INTRODUCTION
Smoking is one of the most serious and dangerous factors among the correctable health risk factors, and 30% of all cancers and 90% of cancers in organs in direct contact with tobacco smoke (oral cavity, esophagus, lung, bronchus) are caused by smoking [1]. In 2004, the US surgeon generalŌĆÖs report showed that cancer affecting the lungs, laryngeal, oral cavity, esophagus, pancreas, bladder, renal cell, uterus, ovaries, endometrium, gastric, colon, prostate, liver, brain, and breast as well as acute leukemia had a causal relationship with smoking [2].
A cancer diagnosis can be a powerful motivation for smoking cessation for cancer survivors. However, research shows that 53.4% of domestic cancer survivors and about 50% of cancer survivors in the West continue to smoke after a cancer diagnosis [3,4], increasing the risk of secondary cancer, cardiovascular diseases, and diabetes. It can also reduce the quality of life [5,6]. The proportion of current smokers among known cancer survivors in Korea is 14.5% to 33.5% for males and 2.5% to 4.2% for females and the smoking rate of males is higher than that of females [4,7]. Furthermore, the smoking rate of female cancer survivors was similar to that of the general population. However, the smoking rate of male cancer survivors is lower than that of the general population; nonetheless, this rate needs to be lowered further [4].
Smoking causes a variety of health problems not only in cancer survivors but also in the general population [8]. Moreover, it is emerging as a health problem that is a burden to society [9]. Therefore, World Health Organization enacted the Framework Convention on Tobacco Control (FCTC) in 2005, and Korea is trying to lower the smoking rate through FCTC implementation by adopting price-related tobacco control policies (e.g., increasing the price of cigarettes) and non-price related tobacco control policies (e.g., by expanding smoking cessation areas, organizing tobacco control campaigns, and inserting graphic warnings on cigarette packages) [10,11]. In 2015, the price of cigarettes was raised by 80% and supports extended to bear the cost of smoking cessation medication increased the accessibility of the treatments. Moreover, smoking bans were implemented in all bars, restaurants, and coffee shops to reduce the smoking rate in the general population [12,13]. In 2016, the efforts were continued to lower the smoking rate by including a graphic warning on cigarette packages [14].
This enhanced tobacco control policy will affect current smoking rates and the smoking cessation plans of cancer survivors as well as the general population. Until now, there has been one study on the current smoking rate of cancer survivors for a certain period, but changes in the rate over time have not been studied [4,15,16]. This study investigates the current smoking rate and motivation to quit smoking of Korean male cancer survivors according to changes in tobacco control policies over the last 8 years using the Korea National Health and Nutrition Examination Survey (KNHANES) data from 2010 to 2017.
METHODS
1. Study Population
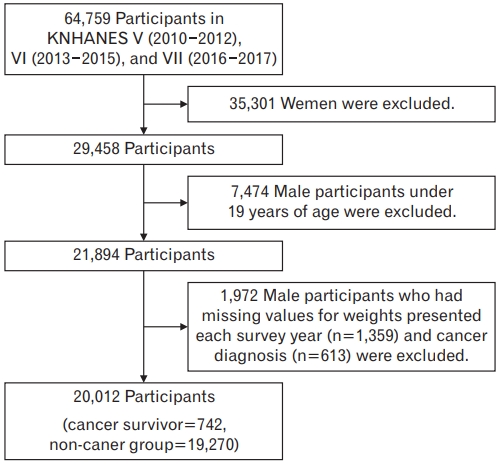
This is a cross-sectional study using the KNHANES for the phases V (2010ŌĆō2012), VI (2013ŌĆō2015), and VII (2016ŌĆō2017) from 2010 to 2017. Of the 64,759 participants of phases V to VII of the KNHANES, 35,301 women and 7,474 male participants under 19 years of age were excluded; the remaining 21,984 male participants aged 19 years and older were included in this study. Furthermore, 1,972 participants who had missing values in the variables applied to the study were excluded, thereby resulting in a final sample size of 20,012. Of these, 742 were cancer survivors (Figure 1). The KNHANES, the data of this study, was conducted with the approval of the Institutional Review Board of the Korea Centers for Disease Control and Prevention, and all participants provided informed consent.
