INTRODUCTION
Depression is one of the most common and impactful mental illnesses worldwide and is a leading cause of social crises, including substance abuse and suicide. The cost of depression in lost productivity is estimated at $1 trillion annually, according to World Health Organization (WHO) reports [1]. Therefore, prevention and treatment of depression are important. Physical activity is a cost-effective and highly accessible intervention for preventing depression in most adults worldwide [2].
In terms of health benefits, physical activity reduces the prevalence of diseases such as cardiovascular diseases, some cancers, and allcause mortality, as well as that of mental diseases, including anxiety and depressive disorders [3-11]. The WHO has published guidelines for different demographic groups with recommendations for types and intensity levels of physical activity for good health. Physical inactivity increases the risk of poor health [11-13].
Although increased physical activity positively correlates with physical and mental health, it is difficult for individuals to instinctively understand and fulfill the recommended types and amounts of physical activity to meet the guidelines. Many people, including health experts, have suggested that any type of physical activity is beneficial for health. However, some studies have verified that work-related physical activity in other countries and across different age groups is negatively correlated with depressive disorder [14-16].
In Korea, associations between the type of physical activity and the likelihood of depression have not been identified. This study aimed to examine whether work-related physical activity and recreational activity were related differently to the depressive mood in subjects, depending on the intensity of physical activity.
METHODS
1. Participants, Design, and Setting of the Study
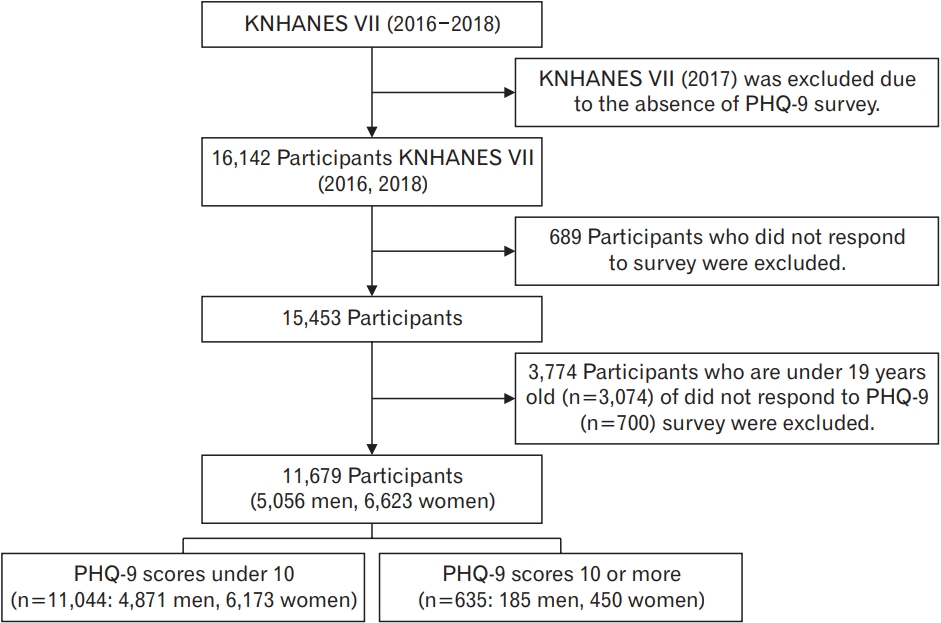
The data for this study were collected during the first and third years (2016, 2018) of the seventh Korea National Health and Nutrition Examination Survey (KNHANES), which was conducted in South Korea by the Korea Centers for Disease Control and Prevention (KCDC). Since the Patient Health Questionnaire-9 (PHQ-9) survey was not conducted in the second year of the KNHANES VII, 2017 was excluded. The KNHANES is a national representative cross-sectional survey designed to provide Koreans with not only subjective information about the general health and nutritional status but also a broad perspective on health risk behaviors and indicators as well as chronic diseases. The initial sample included 16,142 individuals who were invited to participate in the first (2016) and third years (2018) of the seventh KNHANES. The analysis excluded subjects younger than 19 years (n=3,074) and those who provided no information on the PHQ questionnaire (n=700) or any other parts of the survey (n=689). Ultimately, 11,679 participants were eligible for the analysis (5,056 men and 6,623 women) (Figure 1).
The study was approved by the Institutional Review Board on Human Subjects Research and Ethics Committee at Hanyang University Seoul Hospital (IRB approval no., 2021-03-057). The requirement for informed consent from individual patients was omitted because of the retrospective design of this study.
