The Influence of Negative Mental Health on the Health Behavior and the Mortality Risk: Analysis of Korean Longitudinal Study of Aging from 2006 to 2014
Article information

Abstract
Background
Several studies have shown that negative mental health increases risky health behavior and mortality risk. We investigated the relationship between mental health and health behavior, and the causal association between mental health and mortality risk.
Methods
We used data from the 8-year (2006–2014) Korean Longitudinal Study of Aging with a cohort of 10,247 individuals (whom we divided into a younger group aged <65 years and an older group aged ≥65 years). Mental health was assessed with the following factors: depression, social engagement, and satisfaction of life. Health behavior was assessed with smoking, alcohol use, and regular exercise. Mortality risk was calculated using survival status and survival months as of 2014. Multiple logistic regression and Cox proportional hazard analysis were performed.
Results
Negative mental health was associated with current smoking and sedentary life style, but not with alcohol consumption. In addition, it was associated with an increase in all-cause mortality risk. The increase in mortality risk in the highest quartile (vs. lowest) was 1.71 times (hazard ratio [HR], 1.71; 95% confidence interval [CI], 1.12– 2.62) and 2.07 times (HR, 2.07; 95% CI, 1.60–2.67) for the younger and older group, respectively.
Conclusion
Our results show that mental health affects health behavior and mortality risk. A key inference from this study is that improving mental health can lead to positive changes in health behavior and reduce the risk of mortality.
INTRODUCTION
Mental health is defined as “a state of wellbeing” and includes psychological as well as social well-being. It affects how people think, feel, and act [1]. It also determines how they handle stress, relate to others, and make choices. In current times, rapid social change, stressful working conditions, and unhealthy lifestyles are some factors that pose a risk to mental health. The concern for mental health is increasing worldwide as good mental health is associated with the social and intellectual skills needed to deal with new challenges [2,3].
Mental health and mental illness are interrelated but independent concepts. The former refers to “psycho-social wellbeing,” and the latter to disorders diagnosed by the Diagnostic and Statistical Manual of Mental Disorders, 5th edition. An individual might not have a mental illness, and still not be mentally healthy, and the opposite is also possible [4].
A person’s mental health is formed by psychological processes, interacting with social, economic, and physical circumstances. In the “tentative schematic representation of psychosocial pathways” model, Martikainen et al. [5] in 2002 raise two questions about mental health processes―what the relevant social structural forces are, and how these forces might influence individual characteristics. To answer these questions, they describe macro-, meso-, and micro-level social frameworks, and how they interact with an individual’s characteristics and experiences over a lifetime, to influence mental health. In other words, the social structural forces (the macro- and meso-level social processes) lead to the perceptions and psychological processes at the individual level [6].
Extensive scientific evidence points to the association between mental health, health behaviors, and health outcomes [7]. Mental health plays a role in health outcomes in the following ways [8]. First, through the psycho-biological routes, it affects neuro-endocrine, cardiovascular and immune systems. Second, it contributes to the adaptation of health behavior.
In this study, we conceptualized mental health as the interaction of social factors and individual characteristics, assessing it using the variables of depression, social engagement (SE), and satisfaction of life (SoL). We assessed smoking, alcohol consumption, and regular exercise as health behaviors. Mortality risk was estimated using all-causes mortality. Furthermore, we investigated the cross-sectional association of mental health and health behaviors, and the causal relationship between mental health and mortality risk.
METHODS
1. Study Population
We used the data from a cohort of 10,254 persons from the Korean Longitudinal Study of Aging (KLoSA) for an 8-year period from 2006 to 2014. KLoSA used a nationwide, stratified, multistage sample of adults, aged 45 to 79 years. This panel study was repeated every 2 years with detailed interviews and computer-assisted personal interviewing. Seven cases with missing health information at baseline were excluded, leaving 10,247 in the study sample. Information relating to deaths, including the date and cause of death, was obtained from family members in the household. We classified the study population into two subgroups, based on age: a younger group aged <65 years and an older group aged ≥65 years (Figure 1).

