast and cervical cancer screening were compared between cancer survivors and the non-cancer controls using a chi-square test. Differences in cancer screening rates were compared according to cancer site: thyroid, stomach, colon, breast, and cervix. We excluded the mammogram in breast cancer survivors and the Papanicolaou test in cervix cancer survivors. The analysis consisted of a one-way analysis of variance with a post hoc Dunnett test. Multiple logistic regression analysis was used to investigate factors associated with cancer screening behavior after adjusting for age, marital status, education level, household income, employment, smoking, alcohol use, and comorbidities. All analyses were conducted using IBM SPSS ver. 21.0 software (IBM Corp., Armonk, NY, USA), taking sampling weights and the complex survey design into consideration. We considered P-values less than 0.05 to be statistically significant.
RESULTS
The general characteristics of the 738 cancer survivors and 17,027 non-cancer controls are shown in Table 1. Cancer survivors were older and had lower levels of education, household income, and employment compared to the non-cancer controls. The cancer survivors were less likely to smoke and drink alcohol and had more comorbidities than the non-cancer controls.
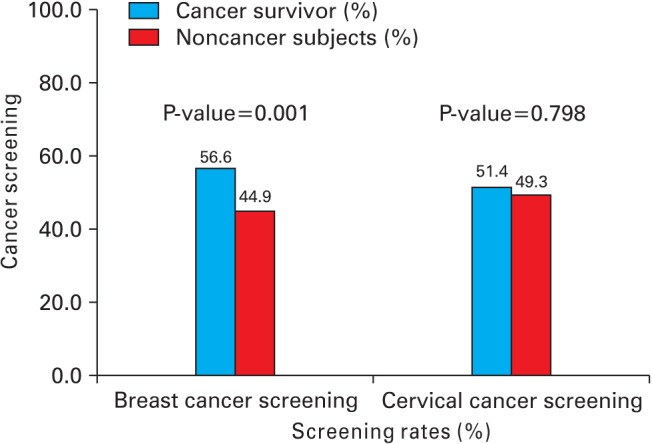
The cancer screening rates of the cancer survivors and non-cancer controls are shown in Figure 1. The cancer survivor group was significantly more likely to have breast cancer screening than the non-cancer controls (56.6% versus 44.9%, P=0.001). However, cervical cancer screening practices were not significantly different between cancer survivors and women in the non-cancer control group (51.4% versus 49.3%, P=0.798). Multiple regression analysis after adjusting for sociodemographic factors showed similar results (Table 2).
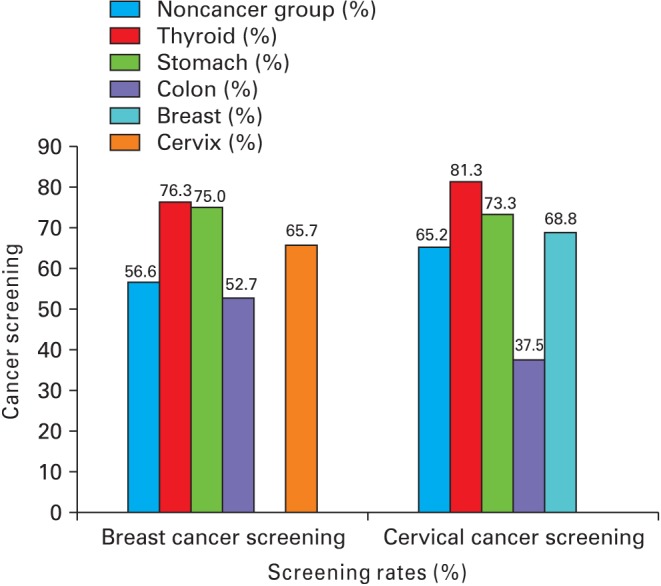
Differences in cancer screening rates according to the most common cancer sites in Korean women are shown in Figure 2. Thyroid and stomach cancer survivors had higher rates of breast cancer screening than women in the non-cancer control group. Thyroid cancer survivors also had higher screening rates than cervical cancer survivors. Colon cancer survivors had lower screening rates for cervical cancer than women in the non-cancer control group.