2. Measures of Depression and Physical Activity
The PHQ-9 is a self-administered instrument comprising nine questions to screen for major depressive disorder (MDD), based on the Diagnostic and Statistical Manual of Mental Disorders, fifth edition. Each question was scored from 0 to 3 according to the frequency of symptoms during the 2 weeks preceding the response: 0 (not at all), 1 (several days), 2 (more than half of the days), and 3 (nearly every day). Previous studies have validated a PHQ-9 cut-off score of 10 or higher for detecting MDD, with a sensitivity of 88% and a specificity of 88%. Accordingly, a cut-off score of 10 was used to determine depression in the current study [17-19].
Physical activity was estimated using the Global Physical Activity Questionnaire (GPAQ), which was developed by the WHO for physical activity surveillance. Physical activity was calculated as metabolic equivalent (MET)-min/wk by multiplying the number of minutes of an activity by its intensity: 8 for vigorous activity and 4 for mild or moderate activity. For the purpose of analysis, work-related, leisure, and commuting activities and walking for transport were individually calculated according to the level of intensity and compared to one another. The total activity refers to the sum of each activity reported by the subjects [20].
3. Demographic Characteristics of the Study Population and Variables
Study participants were classified according to their demographic characteristics, socioeconomic background, medical history, and lifestyle. Sex, age, household income, education level, occupation, and marital status were included as socioeconomic factors. Health-related factors included obesity and comorbid conditions such as hypertension, dyslipidemia, stroke, diabetes, myocardial infarction, angina, arthritis, rheumatoid arthritis, asthma, thyroid gland disorder, cancer, chronic renal failure, hepatitis B, hepatitis C, and liver cirrhosis. Obesity was assessed by body mass index, and weight status was divided into three groups: underweight (<18.5 kg/m2), normal weight (18.5– 24.9 kg/m2), or obese (≥25 kg/m2). Lifestyle habits include current smoking status and alcohol consumption. Current smoking status was a dichotomous variable reported as current smokers and previous smokers who had quit smoking or who had never smoked. Alcohol use was classified as those who consumed alcohol or those who had never consumed alcohol.
4. Statistical Analysis
To reflect the stratified cluster and systematic sampling of the KNHANES, we applied weight sampling to consider the complex sampling method. General characteristics were evaluated using the chisquared test. Associations between the types of physical activity and depression were compared using independent complex-sample ttests. A multiple logistic regression analysis was conducted to determine whether each type of activity was related to depressive symptoms. All statistical analyses were performed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Table 1 shows the general characteristics of the study population. Of the 11,679 participants, 5,056 men and 6,623 women, 185 men (3.66%) and 450 women (6.79%) were diagnosed with depression according to the PHQ-9. The distributions of sex, household income, education level, occupation, marital status, obesity, smoking status, alcohol use, and comorbid conditions were significantly different between the two groups of participants with and without depression.
Table 2 shows the comparative amount of physical activity according to depression. The amount of total work-related activity was significantly higher in participants with depression than in those without depression (386.7 versus 206.7, P=0.01). Participants in the depression group were less likely to engage in recreational physical activity than those without depression (143.7 versus 316.3, P<0.001). The MET values for walking and transport-based activities were not significantly different between the two groups (Table 2). According to the intensity of work-related physical activity, there were significant differences in moderate work-related physical activity between the two groups, with MET values being greater in participants with depression (290.1 versus 140.2, P=0.01). The analysis also revealed greater amounts of vigorous work-related physical activity in the depression group; however, the difference was not significant (66.5 versus 96.7) (Table 2). Regarding intensity levels of recreational physical activity, recreational activities conducted with both vigorous and moderate intensity levels were significantly more frequent in participants without depression (153.2 versus 56.2, P<0.001 for vigorous intensity and 163.1 versus 87.5, P<0.001 for moderate intensity) (Table 2).
Table 3 shows the results of the multivariate logistic regression analysis of the relationship between physical activity and depression. With an increase of 100 MET-min/wk in work-related physical activity, the odds ratio (OR) for depression in participants was 1.01 (95% confidence interval [CI], 1.005–1.015) after adjustment for age, sex, obesity, smoking status, alcohol use, income, education, marital status, occupation, and comorbid conditions. On the other hand, participants were less likely to have depression with greater amounts of recreational physical activity (OR, 0.96; 95% CI, 0.64–0.99). Regarding the associations between work-related activity, recreational physical activity, and depression, similar findings were noted after further adjustment for other types of physical activity, in addition to the variables adjusted in model I. There was no significant association between walking-or transport-related physical activity and depression.
