INTRODUCTION
Osteoporosis is a systemic disease entailing low bone density and dysfunctional bone tissue, resulting in an increase in skeletal vulnerability and fracture risk [1]. As the population of the elderly increases, the incidence of osteoporosis and osteoporotic fracture increases. According to a study on osteoporosis in the Korean population, osteoporotic femoral neck fractures and accompanying mortality have increased recently [2]. Osteoporosis and its resulting fractures not only cause social and economic losses, but also have huge impact on patientsŌĆÖ family members and society. Therefore, the prevention of osteoporosis is needed to reduce the morbidity and economic burden of this disease [2,3].
Since bones continuously undergo a process of remodeling, the formation of new bone requires an adequate supply of amino acids and mineral substrates. Protein has been reported to be beneficial as well as harmful to bone health depending on a variety of factors, including mode of intake, source, calcium intake, demographic factors such as, age and sex, body weight, and/or acid-base balance of the diet [4]. Many studies have reported that as protein intake decreases, bone mineral density (BMD) decreases, and that the intake of both animal and plant protein is important for maintaining BMD [5,6]. However, whether animal protein intake levels are proportional to BMD, and which protein source is more beneficial for maintaining bone density and reducing fracture risk, are controversial issues [7]. Further research exploring the association between intake of animal protein and incident osteoporosis is required.
According to data from the Korea National Health and Nutrition Examination Survey from 2010 to 2019, the proportion of people who consumed less protein than the estimated average requirement (0.73 g/kg/d) increased by 6% from 21.7% in 2010 to 27.0% in 2019, reaching 34.5% for men and 44.7% for women aged 65 years and older [8]. Therefore, it is important in the clinical field to emphasize the importance of protein intake and recommend strategies of consuming sufficient quantities of it.
Meat is the main valuable source of animal protein with a balanced composition of essential amino acids and various nutrients. Processed meat is generally defined as products made from salted or smoked red meat to improve the durability and color and taste of the food [9]. Processed meat is widely consumed because it is easy to obtain and inexpensive.
This study aimed to investigate the relationship between the intake of processed meat and incident osteoporosis in community-dwelling adults aged 50 years and over, using data from the Korean Genome and Epidemiology Study (KoGES).
METHODS
1. Study Population
We used data from the KoGES_Ansung study, a longitudinal prospective cohort study conducted by the Korea Centers for Disease Control and Prevention (KCDC) to investigate the genetic and environmental factors contributing to common chronic diseases in Koreans and the causes of mortality with a long term follow-up period [10]. This cohort study included 5,018 participants aged 40ŌĆō69 years living in a rural area (Ansung) and a follow-up was conducted biennially from 2001ŌĆō2002 (baseline survey) to 2019ŌĆō2020 (ninth follow-up). We used data from the second to the ninth follow-up periods.
Among the 3,975 participants studied at the second follow-up, we excluded 295 who had previously been diagnosed with osteoporosis. Of the remaining participants, we excluded 324 who did not participate in the follow-up after the baseline study. Next, we applied the following exclusion criteria: (1) adults under the age of 50 years (n=736); (2) implausible daily total caloric intake of less than 1,000 kcal/d or more than 10,000 kcal/d (n=106); and (3) daily total protein intake of less than 45 g/d (n=1,254). After these exclusions, 1,260 participants (764 men and 496 women) were included in the final analysis. Participants were asked to complete questionnaires through letters, telephone calls, on-site invitations, and community conferences.
The study protocol was approved by the Institutional Review Board of the KCDC. The KoGES_Ansung study protocol was reviewed and approved by the institutional review board (IRB) of the Korea Centers for Disease Control and Prevention. Written informed consent was obtained from all participants. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. This study was approved by the IRB of Seoul Medical Center (IRB no., 2023-02-009).
2. Data Collection
A validated semi-quantitative 106-food item food frequency questionnaire (SQFFQ) was used to measure the processed meat intake [11]. The questionnaire evaluated how much each participant consumed in a single sitting (three Vienna sausages and one half slice of ham, five Vienna sausages and one slice of ham, or eight Vienna sausages and one and a half slices of ham) and how often they consumed each food item (never or almost never, once a month, 2ŌĆō3 times per month, 1ŌĆō2 times per week, 3ŌĆō4 times per week, 5ŌĆō6 times per week, once a day, twice per day, or twice times per day). Sausage and ham were defined as the processed meat. The daily intake (g/d) of sausage and ham was calculated based on the standard serving size (sausage: 10 g, ham: 20 g). We divided the cohort into two groups by the amount of their processed meat intake at baseline. The barely ingested group had never or rarely ingested processed meat, and the ingested group had ingested processed meat more than once a month.
