INTRODUCTION
Adolescence, a pivotal stage in development, is characterized by marked physiological, social, and reproductive maturation. Changes during adolescence affect future health and health-related behaviors, raising concerns about their long-term impact on the health and well-being [1,2]. Metabolic disorders that manifest during childhood and adolescence pose increased risk of progressing to metabolic syndrome (MS), diabetes, and cardiovascular diseases (CVDs), which place considerable burden on global healthcare systems [3].
Promoting adequate physical activity (PA) is one of the most sustainable and beneficial approaches for combating metabolic disease [4]. Aerobic exercise (AE) is frequently recommended for obese individuals and offers benefits in terms of body composition, lipid profile, blood pressure (BP) control, glycemic control, and cardiorespiratory fitness [5]. Resistance training not only increases the muscle mass and strength, but also improves cardiovascular risk factors, like AE [6,7]. Several studies have shown that combining aerobic and resistance exercises (RE) has a more pronounced effect on reducing fat mass and weight while providing additional cardiovascular benefits than either AE or RE alone [8,9]. Although numerous studies have highlighted the advantages of PA, there is limited evidence regarding the most effective type of exercise for preventing metabolic complications, particularly in adolescents.
Our study aimed to evaluate and compare the benefits of AE and RE in reducing cardiovascular risk factors among adolescents using a representative sample of the general Korean population.
METHODS
1. Study Population
In this study, we analyzed pooled data (2019–2021) from the 8th Korea National Health and Nutrition Examination Survey (KNHANES). The KNHANES is conducted by the Korean Ministry of Health and Welfare, and targets non-institutionalized Korean citizens residing in Korea following a multi-stage clustered probability design sampling plan. The survey questions were prepared by the Korea Institute for Health and Social Affairs and the Korea Centers for Disease Control (KCDC; currently, Korea Disease Control and Prevention Agency), and approved by the ethics committee of the KCDC. Detailed information on KNHANES is available at https://knhanes.cdc.go.kr/knhanes/eng.
This study was performed in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of the Severance Hospital, Seoul, South Korea (IRB approval no.: 4-2023-0877).
The study participants were Korean adolescents aged 12–18 years. Data pertaining to 1,431 adolescent participants were collected in the form of a health interview. Those with missing exercise questionnaires (n=114) and laboratory data (n=95) were excluded, and 1,222 eligible participants were included in the final analysis (Figure 1).
2. PA Questions and Classification of Aerobic Activity and Anaerobic Activity
1) Contents of PA questionnaire
The international PA questionnaire was used to assess the participants’ PA levels over a typical week. The questionnaire asked the participants to report days (and durations) on which they engaged in mild (involving walking for at least 10 minutes, encompassing activities at work, school, transportation, and exercise), moderate (activities such as double tennis or volleyball that increased heart rate or breathing for at least 10 minutes), or intense (vigorous activities, such as running or soccer, for at least 10 minutes) PA.
Participants noted the number of days and total duration of each activity (minimum of 10 minutes). The KNHANES categorizes PA into four types: (1) intense PA (resulting in breathlessness for >10 minutes); (2) medium-intensity PA (activities causing harder breathing or slightly shorter breaths for >10 minutes); (3) RE (including push-ups, situps, weights, and similar activities); and (4) exclusive walking exercise (comprising commuting and exercise). Each participant could belong to multiple exercise categories.
2) Classification of aerobic activity and anaerobic activity
The World Health Organization (WHO) recommends that children and adolescents (aged 5–17 years) should engage in at least 60 minutes per day of moderate-to-vigorous intensity, mostly aerobic, PA across the week. They should also include vigorous-intensity aerobic and muscle- and bone-strengthening activities for at least 3 days per week. Therefore, reducing sedentary time, primarily recreational screen time, is encouraged [10]. For PA measurements, the metabolic equivalent of task (MET) for moderate and vigorous aerobic activities are approximately 4 and 8, respectively. Based on the WHO recommendation of 60 minutes of daily aerobic activity, adolescents were categorized into AE group if they achieved a total of 600 MET×min/wk or more. Adolescents who engaged in strength training for more than 3 days in the previous week were categorized into RE group.
3. Covariates
Household income levels were categorized as low, medium-low, medium-high, or high. Educational level was classified as elementary, middle, or high school.