Flow chart of participants
2. Independent Variables: Mental Health Variables
Referring to previous studies [9-11], we selected three variables from the KLoSA data: depression, measured by the 10-item Center for Epidemiologic Studies Depression Scale (CES-D10) [12], SE, and SoL.
1) Depression (CES-D10)
Depression was measured using the Korean version of CES-D10, a self-report measure of depression [13]. A total score, ranging from 0–30, was calculated by summing up the scores of the 10 items.
2) Social engagement
SE was consisted of 7 factors: (1) frequency of contact with friends; (2) frequency of contact with a mutual benevolence group; (3) frequency of attendance in leisure, culture and sports activities; (4) frequency of attendance in religious activities; (5) frequency of contact with an alumni or hometown alumni group and family group; (6) frequency of participation in volunteer work; and (7) frequency of participation in political activities. The score for each factor was calculated as follows: every day=5, more than once a week=4, more than once a month=3, more than twice a year=2, and once a year or not at all=1. Summing up the scores for the seven items provided a total score ranging from 7–35.
3) Satisfaction of life
The question of SoL was as follows. How satisfied are you with your overall quality of life (happiness) compared to others in your age group? The respondent’s subjective satisfaction of life was assessed by choosing between 0 and 100.
3. Index Scoring for the Mental Health Variables
In addition, we created a composite mental health score by adding the index scores of the three mental health variables. The index scores and cut-off points for each variable were obtained by the following process.
1) CES-D10
We ranked the participants according to their CES-D10 scores, and divided them into four groups. Each group was then assigned an index score, ranging from 0–1. The lowest group (D1; scores, 0–3) was assigned 0, the second group (D2; scores, 4–9) was assigned 0.33, the third group (D3; scores, 10–13) was assigned 0.67 and the fourth group (D4; scores, 14–30) was assigned 1. This was done for both the younger and older groups.
2) Negative SE
The SE scores were converted to quartiles after ranking them in reverse order: the first quartile (Q1; SE scores ≥17) was assigned 0, the second quartile (Q2; SE scores 14-16) was assigned 0.33, the third quartile (Q3, SE scores 8-13) was assigned 0.67, and the last quartile (Q4, SE score= 7) was assigned 1, in both the groups.
3) Negative SoL
SoL scores were converted to quartiles and index scored in reverse order: in the younger group, Q1 (score, 80–100)=0, Q2 (score, 70–79)=0.33, Q3 (score, 60–69)=0.67, and Q4 (score, 0–59)=1; and in ≥65 y, Q1 (score, 80–100)=0, Q2 (score, 60–79)=0.33, Q3 (score, 50–59)=0.67, and Q4 (score, 0–49)=1.
4) Negative mental health
By reviewing similar studies which used cumulative scores [11,14], we created a negative mental health score by summing up the index scores of CES-D10, SE, and SoL. This score ranged from 0–3. The negative mental health score was converted to quartiles and ranked in reverse: for the <65 years group, the quartile scores were Q1 (score, 0–0.67)=0, Q2 (score, 0.68–1.08)=0.33, Q3 (score, 1.09–1.42)=0.67, and Q4 (score, 1.43–3.00)=1. For the ≥65 years group, the quartile scores were Q1 (score, 0–0.83)=0, Q2 (score, 0.84–1.25)=0.33, Q3 (score, 1.26–1.67)=0.67, and Q4 (score, 1.68–3.00)=1.
4. Dependent Variables: Health Behavior and All-Cause Mortality Risk
1) Health behavior
Health behavior consisted of three variables: smoking, alcohol use, and regular exercise. Smoking status was categorized as current smoker, past smoker, and non-smoker. Non-smokers were defined as persons who smoked less than five packets (100 cigarettes) a year in their lifetime. Alcohol use was similarly categorized as current drinker, past drinker, and non-drinker. Regular exercise was defined as exercising more than once a week.