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured thrice times in the right upper arm using a standard mercury sphygmomanometer (Baumanometer; Baum, Copiague, NY, USA). The average of the second and third blood pressure measurements was used for calculating the mean blood pressure as follows: (SBP+2DBP)/3. Income was divided into three groups as follows: (<1 million won, 1ŌĆō3 million won, and >3 million won per month).
3. Covariates
All the participants completed a SSFFQ and self-reported questionnaire that included questions regarding sociodemographic information, medical history, and alcohol consumption status and were accordingly classified as current drinkers or nondrinkers. Smoking status was also assessed, and participants were categorized as current smokers or nonsmokers.
We assessed physical activity using a metabolic equivalent of task (MET)-hours per week (METs-h/wk). MET was obtained from the participantŌĆÖs report on hours spent on sleep and five types of physical activities according to intensity (sedentary, very light, light, moderate, and heavy). Based on the International Physical Activity Questionnaire [12], the activities were assigned the points as follows: sedentary: 0 MET; very light: 1 MET; light: 3 MET; moderate: 5 MET; heavy: 8 MET. We calculated the total METs-h/wk [13].
BMD was measured by Quantitative Ultrasound (QUS) (Omnisense 7000s; Sunlight Medical Ltd., Petah Tivka, Israel), which measures the speed of sound in meters per second (m/s) in the distal radius. Measurements were performed thrice, and the average of the values was used in this study. QUS results are expressed as absolute values and T-scores [14].
4. Statistical Analysis
Continuous variables are presented as means with standard deviation, and categorical variables are presented as frequencies with percentages. The baseline characteristics of the study populations of each group were compared employing the t-test for continuous variables and chi-square test for categorical variables. Kaplan-Meier curves of the results of the log-rank test were plotted to compare the cumulative incidence of osteoporosis between the groups.
The barely ingested group was set as the reference group and the hazard ratios (HRs) with a 95% confidence interval (CI) for incident osteoporosis were calculated using multivariate Cox proportional hazards regression models after adjusting for potentially confounding variables. All statistical analyses were performed using IBM SPSS ver. 22.0 software (IBM Corp., Armonk, NY, USA). P-values of <0.05 were considered statistically significant for all analyses.
RESULTS
1. Participant Characteristics
Of the 1,260 participants, 1,034 were in the barely ingested group, and 226 were in the ingested group. Age and the proportion of low-income participants were higher in the barely ingested group, and the proportion of middle-high income participants; daily calcium (Ca), protein, and coffee intake; muscle mass; and total caloric intake were higher in the ingested group at baseline (Table 1).
2. Longitudinal Relationship between Osteoporosis and Processed Meat Intake
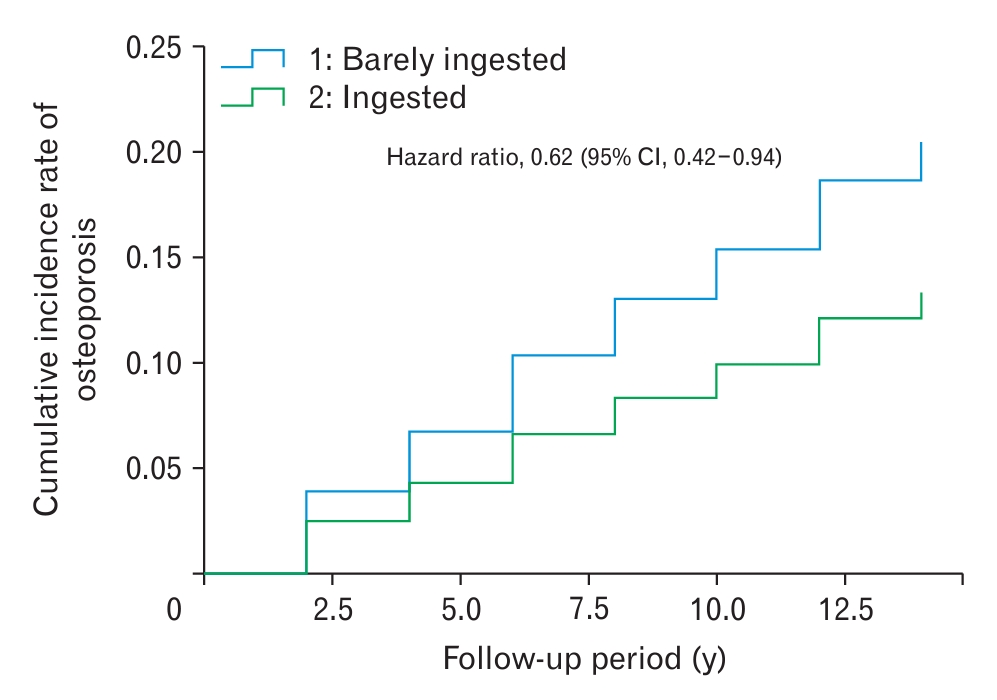
During the follow-up period, the incidence was calculated every other year. During the 16-year follow-up period, 236 of 1,260 participants were newly diagnosed with osteoporosis, representing an incidence of 18.7%. The mean follow-up duration was 8.8 years. The incidence of osteoporosis diagnosis at each calculation ranged from 3.16 to 5.93. In the barely intake group, the average incidence of osteoporosis diagnosis every other year was 4.94. The average incidence in the ingested group was 2.32 (Table 2). The cumulative incidence of osteoporosis was higher in the barely ingested group compared to the ingested group during the follow-up period (Figure 1).