Body mass index (BMI) (kg/m2) was calculated as weight in kilograms divided by height in meters squared. Height was measured to the first decimal place (0.1 cm) using a stadiometer (SECA 225 in 2016–June 2019 and SECA 274 in July 2019–2020; Seca, Hamburg, Germany). Weight was accurately measured to the nearest 10 kilogram using an electronic balance (GL-6000–20; Gtech, Seoul, Korea). Waist circumference (WC) was measured at the midpoint between the lower margin of the rib cage and the upper margin of the iliac crest. BP was measured in a seated position (after a rest period of 5 minutes) in the right arm using a standard mercury sphygmomanometer (Baumanometer Wall Unit 33 [0850] in 2016–2019; W. A. Baum, Copiague, NY, USA and Greenlight 300 in 2020; Accoson, Irvine, UK).
The participants were categorized into four groups based on their BMI percentiles, according to the 2017 Korean national growth charts, as follows: underweight (below the 5th percentile), normal (5th to <85th percentile), overweight (85th to <95th percentile), and obese (≥95th percentile).
For laboratory assessments, all participants fasted for at least 8 hours prior to blood sampling. Blood samples were collected by trained medical personnel. Laboratory measurements included serum fasting glucose, total cholesterol, triglyceride, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), aspartate aminotransferase (AST), and alanine aminotransferase (ALT) levels measured using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). White blood cell (WBC) counts were measured using a laser flow cytometer (XN-9000; Sysmex, Tokyo, Japan).
Fasting insulin levels were assessed using an electrochemiluminescence immunoassay (Roche, Basel, Switzerland) and evaluated with a modular E801 analyzer (Roche). Insulin resistance was evaluated using the HOMA-IR (HOMA-IR=fasting insulin [μU/mL]×fasting glucose [mg/dL]/405) and TyG (TyG index=ln[triglyceride (mg/dL)×glucose (mg/dL)/2]) indices.
MS was defined using the criteria adapted from the National Cholesterol Education Program-Adult Treatment Panel III. According to the definition, MS required the presence of any three out of the five specified criteria: (1) WC ≥90th percentile for age and sex; (2) TG ≥110 mg/dL; (3) HDL-C ≤40 mg/dL; (4) systolic blood pressure (SBP) or diastolic blood pressure (DBP) ≥90th percentile for age, sex, and height; and (5) fasting glucose ≥110 mg/dL [11]. The reference values for WC and BP were based on the growth charts issued by the Korean Pediatric Society.
4. Statistical Analysis
Prior to matching, data are presented as means±standard error or as prevalence (%). Sampling weights were used to account for the complex sampling. The characteristics of the exercise groups were compared using analysis of variance or Student t-test for continuous data and Pearson’s chi-square test. Multivariate regressions were performed to compare the PA groups associated with metabolic risk factors after adjusting for age, sex, educational, and household income status. The results are presented as coefficients and 95% confidence intervals (CI). MS-dependent variables were modeled using multiple logistic regression, and the results are reported as odds ratios (ORs) and 95% CI.
Sensitivity analyses were conducted using propensity score matching (PSM) to verify the robustness of our findings regarding the effects of PA on metabolic risk factors. We performed 1:1:1:1 PSM to mitigate the confounding effects of age and sex using the nearest-neighbor matching algorithm. Propensity score was defined as the probability of treatment assignment conditioned on the observed covariate [12]. Standardized mean differences (SMD) were calculated to evaluate the balance of covariates before and after propensity score implementation. An SMD <0.1 was considered the balanced distribution of data.
Statistical significance was set at two-sided P<0.05. All statistical analyses were conducted using R software ver. 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/).
RESULTS
The clinical characteristics of the participants are summarized in Table 1. Of the 1,222 participants, 662 (56.2%) were boys and 560 (45.8%) were girls. The mean age and BMI of the participants were 15.08 years and 22.05 kg/m2, respectively. When divided into four groups according to their PA status prior to matching, majority of the participants were in the no exercise (NE) group (865, 70.7%), followed by RE-only (141, 11.54%), AE-only (120, 9.82%), and CE groups (96, 7.86%). Among the four groups, there were significant differences in age, sex, educational status, BMI, triglyceride level, glucose level, TyG index, and AST level.
Following 1:1:1:1 PSM, 276 adolescents were matched based on their PA status for the sensitivity analysis. Differences in demographic, anthropometric, and metabolic risk factors, including glucose and lipid parameters, were analyzed in the 69 matched quadruplets (Table 1). No significant differences were noted among the four matched groups, except for fasting glucose levels.
