INTRODUCTION
Marital status has been an important sociodemographic variable for health studies. Married adults not only appear to have better mental and physical health than their unmarried counterparts,1,2) but also have lower morbidity and mortality.3) Marital status also affects specific health behaviors. Women who were divorced or widowed had an increased risk of relapsing or starting smoking than women who stayed married.4) Divorced or widowed men were more likely to be smokers and less likely to be moderate drinkers than married men.5) Becoming divorced or widowed was associated with decreased vegetable intake in both men and women.4,6)
According to the Korean Population and Housing Census, the proportion of the never married adults increased consistently from 21% in 1980 to 24% in 2010.7) Though the divorce rate in Korea has been decreasing since 2003, still 9.5 couples among 1,000 married couples in Korea divorced in 2010.8) The high divorce rate and the increasing rate of never married adults are not only a social phenomenon but have implications for personal health behavior and health status. However, domestic studies on marital status and health have mainly focused on specific health habits9) or specific regions,10) and are therefore hard to generalize to the broader population. This study is to assess whether marital status is associated with health behavior of Korean middle-aged adults.
METHODS
1. Korean National Health and Nutrition Examination Survey and Study Participants
The Korean National Health and Nutrition Examination Survey (KNHANES) is an annual survey to assess health conditions, health related behaviors, and the nutritional status of Korean people. This study used data from the 2010 KNHANES. Among 10,938 persons who participated in the 2010 KNHANES, we selected 2,522 adults (1,049 men and 1,473 women) aged between 40 and 65 years old, who completed all three components (the Health Interview Survey [HIS], the Nutrition Survey [NS], and the Health Examination Study) of the KNHANES.
2. Variable Measurement
1) Marital status assessment
Data on marital status was obtained through the household survey of the HIS. The marital status question was 'Have you been married?' If participants said 'no', he or she was placed in the never married group. If participants said 'yes', the next question given was, 'What is your marital status?' If participants said 'I am living with my partner', he or she was placed in the living with a partner group. The other answers such as separated, widowed, divorced and never married were regarded as the living without a partner group.
2) Health behavior measurement
Data on health behaviors was obtained through the HIS and the NS. Smoking status, alcohol intake, exercise, and breakfast consumption were assessed by the self-administered questionnaires, and periodic health examinations were evaluated by interviews. Smoking status was classified as smoker and nonsmoker. The question was, 'Do you currently smoke cigarettes?', if the answer was 'smoke daily' or 'sometimes smoke', they were placed in the current smoker group. Non-smoker was defined as ex-smoker or people who had never smoked cigarettes. High-risk alcohol intake was defined as an average of more than 7 glasses (5 glasses for women) on one occasion and more than twice a week for men during the previous one year according to the definition used in KNHANES.
Periodic health screening was assessed by the question 'Have you been screened for your health during the last two years?' If the answer was 'yes', they were considered to have periodic health screening. Participants who practiced any type of physical activity (vigorous, moderate, and walking) were classified as regular exercisers. The regular breakfast consumer was defined as a participant who had breakfast without skipping during the previous two days.
3) Covariates measurement
The participants were categorized by age into 40 to 49 years, 50 to 59 years, and 60 to 65 years groups. Educational level was classified as less than middle school graduate, high school graduate, and more than college graduate. Household equivalent income was calculated by dividing total family income by the square root of the number of family members and categorized into tertiles (high, middle, and low). Occupation was classified into non-manual, manual workers, and the unemployed.
Height was measured to the nearest 0.1 cm on a stadiometer (SECA 225; SECA Deutschland, Hamburg, Germany). Body weight was measured to the nearest 0.1 kg on a balance scale (GL-6000-20; CAS Korea, Seoul, Korea) with the subject wearing a lightweight gown or underwear. Body mass index (BMI) was classified into less than 22.9 kg/m2 (normal), 23.0 to 24.9 kg/m2 (overweight), or over 25.0 kg/m2 (obese) according to the standard of World Health Organization (Asia Pacific regional guideline).11) Chronic diseases including hypertension, diabetes, dyslipidemia, stroke, ischemic heart disease, and cancer (stomach, liver, colon, breast, lung, and cervical cancer) diagnosed by physicians was questioned. If participants said 'yes' to any kinds of chronic disease, he or she was regarded as having the chronic disease.
3. Analysis
Descriptive analyses and bivariate analysis were performed with SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA) to incorporate sampling weight (wt_tot) considering the multistage probability sampling design of KNHANES and non-response. Interaction effect between gender and marital status was assessed by inserting sex*marital status interaction terms into the logistic models. A significant gender by marital status interaction was observed for regular exercise (P = 0.003) and periodic health screening (P = 0.007). Thus, subsequent analyses were conducted for men and women separately.