Compared to the referent barely ingested group, the HR (95% CI) for incident osteoporosis of the ingested group was 0.56 (0.375ŌĆō0.836). After adjusting for confounding variables including sex, age, Ca intake, protein intake, muscle mass, physical activity, BMD, smoking, total calorie intake, and coffee intake, the adjusted HR (95% CI) for osteoporosis of the ingested group was 0.62 (0.42ŌĆō0.94) (Table 3).
DISCUSSION
In this large prospective cohort study with a 16-year follow-up period, we found a correlation between processed meat intake and osteoporosis. There was a reduction in the risk of osteoporosis in the high ingested group compared with the barely ingested group. This result was the same after adjusting for confounding variables, and is consistent with other studies that have investigated the relationship between meat intake and osteoporosis. In these studies, the high meat intake groups showed a lower incidence of osteoporosis [15].
Processed meat refers to meat that has been modified through salting, smoking, fermentation, curing or other processes to enhance or preserve its taste for a long time [16]: Many studies have suggested that processed meat contains excessive amounts of salt, saturated fatty acids, and cholesterol, thereby increasing the risk of colorectal cancer and cardiovascular diseases; therefore, it is generally recommended that people refrain from consuming large amount of such food items [9]. However, most Koreans do not consume more than 50 g per day, a quantity known to increase the incidence of cancer [16], and processed meat also contains protein; therefore, this study aimed to focus on the relationship between the protein in processed meat and osteoporosis. The consumption of processed meat continues to increase worldwide, and this pattern is mirrored in Korea. According to a recent report, the average daily intake of red and processed meat in Korean populations was 79.8 g in 2016; and that of processed meat was 9.5 g/d in 2014, 9.8 g/d in 2015, and 10.3 g/d in 2016 [17]. This was lower than the average global daily consumption of processed meat [16], but implies that processed meat can be considered one of the means of protein intake in Korea.
Notably, intake of animal protein and meat have considerable effects on bone health and osteoporosis, but the consequences of consuming animal protein and certain types of meat are still controversial. In contrast to our study, other studies have shown that there is a positive correlation between processed meat intake and the incidence of osteoporosis. Domestic and foreign studies investigating the relationship between Western diet, which includes processed meat, and osteoporosis showed that the incidence of osteoporosis was high in the Western diet group [18,19]. However, this study was the first cohort study to examine the association between osteoporosis and processed meat as a single factor rather than as part of the diet.
This study has several limitations. Firstly, since we only assessed the daily protein intake of the participants, no information regarding the type of protein they consumed could be obtained. Secondly, the diagnosis of osteoporosis and information regarding processed meat intake were self-reported including with the SQFFQ by the participants and thus prone to reporting bias. Food frequency questionnaire is a common dietary assessment method used in prospective cohort studies, but is challenging for individuals to accurately report their food intake over long periods of time [20]. Thirdly, the variability in intake within the processed meat intake group was large, which may have compromised our ability to accurately investigate the effects of intake. Additionally, there were a lack of follow-up data from the KoGES concerning nutrient intake; only the baseline processed meat intake was used in this study. Finally, since our study collected data from participants within a specific region of a single country, our findings may not be applicable to other races, ethnicities, and countries. Despite these limitations, this is the first study to investigate the relationship between processed meat intake and incident osteoporosis in adults using data from a large-scale and long-term prospective cohort study in Korea.
In conclusion, processed meat intake in adults aged 50 years and older was associated with osteoporosis in an inverse and independent manner. This finding suggests that processed meat intake can be proposed as an additional strategy to prevent osteoporosis. Further studies are needed to clarify how processed meat interacts with minerals involved in bone metabolism such as vitamin D and calcium. Furthermore, prospective studies of the relationship between osteoporosis and processed meat in participants from more diverse populations are required.