INTRODUCTION
Risks of smoking have been identified in multiple landmark studies,1,2) and it is the most important modifiable risk factor in mortality rates. According to the Korea National Health and Nutrition Examination Survey (Ministry of Health and Welfare, 2007), 45.0% of Korean men were smokers. Despite a continuous decrease in the prevalence of smokers since the 1980's, South Korea remains in the top 20 of smoking populations worldwide (The Tobacco Atlas 3rd edition).
A quarter of smokers are affected by chronic obstructive pulmonary disease (COPD),3) which is diagnosed about 20 years after the onset of disease.4) To prevent irreversible changes in the lungs, it is important to diagnose COPD early and to help smokers to quit.5) Interventions include individual or group counseling, and pharmacological therapies. Another possible strategy for increasing cessation rates is to provide feedback on the physical effects of smoking by physiological measurements. Several studies have examined the effect of biomarkers, such as impaired lung function, carbon monoxide, atherosclerotic plaque, and CYP2D6 genotype lung cancer susceptibility, on smoking cessation rate, but there is a lack of evidence on the effects of biomarkers for risk assessment.2)
To counsel the results of pulmonary function tests to patients, the concept of 'lung age' was introduced by Morris and Temple5) in 1985. Lung age is estimated from regression equations for the forced expiratory volume in one second (FEV1) in healthy never-smokers,5-7) (Table 1) and constitutes the age at which the FEV1 measured in an individual equals the predicted value of FEV1, taking into account age, height, sex, and ethnicity.8) This concept has received international attention, and has been used to warn individuals against the pulmonary impairment caused by smoking.6) In the randomized controlled trial by Parkes et al.,8) informing smokers of individual lung age significantly improved the likelihood of smoking cessation, when compared to informing FEV1, although this effect was unrelated with the severity of decreased FEV1. A qualitative study among COPD patients examined the results of providing patients with their lung age at the point of diagnosis in hopes of promoting behavioral change.9) The Japanese Respiratory Society recommends the use of lung age in the risk management of COPD.6) Screening of lung disease with lung age was useful,10) and various indicators of obesity may also be related with lung age.6)
Interpretation of spirometry results in terms of 'lung age' had a significant effect in a meta-analysis.2) Lung age is frequently used to promote smoking cessation in other nations, but has not thoroughly been examined in Korea. Thus, we investigated the association between lung age and smoking status in Korean men, using lung age calculated from the predicted FEV1 of Koreans.11) The relationships were also evaluated between lung age and other factors known to affect lung function.
METHODS
1. Study Population
This was a cross-sectional retrospective review of the period between January 2008 and June 2009 (The study was conducted after June 2009). The target population was males aged 20 years or older who visited the health promotion center at Ewha Womans University Hospital. Subjects were eligible if they received a pulmonary function test, chest radiograph, body composition measurements, and anthropometric measurements including height, weight, and waist circumference. A self-administered questionnaire was distributed, and completed questionnaires were returned during a clinical visit. We obtained baseline data regarding age, smoking history in pack years (average daily number of cigarettes smoked divided by 20 and multiplied by the number of years of smoking), medical history, medication, exercise frequency and duration, and comorbidity including chronic bronchitis or emphysema, asthma, pulmonary fibrosis, or other lung disease. Subjects were also interviewed to determine the presence of pulmonary diseases or acute respiratory symptoms. We excluded those who were taking respiratory medications, or those with a history of respiratory disease, cardiovascular disease such as angina or myocardial infarction, neck or thoracic operations, congenital anomaly, malignancy, or neuromuscular disease. None of the men included in this study had abnormal chest radiograph. The study was approved by the institutional review board of Ewha Womans University Hospital (IRB ECT-232-1-32).
2. Pulmonary Function Tests
Patients underwent standard spirometry (Vmax series 2130; Sensor Medics, Yorba Linda, CA, USA) according to the recommendations presented in the Guidelines of the American Thoracic Society. This was repeated at least three times, and the highest reading was used for analysis. The machines were calibrated every morning during the study period with the use of a standard syringe. Values were corrected for body temperature, pressure, and saturation with water vapor.
3. Equations to Predict Lung Age in Korean Males
The population from which the subjects are drawn should be similar with respect to age, height, sex, and ethnic composition to the population from which the prediction values were derived.12) In this manner, equations to predict lung age was derived from "normal predictive values of spirometry in the Korean population" published in 2005. Among 3 predictive equations of spirometry in men, the most predictive equation, including age and height5-7) like other lung age studies, was selected (Table 1).
