Cultural Adaption and Psychometric Analysis of Family APGAR Scale in Iranian Older People
Article information

Abstract
Background
Family function is a necessary factor that influences older people’s health. The Family APGAR has been widely used to study family functions. However, there has been no Persian version of this instrument to assess family function in older people. The aim of this study was to determine the psychometric properties of the Persian version of the Family APGAR Scale to evaluate the perception of family functions.
Methods
The “forward-backward” procedure was applied to translate the scale from English into Persian. The translated version was checked in terms of validity and reliability, with a sample of 281 older people selected from retirement centers. The factor structure of the scale was also tested using a confirmatory factor analysis. To test reliability, internal consistency and test–retest analyses were performed.
Results
The results of the confirmatory factor analysis indicated a good structural model. Criterion-related validity was strongly supported by the pattern of association between the APGAR Scale and the social support survey. Cronbach’s α of the scale was 0.88 and test–retest reliability ranged from 0.96 to 0.98, indicating a good range of reliability.
Conclusion
The findings of this study suggest that the Iranian version of the Family APGAR is a valid and reliable scale to evaluate family functions in health intervention programs.
INTRODUCTION
In the recent decade, the proportion of older people worldwide has increased. According to the latest data from the World Health Organization, between 2015 and 2050, the proportion of the elderly is expected to increase from 12% to 22%, meaning there will be an increase from 900 million to 2 billion elderly people aged 60 years [1]. In Iran, the population over the age of 60 will reach approximately 10 million by 2020 and more than 26 million by 2050. According to these statistics, in the current situation, Iran is moving from a young population to a middle-aged population and will soon join the ranks of countries with an aging population [2].
Social support is one of the social determinants of health, which points to the importance of the social dimension of human beings and has been considered in recent years [3]. Accordingly, many studies indicate that establishing social relationships, particularly with family members, will have a significant impact on the mental health of the elderly [4]. In the elderly with less emotional and social support because of social isolation, it is likely to increase mental disorders, particularly depression, misbehavior, occurrence and exacerbation of chronic diseases, reduced quality of life and satisfaction, and inability and disability [5-7]. Family is considered to be primarily responsible for supporting the social and health needs of the elderly. Therefore, recognizing the dynamics of how the family system works is an important part of caring for the elderly. The systematic characteristics of the family refer to functional performance, family’s ability to coordinate or adapt to changes in life, conflict resolution, solidarity among members, success in disciplinary patterns, adherence to boundaries between members, and the implementation of rules and regulations [8]. To evaluate family performance, Smilkstein et al. [9] in 1982 developed a scale called Family APGAR, which stands for adaptation, which includes family resources when help is needed; partnership, which is associated with family communication and problem-solving; growth, which is the family’s access to role change and emotional growth; affection, which includes intimacy and emotional interactions (reciprocal emotional relationships) in the context of the family; and resolve, which is related to decision, determination, will, and effort in the family.
The Family APGAR Scale provides family performance appraisal independent of the family life and has been used in various studies [10-13]. This scale has been widely used in Brazilian public health services, particularly in family health strategy programs, and has been recognized by the Brazilian Ministry of Health as part of the primary care guidelines for assessing the performance of elderly families [14]. This scale is used to diagnose dysfunction in the family system and help perform interventions to balance family relationships.
Studies that provide psychometric analysis of measurement instruments is important, and their reliability and validation are essential for estimating the scientific quality of standardized tools. Because of social and cultural differences in different parts of the population and geographical areas, it is necessary to consider this point before using health-related tools; in other words, it is important to use stable and valid tools that include the desired concept [15]. Thus, only after confirming that a tool has satisfactory psychometric properties in a particular field of application can it be ensured that its use is appropriate. Evidence from the Family APGAR’s validity and reliability results for elderly people living in northeastern Brazil has reported that the use of such tool to assess the performance of elderly families in many cities in the region is appropriate [8].
Similarly, the translation and standardization of this scale has been studied by researchers in Brazil [8], Peru [14], Korea [16], and Taiwan [17]; and based on the results of most studies, this scale is a valid and reliable tool for performance analysis for families in different cultures. However, despite the efforts of researchers, a standard Persian version of this tool was not found. Given the importance of social support, particularly family support, in improving the quality of life of the elderly and the lack of appropriate tools to measure family performance in the elderly, this study was conducted to meet this aim.