The KNHANES is a nationwide survey conducted annually to assess the health status, health behavior, food intake, and nutritional status of the Korean people. It consists of three surveys: health surveys, including household surveys, health interview surveys, and health behavior surveys; health screening surveys, including physical measurement, blood and urine tests, and oral examination; and nutrition surveys, including assessments of dietary behavior, food intake, and frequency of food intake.
2. Measures
ParticipantsŌĆÖ cancer diagnosis, chronic disease diagnosis, smoking status, drinking status, perceived health status, education level, and income level were surveyed through self-administered questionnaires. A cancer survivor is defined as a person who has concurred to the item ŌĆ£The cancer has been diagnosed by a doctorŌĆØ in the health questionnaire. Types of cancers included in the survey were stomach, liver, colon, breast, cervical, lung, thyroid, and other cancers. Breast and cervical cancers were excluded because the subjects were male. Those individuals who denied any cancer history were defined as belonging to the non-cancer group.
Smoking status was classified into ŌĆ£never smoker,ŌĆØ ŌĆ£former smoker,ŌĆØ and ŌĆ£current smoker.ŌĆØ Individuals who do not smoke or had smoked less than 100 cigarettes during their lifetime were considered nonsmokers. Those who had smoked at least 100 cigarettes but had stopped smoking at present were former smokers. Current smokers were defined as persons who smoke daily or occasionally, and who had smoked at least 100 cigarettes.
The motivation level of current smokers was investigated and classified into three categories according to a transtheoretical model [17]. The health questionnaire asked, ŌĆ£Do you plan to quit smoking in the next month?ŌĆØ Respondents who answered ŌĆ£I plan to quit smoking within 1 month.ŌĆØ were considered to be under the preparation stage; those who answered ŌĆ£I plan to quit smoking within 6 months.ŌĆØ were considered to be under the contemplation stage. Those in the precontemplation stage answered ŌĆ£Not within 6 months, but someday IŌĆÖm going to quit.ŌĆØ or ŌĆ£I do not want to quit at all.ŌĆØ We defined smokers in the preparation and contemplation stages as having a willingness to quit smoking.
The level of education was classified into three categories: lower than middle school, high school, and college and above. The income level was classified into low, mid-low, mid-high, and high by using household income quartiles. The perceived health status was divided into three categories as good, normal, and poor using the question ŌĆ£What do you think about your usual health?ŌĆØ Alcohol consumption was categorized as more than twice a week or less than twice a week. Chronic diseases include high blood pressure, diabetes, dyslipidemia, angina pectoris, and stroke, which can affect smoking cessation. They were considered to have chronic diseases if they had at least one of them.
3. Statistical Analysis
The KNHANES was a multistage stratified cluster data. So, a weight value was presented for each survey year. We integrated the weights for 8-year survey data and applied the integrated weight in our analysis. The continuous variable, age, was expressed as mean and standard error and categorical variables were expressed in percentages and standard errors. Among the sub-categories of these variables, logistic regression analysis was used to calculate the P for trend of the percentage of those with less than middle school education, the lowest family income group, poor perceptions of health, the drinking rate of twice a week, and the chronic disease after adjusting age. The age variable was also analyzed P for trend through linear regression analysis. Logistic regression analysis was used to calculate the P for trend for the current smoking rate and the proportion of those willing to quit smoking among the cancer survivors and non-cancer group. Statistical analysis was performed using the IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
1. General Characteristics of the Study Population
Of the 20,012 men who participated in the study, 742 (3.7%) were cancer survivors and 19,270 (96.3%) were in the non-cancer group. The mean age of cancer survivors was 60.0 years, 61.8 years, and 63.4 years in phases V, VI, and VII, respectively. The mean age increased from phase V to phase VII; however, it was not statistically significant (P for trend=0.053). The mean age of the non-cancer group was 44.0 years, 44.7 years, and 45.5 years in phases V, VI, and VII, respectively. Unlike cancer survivors, the mean age of the non-cancer group increased significantly from phases V to VII (P for trend=0.001). The proportion of cancer survivors having an education level of less than middle school was 67.4%, 70.0%, and 60.1% in phases V, VI, and VII, respectively. Among the non-cancer group, the corresponding percentages were 50.4%, 45.9%, and 41.5% in phases V, VI, and VII, respectively. A decrease in the proportion of those in less than middle school was observed across the phases among the non-cancer group (P for trend <0.001), but not in cancer survivors (P for trend=0.217) (Table 1).
