INTRODUCTION
According to the World Health Organization, the global prevalence of obesity doubled from 1980 to 2014, and the prevalence of childhood obesity also increased owing to improved living standards and a greater preference for the Westernized diet.1) An increasing childhood obesity rate has become a global trend and is emerging as a serious public health issue.2) In South Korea, the prevalence of childhood obesity increased from 14.3% in 2010 to 15.3% in 2013.3)
Childhood obesity confers a burden on society by engendering chronic physical diseases and psychosocial problems.4,5,6) According to data from the Korea Institute for Health and Social Affairs, the annual socioeconomic cost of childhood obesity has reached approximately 1.3638 trillion won.7) In addition, 80% of obese children become obese adults, which increases their risk of chronic diseases and complications in adulthood, thereby increasing the burden of medical costs in subsequent generations.8,9) Therefore, effective management of childhood obesity will help to reduce the socioeconomic burden arising from obesity.
Although a diverse range of school- and community-based intervention programs is being implemented to prevent and manage childhood obesity in Korea,10,11,12,13,14) well-designed, evidence-based intervention trials are scarce. Most Korean intervention trials for prevention of childhood obesity were small-scale and short-term, without significant effects, and targeted only obese children rather than the entire child population.11,12,13) In addition, the assessment methods used in the interventions or contents thereof were rarely evidence based, with most of them being selected and used arbitrarily by the researchers.10,14) Nationwide, non-profit support is needed to boost prevention research. Most of the national research funding for obesity prevention has been short-term and insufficient for a specific purpose. This might be the main reason for the lack of prevention program trials in Korea.
METHODS
1. Selection of the Panel
The panel selection was decided by the research team and confirmed by consultation. The inclusion criteria were as follow: First, a broad range of experts were selected among clinicians, nurses, clinical nutritionists, and researchers in preventive medicine, nutrition, exercise, school health, or policies on childhood obesity prevention. Second, the expert should practice or be involved in a research project for childhood obesity prevention as a person in charge for >1 year. Third, the panel should consist of experts who represent a broad range of expertise and perspectives as related to the childhood obesity prevention program. The final members of the panel were 10 experts who consented to participate in the study.
2. Questionnaire Survey
We selected the final issues for discussion after reviewing domestic and international literatures on childhood obesity interventions, brainstorming within the research group, and discussing the matter with specialists in childhood obesity.17,18,19,20) This corresponds to a modified Delphi technique, as the traditional Delphi technique uses an open-type questionnaire.
A questionnaire was developed to assess the priority population, and the adequacy and feasibility of various items necessary for designing the research on childhood obesity prevention. The questionnaire consisted of five assessment areas, which were ŌĆ£priority populations,ŌĆØ ŌĆ£methods of intervention,ŌĆØ ŌĆ£settings of intervention,ŌĆØ ŌĆ£measurement of outcomes,ŌĆØ and ŌĆ£duration of intervention.ŌĆØ For the questions about the priority population of the intervention, the panel members rated the value of addressing each item from 1ŌĆō5, where 1 is the highest value (score of 5) and 5 is the lowest value (score of 1). The scores for each of the questions were summed to compute the score for the level of importance. The survey also contained questions that addressed the adequacy of 3 representative intervention methods, and the anticipated effect size and feasibility of 4 intervention settings. In addition, the panelists were asked to evaluate the adequacy and feasibility of key variables for assessing intervention outcomes, including 7 anthropometric indexes, 5 clinical indexes, and 6 intermediate variables. Finally, the survey included questions about whether 5 potential intervention durations would be appropriate for assessing the intervention effects. A 5-point scale was applied to each assessment question, with scores of 1 or 2 defined as negative; 3, as having reservations; and 4 or 5 as affirmative. Prior to the commencement of the survey, the questionnaire was corrected and supplemented through the advice of an external expert who had extensive experience with the Delphi technique.