1. Comparison of Metabolic Parameters between the Four PA Groups
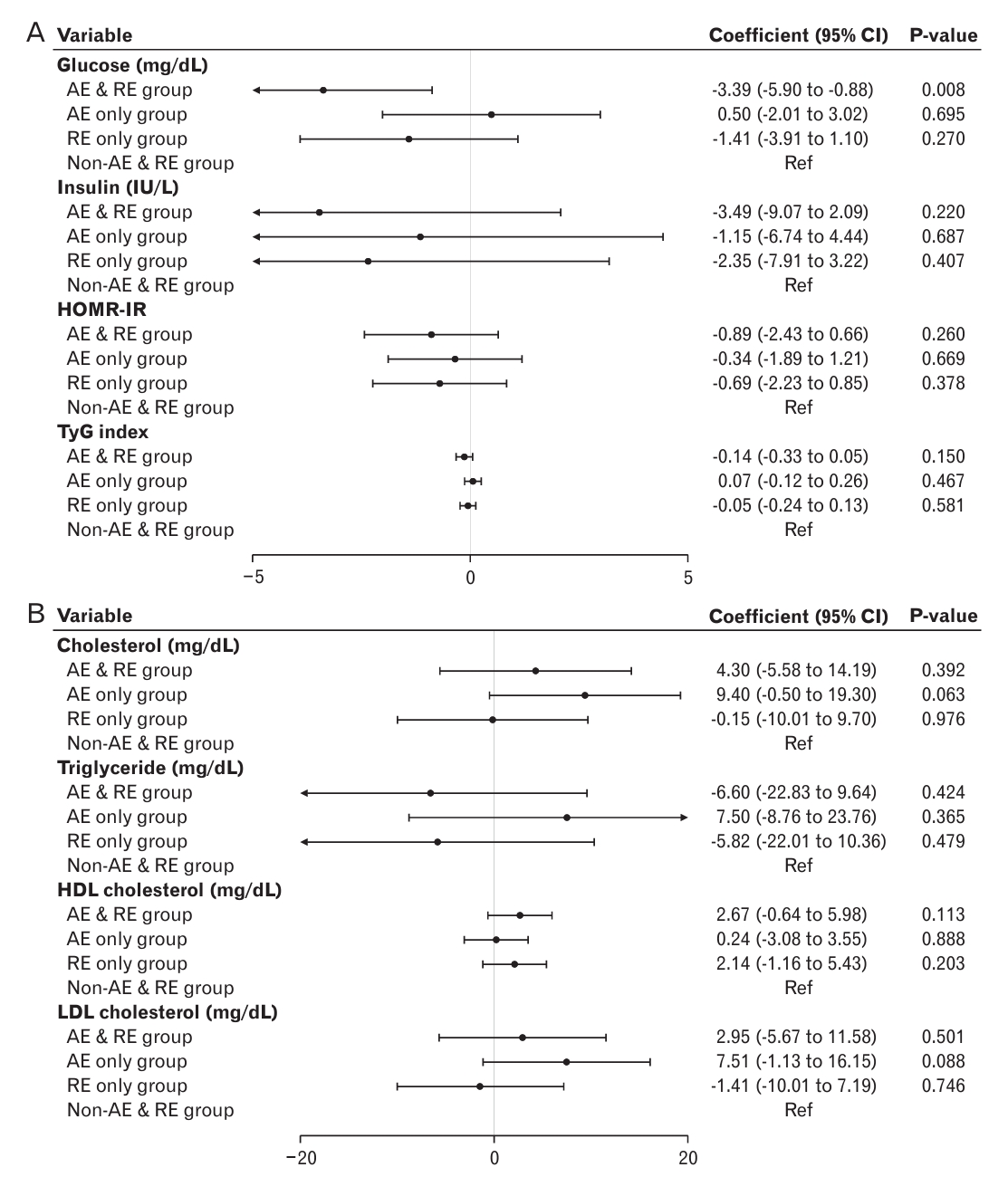
Table 2 and Figure 1 show the regression coefficients of anthropometric and metabolic parameters among the four PA groups. Fasting glucose, TyG index, and WBC count were lower, whereas HDL-C levels were higher in the AE and RE groups compared with that in the NE group. The RE-only group showed decreased values of mean BP, triglycerides, fasting insulin, HOMA-IR, and TyG index; however, it showed increased HDL-C levels compared to the NE group. Total cholesterol and HDL-C levels were significantly higher in the AE-only group compared with that in the NE group. Compared with the NE group, the OR of MS in the RE-only group was significantly lower (OR, 0.228; 95% CI, 0.069–0.756; P=0.016).
The forest plot depicts a comparison of metabolic parameters and cardiovascular risk factors among the four PA groups (Figure 2).
After PSM, when anthropometric and metabolic risks of the CE group were compared with that of the NE group, the results showed a trend similar to that before matching. However, the glucose levels were significantly lower in the CE group than that in the NE group after adjusting for age, sex, educational status, and household income (Appendix 1).