2) Mortality risk
All-cause mortality risk was assessed using survival status (dead, dropped out, or survived) and survival months, or the months lived since the baseline period till the end of the study. Under all-cause mortality, we included all deaths, except those from suicide, murder, accident, or an unknown cause. The excluded causes of death were treated as censored (n=87; 2nd wave=13, 3rd wave=16, 4th wave=17, and 5th wave=41).
5. Covariates
Referring to previous studies [15,16], we included age, sex, marital status (married, single), cohabiting status (cohabiting, single), education level, household income, number of chronic diseases, and health behaviors (smoking status, alcohol use status, and regular exercise) as covariates.
6. Hypothesis
We suggested two research hypotheses using the “tentative schematic representation of psycho-social pathways”: [5] (1) mental health is associated with health behavior, and (2) mental health is causally related to mortality risk (Figure 2).
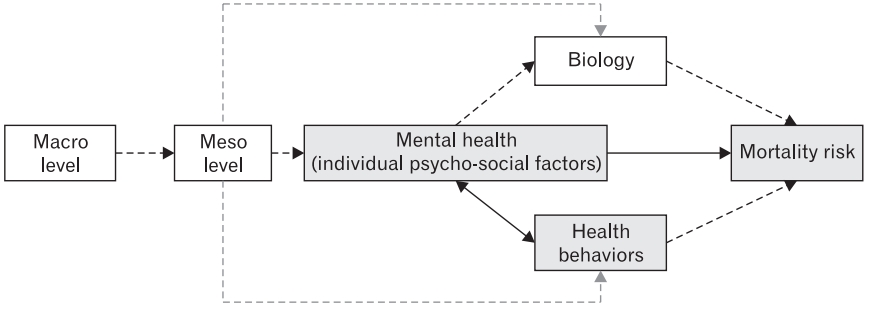
A tentative schematic representation of psycho-social pathways. Meso-level effects refer to the group effects of how norms are organized. These groups include “religious institutions,” “white or blue collar,” “sports clubs,” “neighborhood,” and “family.” Meso-level effects on mental health are in the form of “stress perception or social isolation.” Macro-level effects refer to the large-scale effects of how norms are organized. These include “social structures and institutions,” “large-scale patterns,” and phenomena such as “globalization.” The pathways depicted by solid lines were analyzed in this study, whereas those depicted by dotted lines were not.
7. Statistical Analysis
Analysis was carried out in two directions. First, multiple logistic regression was performed cross-sectionally to explore the relationship between mental health and health behavior. Second, Cox proportional hazard regression analysis was conducted longitudinally to investigate the causality between mental health and mortality risk.
RESULTS
During the 8-year follow-up of the study population (N=10,247), 12.2% (N=1,254) died, 19.2% (N=1,974) were censored, and 68.6% (N=7,029) survived (Figure 1). At baseline, 59.4% (N=6,090) of the sample was younger than 65 years and 40.6% (N=4,157) was 65 years or older.
Demographic characteristics differed according to age. The elderly group (≥65 years) was more likely to be single, had lower education, and lower household income compared with the younger group (<65 years). Health behaviors differed according to gender, with women being healthier than men except in regular exercise. However, there was no difference in alcohol use according to gender. Additionally, the older men had better health behaviors than the younger men; they smoked and drank less. Whereas the older women smoked more but drank less than the younger women. Higher CES-D10, negative SE, negative SoL, and negative mental health were associated with poorer health behavior and increased mortality rate. Mental health vulnerability was higher among the elderly and women (Tables 1, 2).

Scores on mental health dimensions according to age and gender at baseline (2006)

Survival months and mortality rate by mental health dimensions at baseline (2006)
1. The Association between Mental Health and Health Behavior
The association between negative mental health and risky health behavior was analyzed after stratification by age and gender.