At the time of the drafting of the research background and questionnaire, e-mails were sent, in which the precautions to be taken by the subjects were delineated, including ŌĆ£prohibition of mutual exchange of opinionsŌĆØ and ŌĆ£self-administered questionnaire.ŌĆØ The e-mails also contained the questionnaires, guidelines, and number of questionnaire surveys to be conducted. Ten days were spent for the distribution and retrieval of the first and second questionnaires, and 1 day was spent for the development of the second questionnaire.
3. Analysis of the Results
The panelists' opinions were gathered from the second questionnaire survey, and the stability of the survey was evaluated. When the interquartile range (IQR) was <1 and the coefficient of variation (CV) was less than 0.5, the survey was evaluated as stable. In addition, a portfolio analysis was performed, with the adequacy and feasibility indexes as the two axes. If more than two-thirds of the respondents submitted a ŌĆ£negativeŌĆØ (1 or 2 points), ŌĆ£having reservationsŌĆØ (3 points), or ŌĆ£affirmativeŌĆØ evaluation (4 or 5 points) for any one of the items, it was defined that consensus was reached on the corresponding question.21,22,23) If an item belonged to quartile I of the portfolio, it was denoted as having high adequacy and feasibility. However, if an item belonged to quartile III, it was denoted as having low adequacy and feasibility. MedCalc ver. 11.4 (MedCalc Software, Mariakerke, Belgium) was used for the statistical analysis.
RESULTS
1. General Characteristics of the Panel
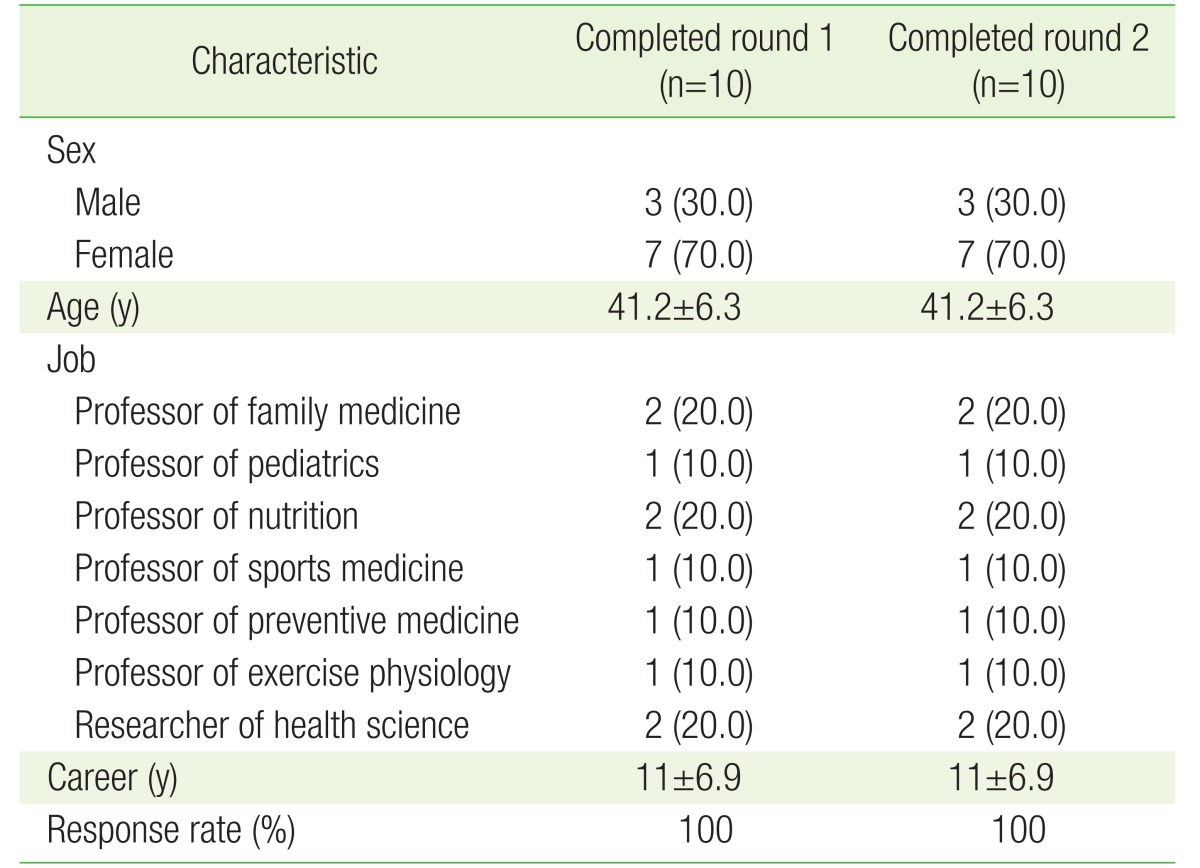
The participating panel in the survey was composed of 10 members (3 men and 7 women), with a mean age of 41.2┬▒6.3 years. By occupation, the panel included 2 professors of family medicine, 1 professor of pediatrics and adolescent medicine, 2 professors of nutritional science, 1 professor of sports medicine, 1 professor of preventive medicine, 1 professor of sports physiology, and 2 health science researchers. The mean length of professional experience in their respective areas was 11┬▒6.9 years. The response rates for both the first and second surveys were 100.0% (Table 1).