METHODS
1. Participants and Study Setting
This study was a descriptive psychometric type. The statistical population of this study included all retired older people in Retirement centers in Qom city, Iran. A total of 300 individuals participated in the study, which used multi-stage cluster sampling, and 281 individuals remained after completing the questionnaires. The inclusion criteria for the study were: at least aged 60 years, living at home, ability to speak Persian, and the absence of a diagnosed psychiatric disorder. The exclusion criterion for the study was incompletion of the questionnaires.
2. Translation and Adaptation
After obtaining permission from the developer, the scale was translated into Persian using the backward-forward method [18]. This method includes translating the original version into the target language by two expert bilingual translators and combining the two versions, measuring the quality of the translation (in terms of clarity, common language usage, conceptual equivalence, and overall quality of the translation) and translating the target version into the original language by two translators. The two versions of the scale (original language and back-translated versions) were then compared for concept equivalence and were approved for final English version by the developer of scale. Subsequently, five psychologists and geriatricians confirmed the validity of the content and cultural compatibility of the scale. To examine the formal validity, the questionnaire was then given to 10 older people who had the criteria to participant in the study, and they were asked to express their opinions about the content, clarity, legibility, simplicity, ease of completing the questionnaire, and ease of comprehension.
3. Instruments
The following instruments were used. The Family APGAR Scale, developed by Smilkstein et al. [9] in 1982, identifies family functions. This scale is an acronym for adaptation, partnership, growth, affection, and resolve. The participants determine their level of disagreement or agreement with each of statement on a 5-point Likert scale, ranging from 1 (never) to 5 (always). All scores were added to obtain the overall score. A high score indicated that the subject enjoyed favorable support from the family [9].
The social support survey is a self-report scale with 19 phrases and five subscales, which include emotional, informational, tangible, affectionate, and positive social interactions [19]. In this scale, the subject determines the degree of disagreement or agreement with each of the statements on a 5-point Likert scale (1=never, 5=always). To obtain the score for each subscore, scores related to the desired scale were added together. All scores were added to obtain the overall score. A high score indicated that the subject had good social support. The validity and reliability of the main scale [19] and the Persian version [20] have been reported to be desirable.
The checklist of demographic information was related to individual characteristics, including age, gender, chronic illness, and marital status.
4. Ethical Considerations
The approval to conduct the study was obtained from the Medical Ethics Committee of Qom University of Medical Sciences (registration no., IR.MUQ.REC.1399.033). For data collection, the study was explained to eligible participants. Informed consent was obtained from the participants before they complete the questionnaire at retirement centers. The purpose of the study and how it was done for the participants were explained.
5. Data Analysis
Smart partial least square (PLS) software ver. 3.0 (SmartPLS GmbH, Oststeinbek, Germany) was used for the data analysis. Descriptive statistics were used to analyze the data. The confirmatory factor analysis method was used to determine the construct validity. In this section, the convergent and divergent validity of the scale were examined. In PLS, factor loads, average extraction variance (AVE), and composite reliability were used to measure convergence validity. For convergent validity, all factor loads must be above 0.6 and significant. The AVE is greater than 0.5, and the composite reliability is greater than the AVE. Divergent validity was measured using the Fornell and Larcker criterion [21], where the squared root of the average variance of each construct should be greater than the correlations from other constructs. In addition, criterion-related validity was performed to demonstrate the extent to which the Family APGAR Scale correlates with scores derived from the social support survey. It was expected that the Family APGAR would positively correlate with this measure. A Pearson correlation coefficient of 0.40 or above was considered satisfactory.
Internal consistency and stability were used to measure the reliability. Cronbach’s α coefficient was used to measure internal consistency. Cronbach’s α was acceptable at >0.7. Scale stability was also assessed using the test–retest method. Twenty-five participants completed the questionnaire in two stages, with a time interval of 2 weeks, and the scores obtained in these two stages were then compared using the intracluster correlation coefficient (ICC). If this index is greater than 0.80, the stability rate is desirable [22].
The goodness-of-fit (GoF) criterion was used to evaluate the fit of the general model. GoF index is the geometric mean of the average communality and average R2 for all endogenous constructs (
RESULTS
The average age of the participants was 65.49 years (standard deviation=5.53). The majority of the participants were men (75.8%), and most of them were illiterate and had an elementary education level (61.9%). In addition, 87.9% of the participants were married, 91.6% were home owners, and 88% lived with a wife and/or children. Table 1 presents further information on the characteristics of the participants.