The largest group of cancer survivors belonged to the low-income group in phases V (27.6%) and VI (26.4%), and the mid-low group in phase VII (27.3%). In the non-cancer group, the largest groups were the high-income group in phase VI (33.9%) and phase VII (33.1%), and the mid-high group in phase V (30.7%). Regarding perceived health status, the largest number of participants indicated that their health status was ŌĆ£normalŌĆØ in cancer survivors and the non-cancer group across phases V to VII. Regarding alcohol consumption, the rate of less than twice a week was higher than more than twice a week in cancer survivors and non-cancer group. The proportion of cancer survivors with chronic disease was 35.6%, 42.6%, and 56.5% in phases V, VI, and VII, respectively. In the non-cancer group, the proportion was 19.7%, 22.2%, and 27.9% in phases V, VI, and VII, respectively. The proportion of people with chronic diseases in cancer survivors (P for trend <0.001) and non-cancer group (P for trend <0.001) increased significantly (Table 1).
2. Changes in Prevalence of Smoking and Motivation to Quit Smoking among Cancer Survivors and the Non-Cancer Group
The prevalence of current smokers among cancer survivors was 19.5%, 19.1%, and 15.3% in phases V, VI, and VII, respectively. There were no significant changes across phases V to VII (P for trend=0.33). The proportion of current smokers in the non-cancer group was 46.6%, 41.2%, 38.9% in phases V, VI, and VII, respectively. Furthermore, a significant decrease in the prevalence of current smokers was observed between phases V and VII (P for trend <0.001). In cancer survivors, the percentage of people who were willing to quit smoking was 36.4%, 53.0%, and 34.8% in phases V, VI, and VII, respectively. In the non-cancer group, the percentage of people who were willing to quit was 34.8%, 39.0%, and 34.4% in phases V, VI, and VII, respectively. The percentage of people who were willing to quit smoking did not present a significant trend in cancer survivors (P for trend=0.964) and the non-cancer group (P for trend=0.884) (Table 2).
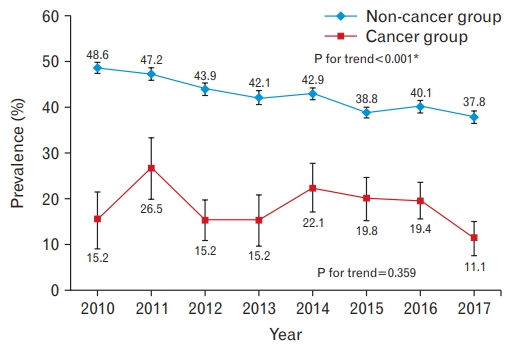
The current smoking rates for cancer survivors by year did not show any significant trends (P for trend=0.359). However, in the non-cancer group, the current smoking rate was higher than the cancer survivors, but the current smoking rate decreased from 2010 to 2017 (P for trend <0.001). Specifically, in 2015, the prevalence of current smokers showed the greatest decrease from 42.9% to 38.8% and a proportion of lower than about 40% was maintained thereafter (Figure 2).
DISCUSSION
In this study, we confirmed the current smoking rates and the changes in motivation to quit smoking of Korean male cancer survivors for the last 8 years from 2010 to 2017 using data from the KNHANES phases V to VII. The proportion of current smokers among male cancer survivors was 15.3% to 19.5% and there was no significant change in this between the phases. However, in the non-cancer group, the proportion of current smokers tended to decrease significantly from 46.6% in the phase V to 38.9% in the phase VII. There were no significant changes in motivation toward quitting among cancer survivors and the non-cancer group within 6 months.
Although the percentage of current smokers in the non-cancer group had declined, a similar trend was not observed among male cancer survivors. There are several reasons for this. First, the current smoking rate of cancer survivors is lower than that of the non-cancer group. This is consistent with those observed in previous domestic and international studies [4,7,18]. In this study, the current smoking rate of male cancer survivors was about half that of the non-cancer group. A cancer diagnosis can be a strong motivation for smoking cessation. According to Westmaas et al. [19], the smoking cessation rate of smokers with a cancer diagnosis was 31.3% within 2 years, which was higher than the 19.5% of smokers who were not diagnosed with cancer in the same period. In another study, the cancer-diagnosed group had a 4.3- fold higher rate of cessation than the non-cancer-group [20]. In other words, cancer diagnosis leads to positive health behaviors. Therefore, the current smoking rate of cancer survivors does not change significantly.