2. Assessment of the Priority Population for Future Research
The priority age groups to be considered at the time of designing the research on childhood obesity prevention were, in order of decreasing importance, ŌĆ£lower elementary school gradesŌĆØ (46 points), ŌĆ£higher elementary school gradesŌĆØ (43 points), ŌĆ£preschoolŌĆØ (26 points), ŌĆ£middle schoolŌĆØ (24 points), and ŌĆ£high schoolŌĆØ (11 points).
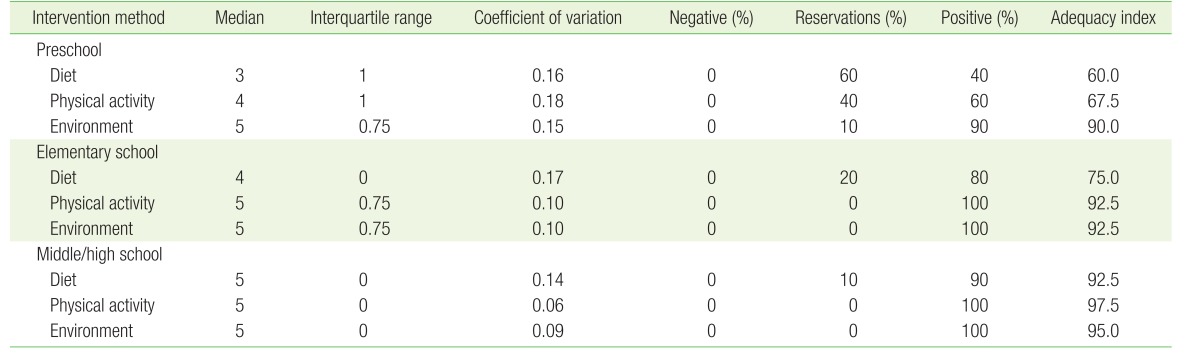
3. Assessment of Intervention Methods for Future Research
The intervention methods that received an ŌĆ£affirmativeŌĆØ (4 or 5 points) consensus for their adequacy, according to age group, were ŌĆ£environmental controlŌĆØ for preschool children, and ŌĆ£dietary control,ŌĆØ ŌĆ£physical activity control,ŌĆØ and ŌĆ£environmental controlŌĆØ for elementary, middle, and high school students. Thus, an affirmative consensus was reached for 77.8% (7/9) of the items. Meanwhile, for preschool children, ŌĆ£dietary controlŌĆØ received a ŌĆ£having reservationsŌĆØ evaluation from 6 of the 10 panelists; and ŌĆ£physical activity controlŌĆØ received an ŌĆ£affirmativeŌĆØ evaluation from 6 of the 10 panelists. The IQR was 0ŌĆō1, and the CVs ranged from 0.06 to 0.18, indicating that the survey was stable (Table 2).