The rate of cancer screening evaluated according to the time since diagnosis is shown in Table 3. In terms of breast cancer screening, cancer survivors showed no significant difference in screening rates five years after their cancer diagnosis. However, cancer survivors were less likely to have cervical cancer screening 10 years after their cancer diagnosis.
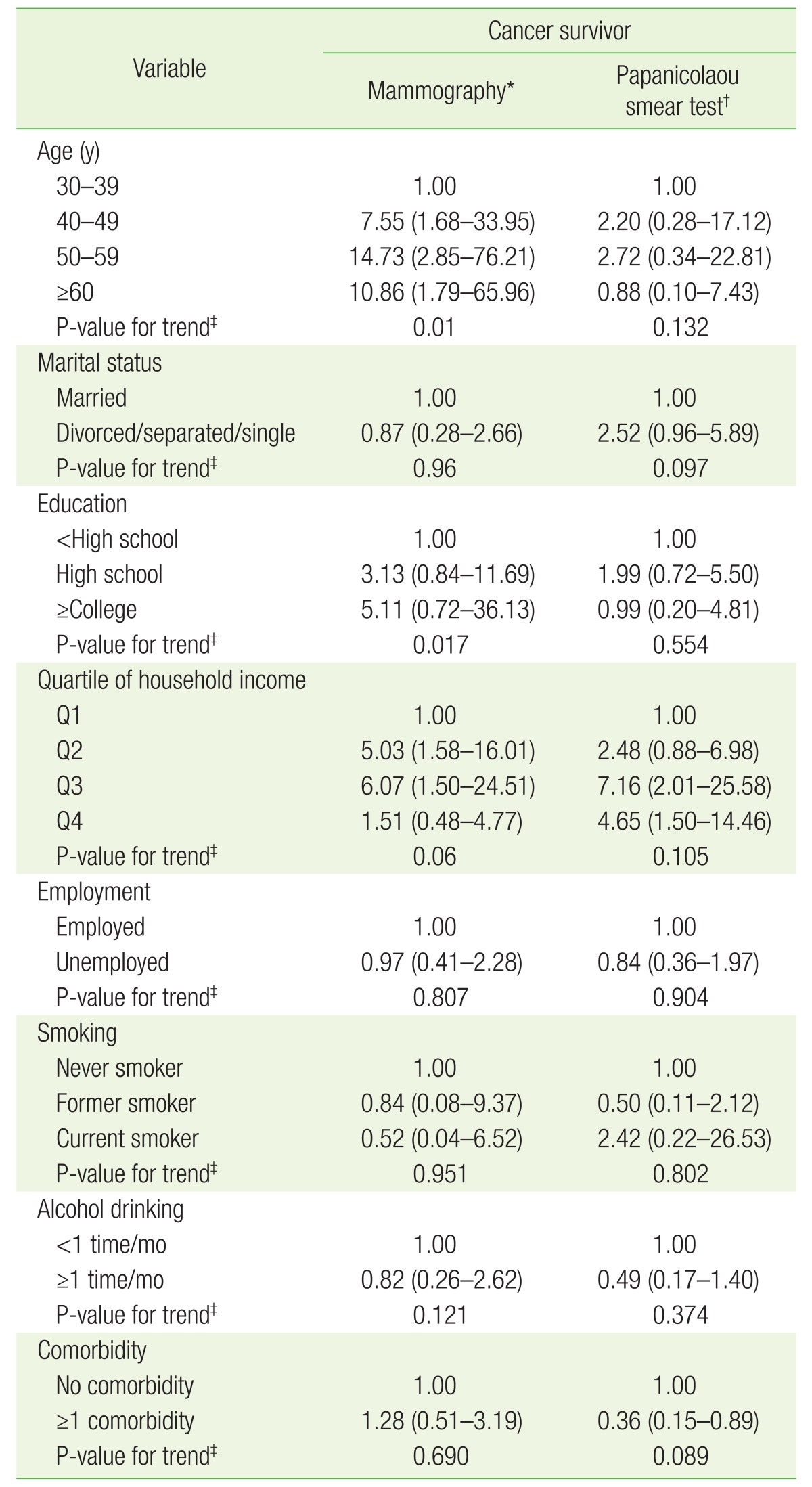
The factors associated with cancer screening behavior in the cancer survivors are shown in Table 4. Only women over 40 years of age had significantly higher breast cancer screening rates.