Among men, after adjusting for the covariates, (1) the highest negative mental health quartile (Q4) had higher risky health behaviors, compared with the lowest quartile (Q1): increased current smoking rate by 1.61 times and 1.53 times, and increased rate of no regular exercise by 2.79 times and 2.30 times in the younger and older groups, respectively; however, there was no difference in current drinking across the two groups. (2) The highest CES-D10 group (D4) compared with the lowest CES-D10 (D1) had decreased regular exercise by 2.68 times and 2.22 times in the younger and older groups, respectively and no difference in current drinking; however, the higher CES-D10 group had decreased current drinking by 0.48 times in the younger group. (3) The highest negative SE quartile (Q4) compared with the lowest negative SE (Q1) had increased current smoking rate by 1.44 times and 1.25 times, and decreased regular exercise rate by 2.39 times and 2.06 times in the younger and older groups, respectively; however, there was no difference in current drinking across the groups. (4) The highest negative SoL quartile (Q4) compared with the lowest negative SoL (Q1) had increased current smoking rate by 1.48 times and 1.57 times, and decreased regular exercise rate by 1.69 times and 2.66 times in the younger and older groups, respectively; however, there was no difference in current drinking across the groups.
For women, after covariate adjustment, (1) the highest negative mental health quartile (Q4) had increased risky health behaviors compared with the lowest (Q1), including: increased current smoking rate by 5.64 times and 2.04 times, and decreased regular exercise rate by 3.76 times and 3.76 times in the younger and older groups, respectively; however, there were no differences in current drinking across the groups. (2) The highest CES-D10 group (D4) compared with the lowest (D1) had: increased current smoking rate by 5.87 times and 4.02 times in the younger and older groups, respectively; and decreased regular exercise rate by 1.98 times in the older group; moreover, the highest CES-D10 group had decreased alcohol drinking rate by 0.68 times in the younger group. (3) The highest negative SE quartile (Q4) compared with the lowest (Q1) had: increased current smoking rate by 4.14 times and 1.71 times; decreased regular exercise rate by 2.37 times and 2.16 times in the younger and older groups, respectively; however, there was no difference in current drinking in both the groups. (4) The highest negative SoL quartile (Q4) compared with the lowest (Q1) had: increased current smoking rate by 3.16 times and 1.75 times; decreased regular exercise rate by 2.49 times in and 2.19 times in the younger and older groups, respectively; however, there were no differences in current drinking in both the groups (Table 3).
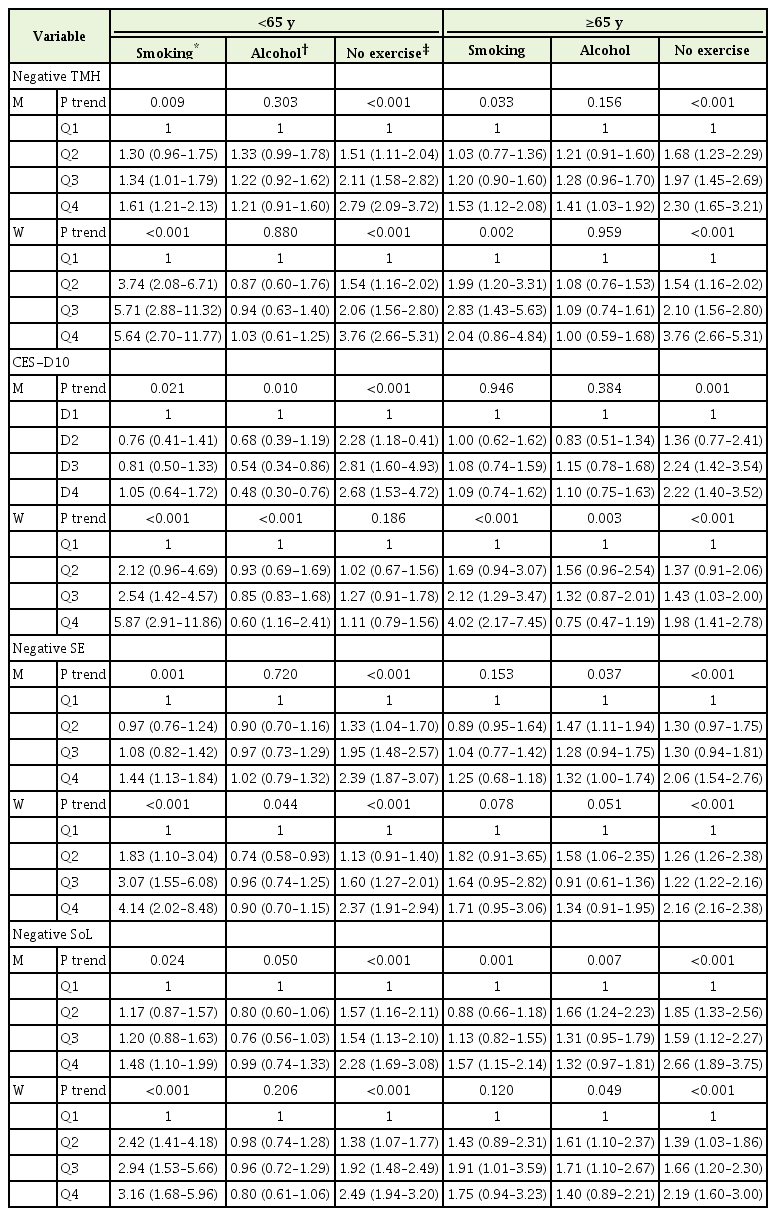
The relationship between mental health, depression, social engagement, satisfaction of life, and mortality risk by multiple logistic regression analysis, the Korean Longitudinal Study of Aging at baseline (2006)
In both men and women, negative dimensions of mental health had dose-response relationships with risky health behaviors, except for alcohol use. In particular, smoking was strongly related to women’s negative mental health, and regular exercise was the health behavior most associated with mental health.