4. Assessment of Intervention Settings for Future Research
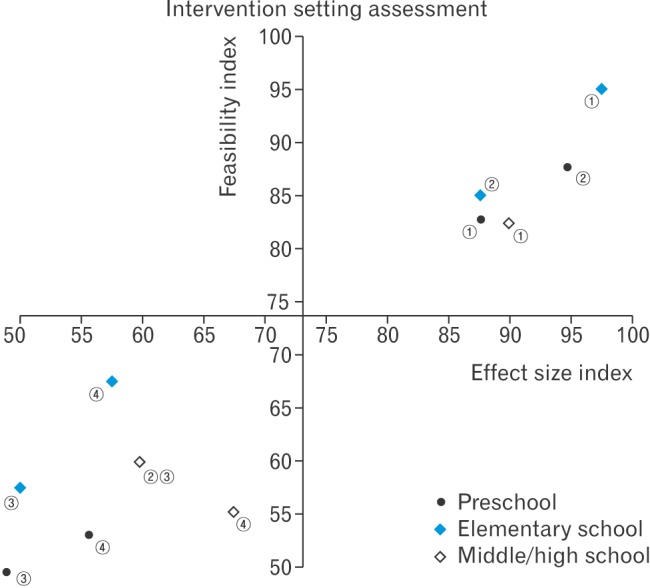
The intervention settings that received an affirmative consensus in terms of the anticipated effect size and feasibility for preschoolers were ŌĆ£homeŌĆØ and ŌĆ£kindergarten and childcare centers,ŌĆØ while ŌĆ£communityŌĆØ received a consensus of ŌĆ£having reservations.ŌĆØ The IQR was 0ŌĆō1, and the CVs ranged from 0.06 to 0.28, indicating that the survey was stable. A consensus was reached for 83.3% of the items pertaining to the intervention setting (20/24) (Table 3).
In the portfolio analysis, ŌĆ£homeŌĆØ and ŌĆ£kindergarten and childcare centersŌĆØ were the settings evaluated to have high effect sizes and feasibility (quartile I) for preschoolers. On the other hand, ŌĆ£primary careŌĆØ and ŌĆ£communityŌĆØ settings were evaluated to have low effect sizes and feasibility (quartile III) for this age group. For elementary school students, ŌĆ£schoolŌĆØ and ŌĆ£homeŌĆØ were evaluated as having high effect sizes and feasibility, while ŌĆ£primary careŌĆØ and ŌĆ£communityŌĆØ were evaluated as having low effect sizes and feasibility. In the case of high school students, ŌĆ£schoolŌĆØ was assessed as having a high effect size and feasibility, while ŌĆ£home,ŌĆØ ŌĆ£primary care,ŌĆØ and ŌĆ£communityŌĆØ were assessed as having low effect sizes and feasibility (Figure 1).
5. Assessment of Intervention Outcomes for Future Research
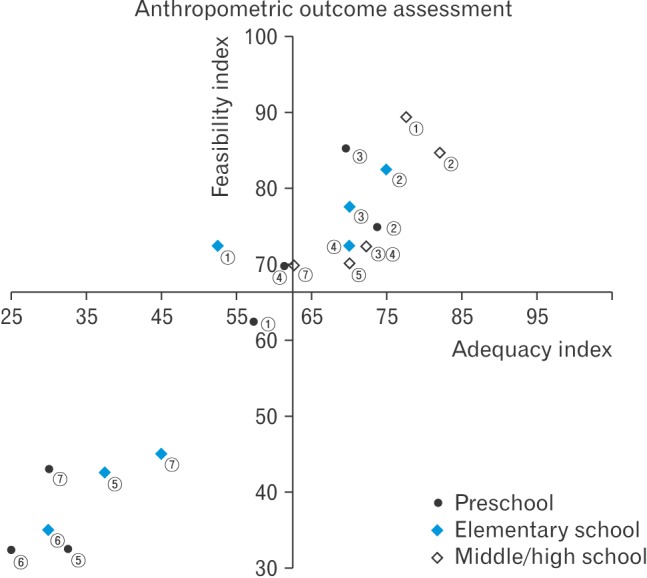
The panelists were also asked to evaluate key outcome measures of obesity interventions, including anthropometric indexes such as ŌĆ£body mass index (BMI),ŌĆØ ŌĆ£BMI percentile,ŌĆØ ŌĆ£relative weight on the standard weight for each sex and age group,ŌĆØ ŌĆ£prevalence of obesity in the group,ŌĆØ ŌĆ£waist circumference,ŌĆØ ŌĆ£skin thickness,ŌĆØ and ŌĆ£body fat.