DISCUSSION
Our study demonstrated that work-related physical activity and recreational activity were related differently to depression in subjects depending on the intensity of physical activity. Work-related physical activity was associated with an increase in the ORs of depression by PHQ scoring, and both vigorous- and moderate-intensity recreational physical activity lowered the ORs of depression. The relationship remained significant after further adjustment for different types of physical activity. On the other hand, walking or commuting physical activity was not significantly associated with depression.
This study is the first to consider the differences between types of physical activity associated with mental health in Korean adults. Physical activity allows individuals to maintain healthy bodies and provides a foundation for sound mental health. Increased levels of physical activity and exercise are known to improve mental health and prevent depression in various populations [15,21-28]. Numerous studies have demonstrated that physical activity decreases stress by impacting hormone levels [27,29] and improves anxiety and depression [15,28]. However, these previous studies have been limited to specific groups, such as older adults [15] or college students [23], and/or have not distinguished between types of physical activity to examine their varying effects on mental health.
An analysis of the relationship between general characteristics and depression is shown in Table 1. Consistent with the findings of previous studies, low household income, low education level, and unemployment status were more strongly related to the prevalence of depression [30].
Using a cross-sectional design, we found that work-related physical activity is negatively related to mood. This finding is consistent with research indicating that greater amounts of moderate work-related activity correlate with a higher prevalence of depression [15]. The MET values of work-related activity and recreational activity were inversely related to the prevalence of depression. According to the PHQ-9, total work-related activity was higher by 180 MET-min/wk in subjects with depressive disorders. On the other hand, total recreational activity was lower by 162.95 MET-min/wk in those with depression. These results suggest that work-related physical activity does not positively affect depressive mental status. Work-related physical activity was highest in those with lower levels of education, which could imply that these subjects have more labor-intensive work than the work done by others [15]. After adjusting for other covariates, including education and income status, every 100-unit increase in total work-related activity induced the prevalence of depression by 1.010 times (95% CI, 1.005– 1.015; P<0.001). This finding indicates that work-related activity itself could be associated with the aggravation of depression regardless of socioeconomic status. Other types of physical activity did not interfere with the effects of work-related or recreational activity, which presented identical trends in ORs corresponding to a 100-unit increase in work-related physical activity (OR, 1.012; 95% CI, 1.006–1.017) and recreational physical activity (OR, 0.962; 95% CI, 0.937–0.987). Total work-related activity and moderate work-related activity were significantly related to depression, whereas vigorous work-related activity was not statistically significant. This finding is consistent with the results of previous studies on older adults [15].
Our study has some limitations. The mechanism by which work-related physical activity affects depressive mood was not identified in this study. In multivariate linear regression analysis, Vigorous work-related physical activity was not significantly related to the prevalence of depression. The ORs of work-related physical activity demonstrated that any intensity level of work-related activity could contribute to depressive mood. However, moderate work-related physical activity was more highly associated with depression than vigorous work-related physical activity (vigorous work: OR, 1.005; 95% CI, 1.001–1.009; moderate work: OR, 1.008; 95% CI, 1.004–1.013). This result might be due to the small sample size and the small amount of vigorous work-related activity analyzed. Accordingly, the reasons for the lack of a positive correlation between the intensity of work-related activities and depression should be investigated.
Another limitation of this study is its cross-sectional design, which could not establish causal relationships between physical activity and depressive moods. We could not confirm a causal relationship between physical activity and the prevalence of depression among the participants. These two phenomena might affect each other reciprocally, with depressive people performing less recreational activity, causing them to be more depressed; greater work-related activity induces stress, leading to greater depressive mood; and depressive people experiencing more work-related physical activity. In addition, in observing only a certain moment in time, this study should not be used to analyze the effectiveness of physical activity on depression over a period of time or to establish long-term trends. As self-administered tools, the PHQ-9 and GPAQ might have high rates of “false negatives” or “false positives.”
Regardless of intensity level, recreational activity was positively associated with an improvement in depressive mood. Accordingly, any kind of recreational physical activity is recommended to provide mental health benefits. In contrast, work-related physical activity should not aggravate mental health.
In conclusion, this study is the first to show that different types of physical activity can be differentially associated with depressive mood disorders in Korean adults. This study provides guidance for reducing work-related physical activity and increasing recreational physical activity to improve mental health and prevent depression. Health-enhancing leisure-time physical activity interventions may be needed for individuals with depressive moods to generate benefits for mental health. However, further research is required to determine the causal effect of various types of physical activity on clinical depression in a prospective manner or to establish the intervention effects of physical activity to improve depressive mood in specific populations.