4. Anthropometry & Body Composition
With the subjects wearing light indoor clothes and no shoes after fasting for more than 8 hours, weight was measured (in kg) on digital weight scales which measured to the nearest 100 g. Height was measured (in cm) by stadiometer to the nearest 0.1 cm while participants stood, wearing no shoes, on a hard surface. Waist circumference was measured (in cm) horizontally through the narrowest part of the torso, between the lowest rib and the iliac crest. Measurements were averaged between measurements separately obtained by two examiners. Total body fat, total muscle mass, percentage body fat, and percentage body muscle were measured with a bioelectrical impedance analysis device (Inbody 3.0; Biospace, Seoul, Korea).
5. Smoking Status
Current cigarette smokers were defined as participants who currently smoke cigarettes daily and who had smoked ≥ 5 packs of cigarettes before the date of spirometer. Ex-smokers were defined as participants who do not currently smoke cigarettes and who had smoked ≥ 5 packs of cigarettes before the date of spirometer. Non-smokers were defined as participants who had smoked < 5 packs of cigarettes during their lifetime or participants who had not smoked at all in the past.13)
6. Statistical Analysis
We used analysis of variance with a Tukey post hoc analysis to analyze differences between smoking groups for normally distributed variables. The Kruskal-Wallis test was used for other types of variables. The dependent variable was age difference (lung age - chronologic age) and univariate linear regression analysis was used to test the effects of independent variables on age difference. Variables with a P-value ≤ 0.10 in the univariate linear regression analysis or variables known to affect lung age were considered as candidates in the final multivariate model. Stepwise multiple linear regression analysis was used to select variables to be maintained in the final model. A P-value of less than 0.05 was considered statistically significant. Statistical analyses were performed using the PASW SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Baseline Characteristics of the Patients
In total, 1,100 adult subjects were enrolled in the study. Baseline characteristics by smoking status are shown in Table 2. Of the subjects, 41.8% were current smokers, 20.7% were exsmokers, and 37.5% were never smokers. Lifetime pack year was higher for current smokers than for ex-smokers (15 vs. 12.5, P < 0.001). FEV1 of non-smokers was higher than that of ex-smokers or current smokers (P < 0.001; 106.0% [3.75 ± 0.56 L], 104.9% [3.64 ± 0.5 L], and 102.8% [3.69 ± 0.53 L], respectively). The exsmoker group was older, had the longest exercise time per week, largest waist and weight, but non-smokers and current smoker groups did not show any difference in these variables. There were no differences in height, body mass index (BMI), muscle mass (%), or fat mass (%) among the 3 groups.
2. Age Difference according to Smoking Status, Indices of Obesity
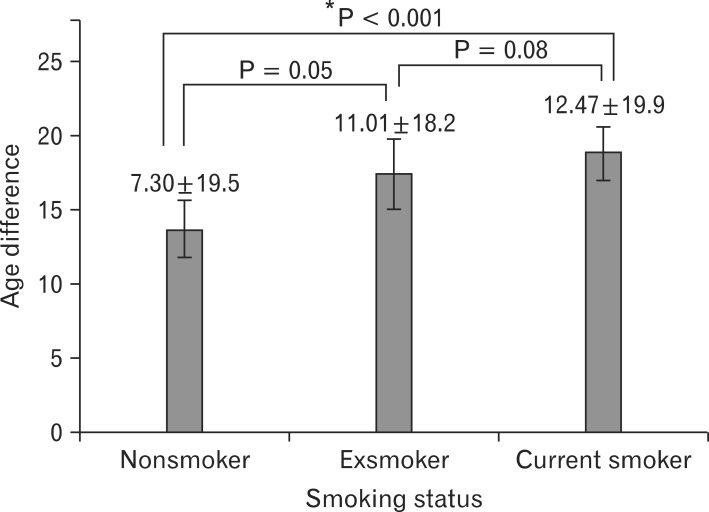
We used age difference (lung age - chronological age) for comparison of lung age due to the higher chronological age in the ex-smokers group (Table 3). There was a trend toward increasing age difference in the order of non-smoker, ex-smoker, and current smoker (P < 0.001; 7.30 ± 19.52, 11.01 ± 18.23, and 12.47 ± 19.90, respectively). The age difference was significant between current smokers and non-smokers (P < 0.001), but not between ex-smokers and non-smokers (P = 0.05), or between ex-smokers and current smokers (P = 0.08) in post hoc analysis (Figure 1).