ŌĆØ In the portfolio analysis, ŌĆ£BMI percentileŌĆØ was deemed as having high adequacy and feasibility for preschoolers. In the case of the elementary school students, ŌĆ£BMI percentile,ŌĆØ ŌĆ£relative weight on the standard weight for each sex and age group,ŌĆØ and ŌĆ£prevalence of obesity in the groupŌĆØ were the indexes with high adequacy and feasibility. For the middle and high school students, the indexes evaluated as having high adequacy and feasibility included ŌĆ£BMI,ŌĆØ ŌĆ£BMI percentile,ŌĆØ ŌĆ£relative weight on the standard weight for each sex and age group,ŌĆØ ŌĆ£prevalence of obesity of the group,ŌĆØ and ŌĆ£waist circumferenceŌĆØ (Figure 2).
In the portfolio analysis of clinical indexes such as ŌĆ£blood pressure,ŌĆØ ŌĆ£serum glucose level,ŌĆØ ŌĆ£cholesterol,ŌĆØ ŌĆ£liver function,ŌĆØ and ŌĆ£proteinuria,ŌĆØ all the indexes were assessed as having low adequacy and feasibility for both preschoolers and elementary school students. For the middle and high school students, ŌĆ£blood pressure,ŌĆØ ŌĆ£serum glucose level,ŌĆØ and ŌĆ£cholesterolŌĆØ were the indexes scored with high levels of adequacy and feasibility (Figure 3).
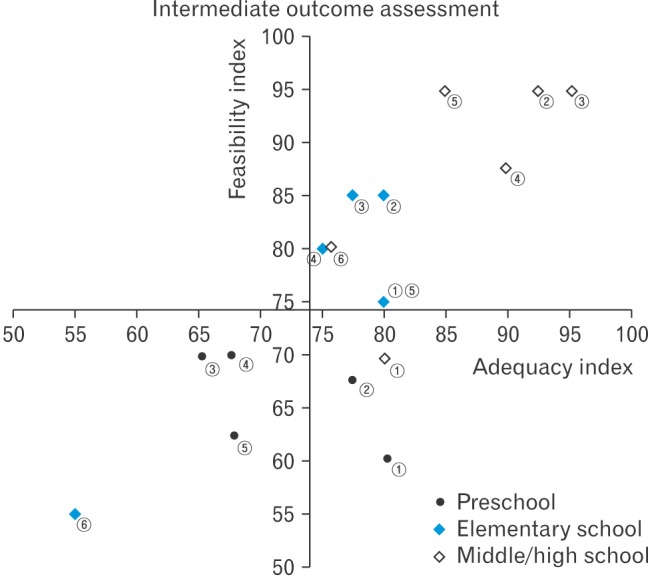
In the portfolio analysis for the measurement of intermediate variables, including ŌĆ£knowledge of, attitudes toward, and beliefs about nutrition,ŌĆØ ŌĆ£eating-related behavior,ŌĆØ ŌĆ£quantity of food eaten,ŌĆØ ŌĆ£screen time,ŌĆØ ŌĆ£amount and intensity of exercise,ŌĆØ and ŌĆ£emotions such as depression and sense of self-efficacy,ŌĆØ the indexes assessed as having high adequacy but low feasibility were ŌĆ£knowledge of, attitudes toward, and beliefs about nutrition,ŌĆØ and ŌĆ£eating-related behaviorŌĆØ for preschoolers. For elementary school students, all the indexes except ŌĆ£emotions such as depression and sense of self-efficacyŌĆØ were scored as having high adequacy and feasibility. In the case of middle and high school students, all the intermediate variables except ŌĆ£knowledge of, attitudes toward, and beliefs about nutritionŌĆØ were evaluated as having high adequacy and feasibility (Figure 4).