DISCUSSION
In this study, women in a cancer-survivors group were more likely to undergo breast cancer screening than women in a non-cancer control group. Nonetheless, half of the cancer survivors did not undergo cancer screening. There were no sociodemographic factors or health behaviors that were significantly associated with breast and cervical cancer screening, with the exception of having an age over 40 years, which was positively associated with breast cancer screening.
We propose several reasons for the low rate of cancer screening in female cancer survivors. First, cancer survivors believe that cancer screening is not necessary because they have routine medical examinations.13,16) Second, there is a lack of physician recommendations about SPC screening. Past studies on perceptions and attitudes about SPC screening among Korean cancer survivors have shown that cancer survivors have positive attitudes towards SPC screening, even though most do not receive cancer screening.13,17) A study of women without cancer in Korea found that the most common reasons for not participating in cancer screening programs were ŌĆśnot feeling the needŌĆÖ and ŌĆśnot having time.ŌĆÖ18) However, cancer survivors perceive themselves as having a greater risk of developing SPC,10,13,17) and they visit health care providers more frequently than the general population.19,20,21) These factors may affect SPC screening rates. Also, in previous studies, cancer survivors followed up by both primary care providers and oncologists were more likely to have SPC screening and other comprehensive care compared to those who were only seen by oncologists.22,23) Thus, we think that the role of primary care providers for following cancer survivors is important in improving SPC screening rates.
Comparing breast and cervical cancer screening rates according to cancer site, our results revealed that stomach and thyroid cancer survivors had greater than 70% screening rates for breast and cervical cancers. However, of colon cancer survivors, only 52.7% had breast cancer screening and 37.5% had cervical cancer screening, which was lower than the rates in non-cancer controls. These findings were consistent with previous studies.13,20,24) However, in previous studies, the much lower rate of SPC screening for female colon cancer survivors was noted as a weak point of their health care and promotion policy. Survivors of breast and cervical cancer were expected to have higher rates of screening with mammograms and Papanicolaou testing, respectively, because of the common hormone receptors underlying the pathogenesis of both diseases. However, the screening rates in these groups were not different from those of the non-cancer controls or survivors of cancers at other sites. Therefore, patient education and physicians' recommendations are needed for these patient populations.
Our findings suggest that sociodemographic factors and health behaviors are not significantly associated with breast and cervical cancer screening rates in female cancer survivors. In a previous study, cancer survivors with high household incomes were more likely to undergo cancer screening than those with low household incomes.8) We propose that people in the middle range of household incomes may have more easy access to the NCSP. Since 2005, the NCSP has been free for Medical Aid recipients and National Health Insurance participants in the lower half of the income stratum.25) The NCSP might have reduced the effect of household income on cancer screening practices. Other studies on breast and cervical cancer screening in the general population show that it is associated with education level, marital status,18,26) smoking,27) and alcohol use.28) However, our results indicate that the marital status, education level, smoking, and alcohol use of female cancer survivors were not significantly associated with cancer screening rates.
Generally, the rate of SPC screening declines with time since the primary cancer diagnosis.13,24,29) Accordingly, the cancer survivors in our study surviving more than 10 years after their cancer diagnosis were less likely to undergo cervical cancer screening, which was thought to be due to the fact that they were too old to undergo routine cervical cancer screening. However, for breast cancer screening, we found no decrease in screening rates with time.
This study had several strengths. We excluded breast and cervical cancer survivors for our overall analysis to rule out their influence on overall cancer screening rates; therefore, our data reflect a representative sample of the general population in Korea.
A limitation of this study was the use of secondary data. KNHANES did not provide clinical data such as cancer stage and the method of cancer treatment. Also, we could not explain the causal relationship between cancer screening rates and sociodemographic factors because the study design was cross-sectional. KNHANES is based on self-reported questionnaires, introducing the possibility of recall bias. However, in the self-reported data, both cancer screening paid for by the government and screening paid for by individuals can be included in the analysis of screening behavior.
In conclusion, a substantial proportion of women cancer survivors do not undergo breast and cervical cancer screening. However, unlike previous studies, sociodemographic factors showed no significant effects on screening rates. We need to comprehensively understand other factors that affect SPC screening behavior in female cancer survivors such as their knowledge and the perceptions of both cancer survivors and physicians.