Second, the effects of the ongoing tobacco control policy can be considered. The policy in Korea is gradually being strengthened. For example, beginning with the release of data of the tar and nicotine components in 2002, expanding the non-smoking area in 2003, increasing the price of cigarettes to 2,500 won in 2004, nationwide public health centers providing free smoking cessation counseling services in 2005, increasing the price of cigarettes from 2,500 to 4,500 won, inclusion of smoking cessation treatment under the National Health Insurance cover, enhancing smoke-free legislation at public places in 2015, and inserting graphic warnings on cigarette packages in 2016 [11]. According to the KNHANES, adult men aged 19 years and above are currently showing a decline in smoking trends (66.3% in 1998 to 39.3% in 2015) [10]. Specifically, in 2015, it declined from 43.2% to 39.3%, which is predicted to be the result of three new policies in 2015. The positive effects of these policies on cigarette smoking and health are wellknown [13,14,21-23]. According to a study by Kim and Kim [12], who analyzed the effects of the strengthened tobacco control policies in Korea, the total current smoking rate was decreased by 0.745 times and the current smoking rate of men decreased by 0.69 times after an increase in tobacco prices. In this study, the current smoking rate of the non-cancer group is reduced from 42.9% in 2014 to 38.8% in 2015. This suggests that the tobacco control policy implemented in 2015 had a positive impact on the current smoking rates in the non-cancer group. However, cancer survivors did not show a significant change in current smoking rates, suggesting that tobacco control policies did not significantly affect smoking cessation in this group.
Finally, even if a cancer survivor motivated by these policies has been treated for smoking cessation, the effectiveness of the treatment may be diminished. According to Nayan et al. [24], the effectiveness of short-term or long-term treatments with counseling and smoking cessation medication for cancer survivors was not significantly different from the baseline recommendation. This shows that smoking cessation in cancer survivors is more complex.
There were no significant changes in motivation level within 6 months in cancer survivors and the non-cancer group regarding smoking. According to West and Sohal [25], in a survey conducted on current and former smokers in 1914, 50% attempted to immediately quit smoking without planning, and the success rate of smoking cessation was 2 times higher than planned cessation. In a qualitative study of 35 current or former smokers, most quit smoking for a certain reason rather than through planned quitting [26]. Although the smoking rate of the non-cancer group decreased as a result of trying to quit smoking according to changes in the tobacco control policies in Korea, the results may not be consistent with the motivation level of smokers. Moreover, cancer survivors who had no reduction in smoking rates had a higher rate of motivation level to quit smoking within 6 months compared to the non-cancer group. According to Little et al. [3], several cancer survivors have participated in a cessation treatment program without the willingness to quit smoking. They may have been pressurized by a doctor or compelled by a sense of duty to quit. In this way, the cancer survivors of this study may have shown more willingness to quit smoking than their initial thoughts during the survey.
The limitations of this study are as follows. First, since the KNHANES is a cross-sectional study, it is difficult to clarify the sequence of events between smoking and cancer diagnosis, and there is a difference between the study subjects at the time of the survey. Second, as the questionnaires were self-administered, cancer diagnosis and smoking rates might not have been accurately reported. Despite these limitations, the strengths of this study are as follows. First, we used the KNHANES data which is representative of the country. In fact, the percentage of cancer survivors during the study period was 3.7%, similar to national cancer registration statistics [27]. Second, unlike existing domestic and international studies focusing on factors affecting smoking in cancer survivors, it is meaningful that trends in current smoking rates of Korean male cancer survivors for 8 years could be confirmed for the first time.
In conclusion, there is a need for improvement of the current smoking rate for male cancer survivors and there are no significant changes in the current smoking rates and motivation to quit smoking during the study period. The tobacco control policy had a limited effect on reducing the smoking rate of cancer survivors. A cancer diagnosis motivates smokers to quit smoking. However, since the smoking rate after a cancer diagnosis is high, it can be seen that cessation is difficult. Smoking in cancer survivors increases the risk of secondary cancer development and chronic diseases as well as the recurrence of cancer. Therefore, we should actively promote smoking cessation. Moreover, further research is needed to determine if tobacco control policies can lower smoking rates in cancer survivors.