6. Assessment of Intervention Durations for Future Research
The periods deemed appropriate for the assessment of the intervention outcomes were 9 months for the ŌĆ£anthropometric indexesŌĆØ (mean┬▒standard deviation score: 2.5┬▒0.53), 1 year for the ŌĆ£clinical indexesŌĆØ (2.9┬▒0.32), and 6 months for the ŌĆ£intermediate variablesŌĆØ (2.1┬▒0.32). The IQR was 0ŌĆō1, and the CVs ranged from 0.11 to 0.21, indicating that the survey was stable.
DISCUSSION
In this study, a Delphi survey was conducted to examine the priority age group for the research on childhood obesity prevention, and the adequacy and feasibility of different intervention methods. It is significant that the Delphi technique was applied for the first time in Korea to assess the priorities and intervention methods for a future research on childhood obesity prevention.
Elementary school students were judged as the highest priority population for the research on childhood obesity prevention. For preschoolers, ŌĆ£kindergarten and childcare centersŌĆØ and ŌĆ£homeŌĆØ were selected as the priority settings, and ŌĆ£environmental controlŌĆØ interventions that measure ŌĆ£BMI percentileŌĆØ were found as having high adequacy and feasibility among the various methods and outcome measures. In the case of the elementary school students, the priority settings for future research were established as ŌĆ£schoolŌĆØ and ŌĆ£home,ŌĆØ and high adequacy and feasibility were assigned to interventions focused on ŌĆ£dietary control,ŌĆØ ŌĆ£physical activity control,ŌĆØ and ŌĆ£environmental controlŌĆØ and measuring ŌĆ£BMI percentile,ŌĆØ ŌĆ£relative weight on the standard weight for each sex and age group,ŌĆØ ŌĆ£prevalence of obesity of the group,ŌĆØ ŌĆ£nutritional knowledge, attitudes, and beliefs,ŌĆØ ŌĆ£eating-related behavior,ŌĆØ ŌĆ£quantity of food eaten,ŌĆØ ŌĆ£screen time,ŌĆØ and ŌĆ£amount and intensity of exercise.ŌĆØ For middle and high school students, ŌĆ£schoolŌĆØ was selected as the priority setting, and interventions that focused on ŌĆ£dietary control,ŌĆØ ŌĆ£physical activity control,ŌĆØ and ŌĆ£environmental controlŌĆØ and measured most of the possible indicators were assessed as having high adequacy and feasibility.
The priority age groups of the research on childhood obesity prevention were (in decreasing order) ŌĆ£elementary school,ŌĆØ ŌĆ£preschool,ŌĆØ and ŌĆ£middle and high schoolŌĆØ students. In the results of the questionnaire survey conducted by Wu et al.24) about the prevention of childhood obesity, the priority age group was ŌĆ£preschool students,ŌĆØ followed by ŌĆ£elementary school students.ŌĆØ When anticipating the outcomes of the research on childhood obesity prevention in a domestic environment, the panelists of this study considered elementary school students to be the highest-priority group. This may be because elementary school students do not yet have fixed lifestyles and are at an age when an intervention would be realistic owing to the low burden of their school studies. In addition, elementary school students may be the most effective target population for the prevention of obesity or related diseases.
Regarding the appropriate intervention method(s) for the research on childhood obesity prevention for each age group, ŌĆ£environmental controlŌĆØ was assessed as appropriate for preschoolers, and ŌĆ£environmental control,ŌĆØ ŌĆ£physical activity control,ŌĆØ and ŌĆ£dietary controlŌĆØ were deemed appropriate for elementary, middle, and high school students. In our assessment, this could be because meals and physical activities are dictated by the surrounding environment without the students' selection or control, and because preschoolers lack self-control. In a meta-analysis of 37 obesity intervention trials conducted over a period of 12 weeks in adolescents aged <18 years, BMI was reduced by 0.11 kg/m2 (P=0.02) when only ŌĆ£physical activity controlŌĆØ was applied and by 0.12 kg/m2 (P=0.16) when only ŌĆ£dietary controlŌĆØ was applied. However, when interventions such as ŌĆ£physical activity controlŌĆØ and ŌĆ£dietary controlŌĆØ were combined, BMI was reduced by 0.18 kg/m2 (P<0.0001).25) Considering that the combined intervention was more effective than the respective individual interventions, combined interventions could achieve much better effects among elementary school students, and middle and high school students.