2. Comparison of Metabolic Parameters between AE- and RE-only groups
We performed a subgroup analysis to investigate differences in metabolic risk between the AE- and RE-only groups. Prior to and after the 1:1 PSM, the RE group had lower total and LDL-C levels than the AE group (Table 3).
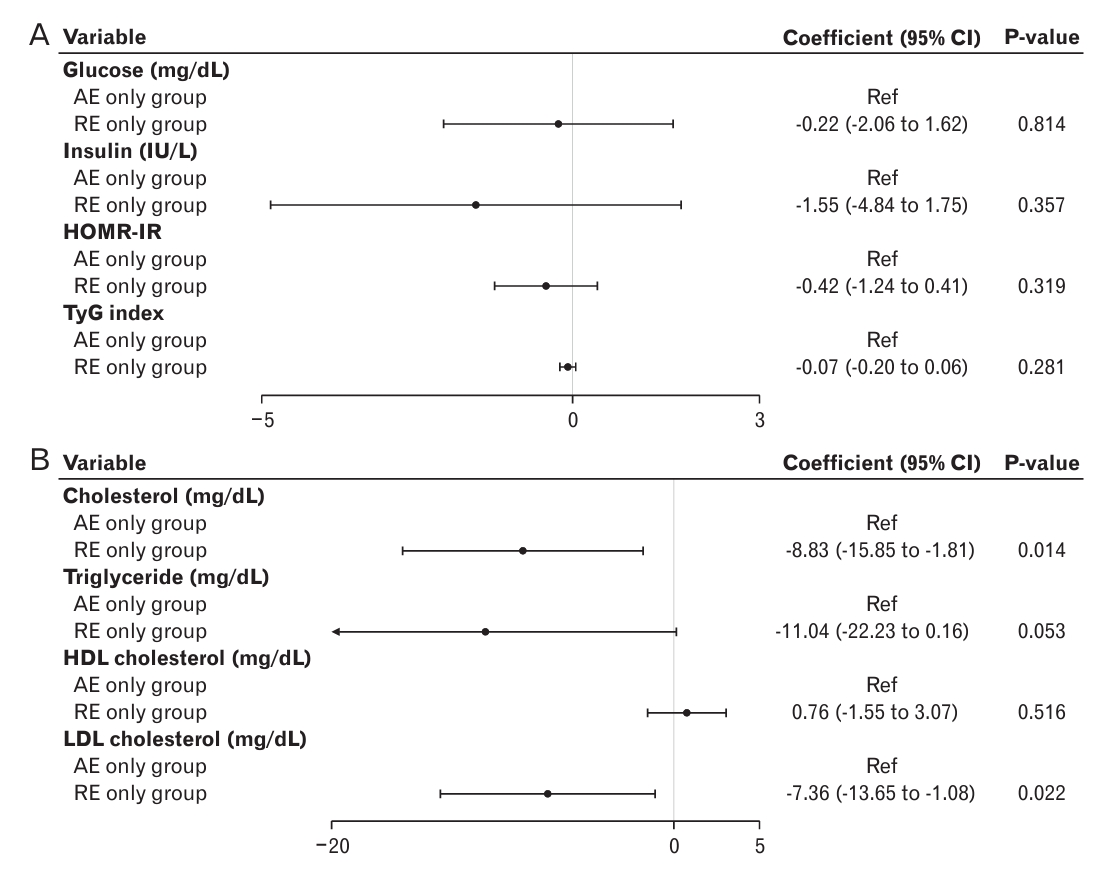
Table 4 and Figure 3 show the correlation coefficients of the anthropometries and metabolic indices, and the OR of MS in the RE-only group, with the AE group set as a reference prior to matching. Compared to the AE-only group, the RE-only group showed significantly lower mean BP (-2.041; 95% CI, -3.957 to -0.125; P=0.037), total cholesterol (-8.881; 95% CI, -15.855 to -1.807; P=0.014), and LDL-C levels (0.762; 95% CI, -13.646 to -1.081; P=0.014).
After PSM, the comparison of glucose and lipid metabolism parameters between the RE- and NE-only groups showed similar trends to those prior to matching (Appendix 2, Figure 3). In addition, compared to the AE-only group, the RE-only group showed a significantly lower TyG index (-1.158; 95% CI, -0.313 to -0.002; P=0.046) after matching (Figure 3).
DISCUSSION
Despite various guidelines endorsing PA for adolescents, the type of exercise that is most effective in reducing cardiovascular risk in this age group remains unclear. Comparing the benefits of each exercise modality can lead to better exercise recommendations for adolescents with or at risk for MS.