2. Mental Health Affected Mortality Risk
Survival analysis of the negative mental health variable was carried out after stratification using the age of 65 years. After covariates were adjusted, (1) the highest negative mental health quartile (Q4) compared with the lowest (Q1) had: increased mortality risk by 1.71 times and 2.07 times in the younger and older groups, respectively, (2) The highest CES-D10 group (D4) compared with the lowest (D1) had: increased mortality risk by 2.97 times and 2.21 times in the younger and older groups, respectively, (3) The highest negative SE quartile (Q4) compared with the lowest (Q1) had: increased mortality risk by 1.93 times and 1.62 times in the younger and older groups, respectively, and (4) The highest negative SoL quartile (Q4) had increased mortality risk by 1.62 times in the younger group and the highest negative mental health quartile (Q4) had increased mortality risk by 1.71 times and 2.07 times in the younger and older groups, respectively (Table 3). We found dose-response associations of negative mental health across the four dimensions and an increased mortality risk (Table 4, Figure 3).

All-cause mortality HRs and 95% CIs for quartiles on the mental health dimensions, the Korean Longitudinal Study of Aging, 2006–2014

All-cause mortality hazard ratios for the mental health dimensions, the Korean Longitudinal Study of Aging 2006–2014. (A) Dose-response causal relationship between negative total mental health and all-cause mortality. (B) Dose-response causal relationship between depression and all-cause mortality. (C) Dose-response causal relationship between negative social engagement and all-cause mortality. (D) Dose-response causal relationship between negative satisfaction of life and all-cause mortality. TMH, total mental health; CES-D, Center for Epidemiologic Studies-Depression; SE, social engagement; SoL, satisfaction of life; HR, hazard ratio.
DISCUSSION
Similar to previous studies [17,18], a dose-response association of mental health with health behaviors and mortality risk remained after adjusting for covariates. There is a wealth of evidence to show that positive mental health influences a wide range of health outcomes such as healthier lifestyles, better physical health, higher social cohesion, and reduced mortality risk.
Mental health essentially refers to a person’s psychosocial wellbeing, which means how well a person can cope with the stresses of life, work productively and fruitfully, and make a contribution to her or his community. Psychosocial factors can be regarded as including socioeconomic position (SEP) and individual psychological factors; in our study, we have replaced it with mental health. The “schematic representation of psycho-social pathways” model on which this study was based, suggests that SEP is reflected in mental health. The extent to which SEP involves exposure to psychological (in addition to material) risks and buffers is of special interest from a mental health perspective. SEP also influences constructs like identity and social status, which in turn impact mental health [5].