We assessed both, the anticipated effect size and feasibility of different settings for research on childhood obesity prevention for each age group through a portfolio analysis. As we anticipated that high effect sizes and feasibilities could be achieved through interventions at ŌĆ£kindergarten and childcare centersŌĆØ and ŌĆ£homeŌĆØ for preschoolers, ŌĆ£schoolŌĆØ and ŌĆ£homeŌĆØ for elementary school students, and ŌĆ£schoolŌĆØ for middle and high school students, we deemed that these intervention settings should be highly prioritized. On the other hand, the intervention effects and feasibilities were anticipated to be low for the ŌĆ£primary careŌĆØ and ŌĆ£communityŌĆØ settings for preschoolers and elementary school students, and for the ŌĆ£home,ŌĆØ ŌĆ£primary care,ŌĆØ and ŌĆ£communityŌĆØ settings for middle and high school students. Thus, the specific obstacles in these settings should be examined. Primary care settings are thought to be more appropriate for treatment interventions than for preventive interventions. ŌĆ£HomeŌĆØ received a reserved assessment for middle and high school students, likely because the time such students spend at home is short, as most of their time is spent at school or in private academies.
A diverse range of outcome measures have been used in research studies on childhood obesity prevention in Korea. However, systematic comparison of these studies has been difficult because most of the researchers arbitrarily used cross-sectional self-defined outcome measures.26,27,28) Thus, in this study, we identified the most appropriate and feasible indexes among those used previously, in an effort to standardize the tools for measuring outcomes. The number of available measurement tools increased as the age group increased in the case of the anthropometric indexes. In the case of the clinical indexes, all were assigned low adequacy and feasibility for preschoolers and elementary school students, while indexes such as ŌĆ£blood pressure,ŌĆØ ŌĆ£serum glucose level,ŌĆØ and ŌĆ£cholesterolŌĆØ were deemed to have high adequacy and feasibility for use among middle and high school students. Regarding the anthropometric or intermediate indexes that influenced the clinical indexes, ŌĆ£quantity of food eaten,ŌĆØ ŌĆ£screen time,ŌĆØ and ŌĆ£amount and intensity of exerciseŌĆØ cannot be considered as age-appropriate indexes for preschoolers. For elementary school students, the assignment of low adequacy and feasibility to ŌĆ£emotions such as depression and sense of self-efficacyŌĆØ needs to be reassessed.
The durations selected as appropriate for the assessment of outcomes of research on childhood obesity prevention were 9 months, 1 year, and 6 months for the anthropometric indexes, clinical indexes, and intermediate variables, respectively. The results of an evidence-based research review suggested that proper assessment can be made only if school-based interventions are executed for a minimum of 6 months and if community-based interventions are executed for a minimum of 1 year.19,20)
The limitations of this study include the following: First, because a questionnaire with structuralized and closed questions was used for the first survey, the panel members' ability to express their opinions might have been restricted. Second, the results might have been exaggerated or downsized, as weighting was applied during the calculation of the importance scores, adequacy indexes, and feasibility indexes used for the assessment of priorities.
In this study, the priorities for designing the research on childhood obesity prevention were assessed with the Delphi technique, and their adequacies and feasibilities were considered. The highest-priority population for the research on childhood obesity prevention was elementary school students. Different settings, contents, assessment methods, and durations were anticipated to be effective in the different age groups. Accordingly, future research is needed to evaluate intervention outcomes by developing a research on childhood obesity prevention by using appropriate indexes over a prolonged period, with consideration of the populations and settings with high levels of adequacy and feasibility.