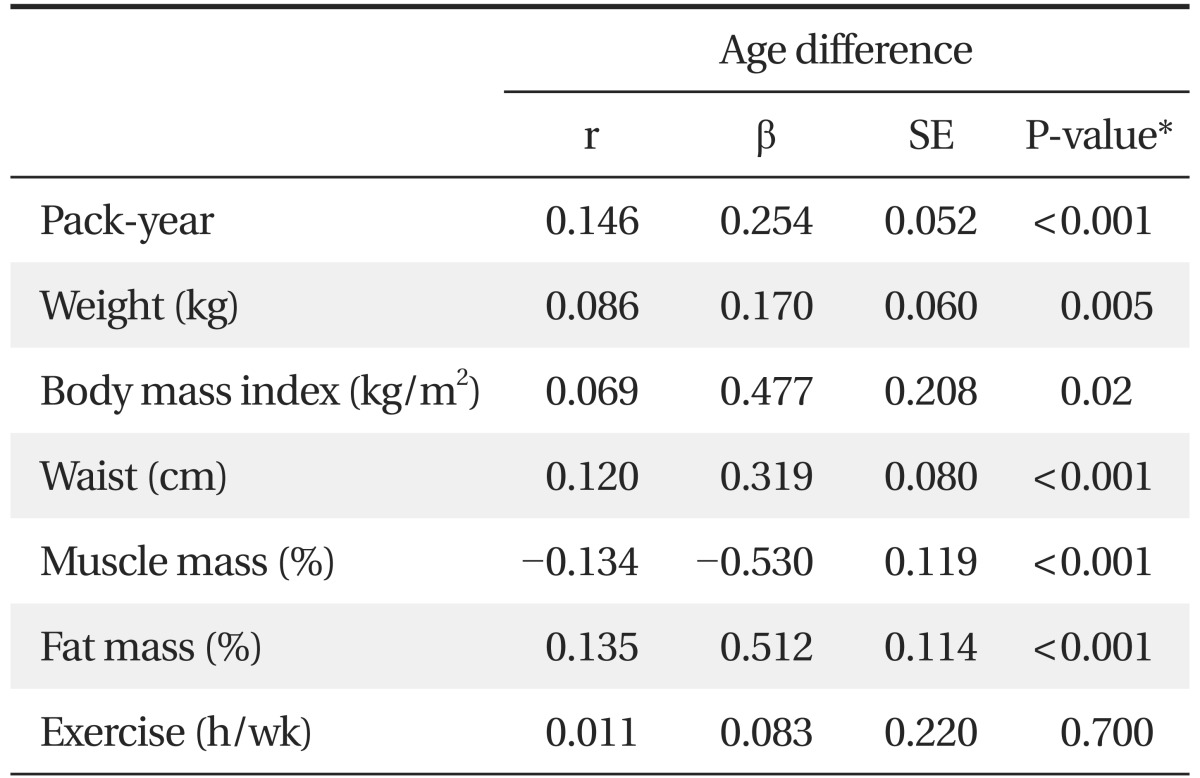
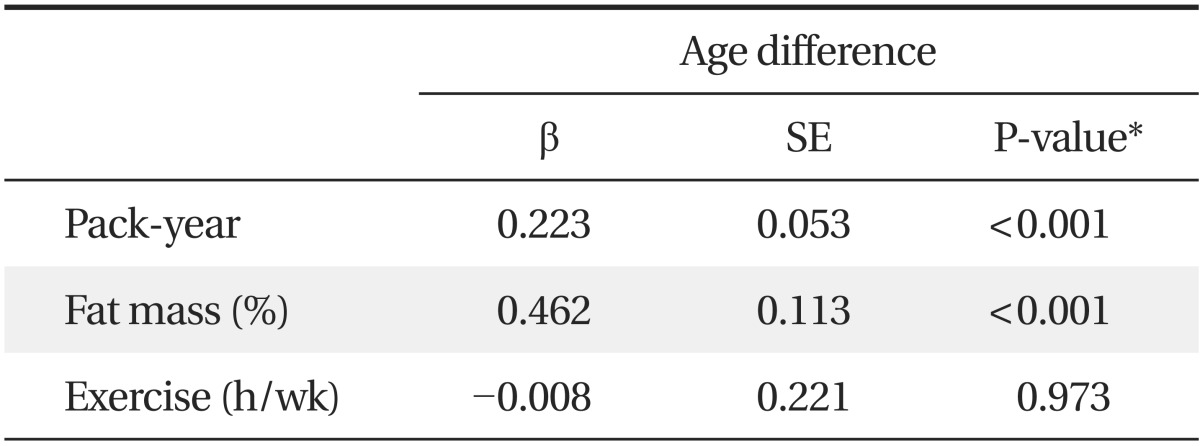
Age difference was associated with life-time pack-year, and (β = 0.254; P < 0.001), weight (β = 0.17; P = 0.005), BMI (β = 0.477; P = 0.02), waist (β = 0.319; P < 0.001), and fat mass (β = 0.512; P < 0.001) showed a positive relationship. Additionally, muscle mass (β = -0.530; P < 0.001) was negatively correlated with age difference (Table 4). Among statistically significant variables in univariate regression analysis such as weight, BMI, fat mass, and muscle mass, only fat mass was included in the multivariate analysis, because the variables showed definite multicollinearity, and the correlation coefficient was greatest for fat mass. When multivariate regression analysis was performed, adjusting for age which can affect lung age, life-time pack year (β = 0.223; P < 0.001) and fat mass (β = 0.462; P < 0.001) was positively correlated with age difference, but exercise was not (β = -0.008; P = 0.973) (Table 5). Life-time smoking of 4.48 pack-year and fat mass of 2.16% was estimated to contribute an additional gain of l year for lung age, respectively.