Demographic characteristics of the study sample (n=300)
According to the results in Table 2, Cronbach’s α coefficients, composite reliability, and AVE were appropriate. The factor loads of the scale in all items were significant and higher than 0.6 (Figure 1).

Convergent validity of the Family APGAR Scale
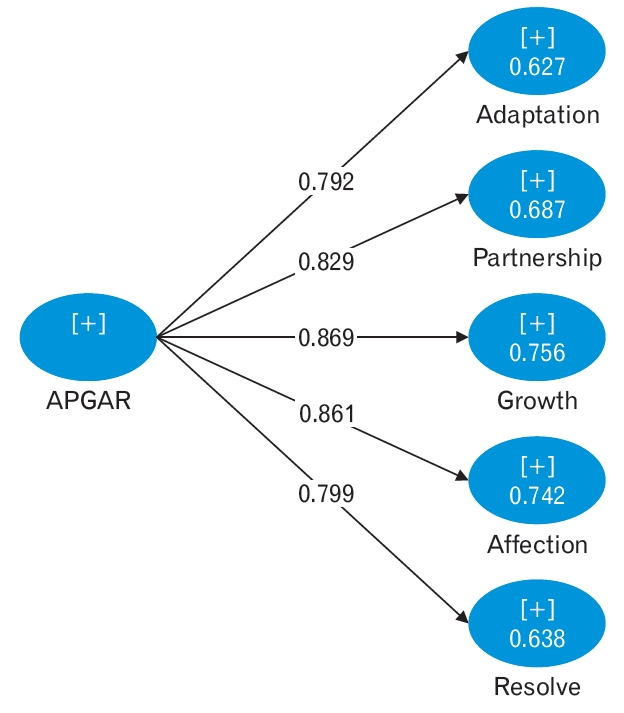
Factor loads of the APGAR Scale in all items. Values are standardized regression weights for items in the APGAR scale.
The results in Table 3 show that the squared root of the average variance exerted by all variables is greater than the correlation value of that variable with other variables. Therefore, the validity of this scale was confirmed.

Divergent validity of the Family APGAR Scale
Criterion-related validity was examined by performing a correlation between the Persian version of the Family APGAR Scale and the social support survey. As expected, a significant positive correlation was observed. The results are presented in Table 4.

Correlation between the social support survey and Family APGAR Scale
The internal consistency of the Family APGAR Scale, as assessed by Cronbach’s α coefficient, showed satisfactory results. Cronbach’s α coefficient for the total scale was 0.887. For the test–retest reliability, the ICC coefficients ranged between 0.96 and 0.98 (P<0.001). The reliability results for the scale are presented in Table 5.

Reliability of the Family APGAR Scale
The GoF index of the study model was 0.69, indicating that the scale had a good fit.
DISCUSSION
To understand how family functions with older people, the use of Family APGAR tools to facilitate health care is a key component of successful intervention health planning, particularly in primary care. The present study was conducted to translate and study the psychometric characteristics of the Family APGAR in Iranian older people.
In this study, confirmatory factor analysis was used to investigate the validity of the construct validity scale. The results confirm the model of factor analysis and indicate its suitability. A study of da Silva et al. [8] in 2014 of construct validity was investigated using exploratory factor analysis, which showed the one-dimensional nature of the Brazilian version of the scale.
To establish the criterion-related validity of the scale, the Family APGAR and social support survey were administered to the participants. There was a significant positive correlation between the social support survey and its subscales, which was consistent with other studies [11,24].
Moreover, the present study showed that the scale had relatively good internal consistency (Cronbach’s α=0.887). The results of a study by da Silva et al. [8] showed a Cronbach’s α of 0.80. Cronbach’s α varied between 0.73 and 0.78 when one item was removed.
The reliability of the scale was also examined using the test–retest analyses, which showed that the results obtained from the two tests at a 2-week interval showed a high stability of the scale.
This study has limitations. First, this study may have led participants to distort their responses to social validation because of the use of self-reporting tools. Another limitation may be that the sample used in this study was unique to Qom city and was available from the sampling method. Therefore, precautions should be taken in generalizing the results.
Overall, the findings of this study suggest that the Family APGAR is desirable in terms of psychometric properties. This tool can be used to measure health outcomes in research and treatment. The application of this scale is easily possible and can be completed by the elderly or health-care providers in less than 10 m.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
This study was financially supported by the University of Medical Sciences.
Acknowledgements
The researchers express their gratitude from participants in this study as well as the deputy of research, Qom University of Medical Sciences to fund and support this project.