Comparison of metabolic parameters in the CE and NE groups revealed that the CE group exhibited lower fasting glucose, TyG index, and WBC count but higher levels of HDL-C. The RE-only group showed reduced mean BP, triglycerides, fasting insulin, and insulin resistance indices (HOMA-IR and TyG), along with increased HDL-C compared to the NE group. Additionally, the RE-only group had significantly lower odds of developing MS than the NE group. In contrast, the AE-only group showed higher total cholesterol and HDL-C levels. In a detailed comparison of the AE and RE groups, the RE group consistently exhibited favorable metabolic parameters, including lower BP and total and LDL-C levels, which persisted even after PSM.
The WHO recommends 60 minutes of moderate-to-high-intensity PA for children and adolescents, including muscle-strengthening exercises for at least 3 days per week [13]. However, our study found that over 70% of Korean adolescents did not meet this minimum recommended PA level, with only 40% incorporating resistance training, and their compliance with these standards trailing significantly behind those of other nations [14,15]. Given these results, it is essential to create a plan that enables students to engage in PA at school, home, and while commuting. Strength training and increased exercise volumes can enhance the overall metabolic health of adolescents.
Given the lasting impact of the CVD risk from youth to adulthood [16], it is essential to highlight that healthy lifestyle habits that develop through daily PA during adolescence often persist into adulthood [17]. Robust evidence suggests that a sedentary lifestyle contributes to the pathogenesis of MS [18,19]. In contrast, PA not only enhances physical fitness but also has a positive impact on cardiometabolic health in the youth, as confirmed by previous studies [20,21].
PA enhances insulin sensitivity by addressing critical factors in the pathophysiology of insulin resistance, such as adiposity, inflammation, and disrupted glucose metabolism [22]. In addition, it positively affects plasma lipids, particularly triglycerides and HDL-C [23]. Moreover, PA of any intensity is linked to lower BP, suggesting its value in improving the metabolic health of adolescents [16]. However, limited and inconsistent data are available on the comparative effects of AE and RE on cardiovascular and metabolic parameters in adolescents.
AE notably enhanced cardiorespiratory fitness, whereas RE and CE improved muscular strength and endurance more effectively than the control conditions or AE-alone in adolescents [7]. Although there is limited information on the impact of RE on cardiovascular health compared to that of AE, our findings indicate that RE outperforms AE-alone in reducing lipid parameters and the TyG insulin resistance index, even after adjusting for demographic covariates. The HEARTY trial (healthy eating, aerobic and resistance training in youth trial) reported that insulin resistance tended to persist in young individuals transitioning into puberty and increased their cardiometabolic risk in adulthood along with early onset of dyslipidemia in childhood and adolescence [24], and showed that effective management of insulin resistance and lipid profile through RE in adolescents may reduce the risk of premature CVD [25].
Our study had several limitations. First, the cross-sectional design did not establish causality. Especially in adolescents, the type of exercise may be influenced by external factors, such as parental guidance, and other variables such as obesity, socioeconomic status, and age. To compensate for this limitation, we used PSM, which successfully reduces the bias between groups. Second, there are inconsistencies between the results of previous studies and ours. Several studies have revealed that AE and CE are superior to RE [8,26-28]. The precise reasons for the inconsistent results remain to be elucidated and are possibly influenced by factors such as racial disparities, sample sizes, and variations in exercise type and strength. Therefore, further extensive prospective cohort studies with larger population and meticulously designed clinical trials are warranted to establish the optimal exercise regimen for adolescents. Third, there were substantial discrepancies in demographic characteristics, such as sex and BMI, prior to matching. Consequently, a limitation arose regarding the reduced availability of matching data with similar characteristics: the proportion of female adolescents was lower than male adolescents. However, PSM remains a valuable method for reducing baseline group differences, particularly when randomized controlled trials are not feasible. Fourth, our study did not consider essential dietary factors among the various lifestyle factors that can influence the cardiovascular risk. Finally, we relied on self-reported questionnaires to evaluate PA, potentially weakening the connection between AE and RE, and their impact on glucose and lipid parameters.
Despite these limitations, this study has several strengths. To the best of our knowledge, this is the first study to identify a positive association between RE and metabolic indices compared with AE in adolescents. Additionally, we conducted a sensitivity analysis using a 1:1 PSM approach, using a well-known database that accurately represents the Korean population.
The findings of this study provide valuable insight into the positive effects of PA on cardiovascular risk factors in adolescents. In addition, our study suggests that RE may be superior to AE in improving metabolic risk factors in adolescents. Further studies are warranted to confirm the relative benefits of exercise, based on the type of exercise.