DISCUSSION
Our data show that the lung age differed significantly between current smokers and non-smokes and that lifelong total amount of smoking was positively associated with lung age, even after adjusting for other factors known to influence lung age. In our study, there was a trend toward decreased age difference in the order of current, ex-, and non-smoker. These findings are similar to those of the study by Wada,14) who assessed the differences in the lung age among smokes, past smokers, and non-smokers in Japan, and to those of another study from Austrailia.7) Dockery et al.15) also reported that FEV1 decreased by 7.4 mL per 1 pack-year increase in lifetime pack-year for male smokers, which translated to a lung age decrease of 1 year per 3 pack-year increase. Although this is somewhat different from our result of 4.48 pack-years, the results were consistent with previous papers which described an inverse association of cigarette smoking with FEV1.16-18)
We confirmed again the correlation of lung age with the indices of obesity known to influence lung function.19-23) Age difference was positively related with fat mass (β = 0.512; P < 0.001), waist circumference (β = 0.319; P < 0.001), and BMI (β = 0.477; P = 0.02) and negatively with muscle mass (β = -0.530; P < 0.001). In multivariate regression models substituting muscle mass or waist circumference for body fat mass, each variable demonstrated a significant association with lung age. Lung age increased 1 year for each 2.08% decrease in muscle mass (β = -0.481; P < 0.001) and 3.7 cm increase in waist circumference (β = 0.270; P = 0.001) (Table not shown). The negative relationship of lung age with muscle mass was pronounced after adjusting for other variables, corresponding with the correlation of FEV1 with fat free mass representative of muscle mass.19,23) In a multivariate regression model including BMI, however, there was weaker correlation of lung age with BMI than other obesity-related indices (β = 0.409; P = 0.049). This finding is in concordance with previous publications' assertion that BMI is not an ideal measure for excess body weight as a predictor of pulmonary function compared with waist circumference or fat-free mass, because a high BMI value can result from higher muscle mass.19,23) Therefore, our results might provide an effective tool to explain the association of lung age with body fat mass, muscle mass, and waist circumference and to presumably control obesity in non-smokers.
Currently, a widely used spirometric reference equation in Korea is based on the Morris equation published in 1979 for Caucasian populations. In this study, the normative predictive values of spirometry in the Korean population published in 2005 by Choi et al.11) was used to derive predictive equation of lung age. We compared the Morris equation and the Choi equation prior to analysis. In the Morris equation, lung age was less than chronological age and was not significantly different with chronological age in current smokers. This result seems paradoxical in suggesting that smokers' lung age is younger than expected, unlike the results reported by Newbury et al.7) In contrast, when the Choi equation was used, lung age was significantly greater than chronological age in smokers (P < 0.001). The Choi equation was derived from a younger Korean population than our study population, and the index study barely included any elderly subjects. For this reason, predictive values of spirometry were greater than that of previous results, over-predicting lung age, even in non-smokers. Future research should be planned to reduce the gap between lung age and chronological age in never smokers.24) If a large-scale study similar to Hansen's study24) was conducted for the Korean population, a more powerful model could be developed.
Our study has several strengths. First, this is the first Korean lung age study and it can provide the basis for research about lung age in this population.2,6-8) Second, we compared currently used predictive equations of spirometry with Choi's predictive values of spirometry in the Korean population, and evaluated the association of lung age with smoking using a more suitable equation. Third, a large number of subjects were selected according to strict criteria by standardized measurement and history.
Limitations of this study include the possible inaccuracy of a self-administered questionnaire and recall bias. However, we tried to obtain more accurate information through history taking by physician for past medical history and current symptoms in the same day. The lack of information on exposure to occupational risk factors and secondhand smoking in non-smokers could be another limitation. Large standard deviations in lung age in each group can be problematic when predicting values for an individual as result of wide variability of spirometry results of normal healthy subjects (Table 3). Moreover, because this study was conducted retrospectively in a health promotion center at a single tertiary referral hospital, the findings are not generalizable to the broader population, and further randomized controlled trials are required to confirm clinical implications.
In conclusion, we found a significant relationship between lung age and both smoking status and fat mass in healthy Korean males. Further research is needed to fully explore the usefulness of lung age in the Korean population.