According to the model, psychosocial factors (mental health) can be best seen and operationalized in terms of the influences acting primarily between the social (or the meso-level) and the individual level (or the micro-level). The following statement provides an example of the relationship between the social and individual levels: “Unemployment that leads to loss of income is not a mental health issue, whereas the loss of self-esteem that accompanies unemployment is.” [5]
Mental health is not the only factor influencing physical health, but it is assumed to play a pivotal role. It pervades physical health through two mechanisms. First, it affects hormone secretion and inflammation through neuro-endocrine, cardiovascular, and immune systems. Second, it influences the choice of health behaviors [18,19].
Studies have shown that improving mental health reduces alcohol consumption and smoking, and increases physical activity. Our study showed that negative mental health decreased regular exercise in both genders, and increased current smoking in women. However, the effect of mental health on current drinking was not significant, regardless of gender and age. This may be interpreted within the social drinking culture (such as business drinking and stress-related drinking) and high rates of drinking in Korean society [20]. Rates of smoking among men was twice as high as that in other countries, while it was much lower among women [21,22]. Therefore, current smoking is highly relevant to negative mental health, and requires attention. Global researches have showed that mental health is not universally correlated to all forms of risky health behaviors [23]. A significant interpretation of the link between mental health and health behaviors is that risky health behaviors might be a survival strategy when faced with problems. Unhealthy behavior may be chosen in circumstances in which the health behavior that determines the future cannot be controlled. In other words, because people believe that future rewards are uncertain, they choose harmful health behaviors with immediate rewards over positive health behaviors with rewards in the future. Choosing risky health behavior is called “present-oriented behavior” and choosing beneficial health behavior is called “future-oriented behavior.” [24] Motivation to choose health behaviors is strongly influenced by mental health, making these pathways a component of the growing interest in mental health and as a route to achieving behavior change [25].
The influence of mental health on mortality has been widely asserted [26,27]. A key rationale for promoting mental health is that through improving mental health, we can modify health outcomes, even other risk factors remain [26]. In our results, the mortality risk increased as mental health dimensions worsened, although SoL did not increase mortality risk in the younger group. The subjective meaning of SoL may vary depending on age. Young adults might be relatively dissatisfied, with high expectations for goals, and such dissatisfaction represents, in part, a rather positive mental health [28]. With the exception of SoL, the effects of mental health on mortality risk were greater in the elderly group.
The limitations of the study are as follows. First, although existing literature was referenced [1,27], the measurement of mental health was somewhat arbitrary and lacked sufficient validity. The three measures of CES-D10, SE, SoL were not adequate to represent mental health as a whole. However, within the limitations of the KLoSA data, we extracted variables that could be included in the mental health domains and analyzed the relevance of these variables to health behavior and mortality risk. Second, it is not appropriate to express mental health scores by summing up index scores of the three variables. Each of the three variables has a different degree of impact on health behavior and mortality risk, and has conceptually overlapping aspects. However, in order to analyze the comprehensive effects of mental health, the index scores of the three variables were summed up and expressed as a composite mental health score. Third, because the respondent’s perceptions were subjective and their recall might be imperfect, the data may contain information bias and recall bias. In particular, data relating to deaths may contain these biases, as they were obtained from family members rather than from official sources. Fourth, the measurement of health behavior in this study may be said to be oversimplified. Simple categorical variables tend to underestimate differences in measurement and effect.
Nevertheless, our research has the following strengths. First, we obtained a nationwide, longitudinal, and large sample size. So, the results can be generalized to the Korean population, aged over 45 years. Second, the use of the psycho-social model (Figure 2) enriches the understanding of the causal relationship between of mental health and mortality risk through the incorporation of health behavior.
Notes
No potential conflict of interest relevant to this article was reported.