Logistic regression analyses were performed to examine the relationship between five health behaviors and marital status, after adjustment for age, educational level, income level, occupation, and chronic disease. Odds ratios (OR) and 95% confidence interval (CI) are presented.
The study protocol was reviewed and approved by the institutional review board of the Seoul Paik Hospital (IRB no. IIT 2012-230) and informed consent was waived.
RESULTS
1. General Characteristics
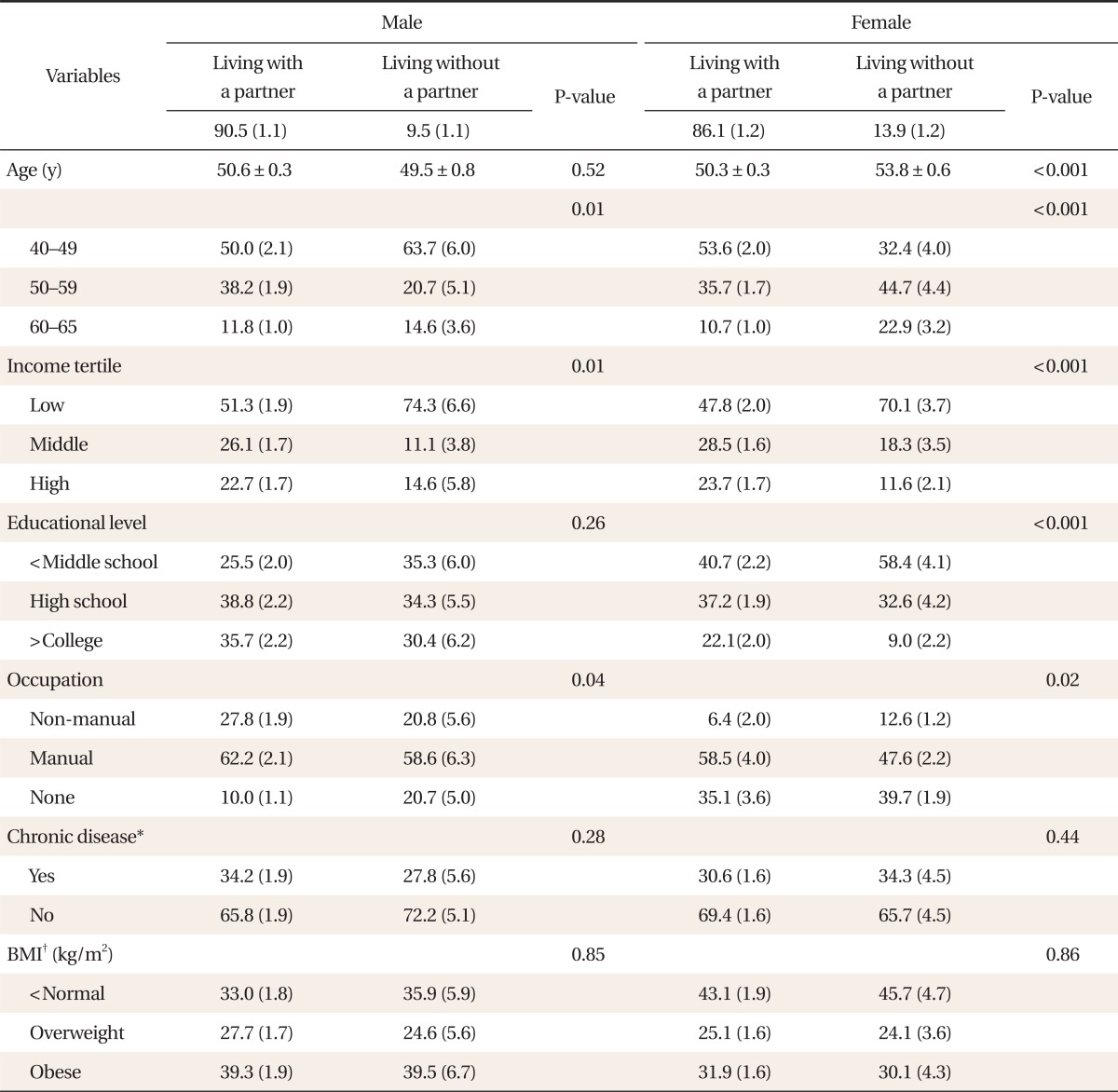
When sampling weights were applied, 1,049 men represented 8,509,866 of Korean middle-aged men. The proportion of men living without a partner was 9.5 (1.1)%. One thousand four hundred and seventy-three women represented 8,336,278 of Korean middle-aged women. The proportion of women living without a partner was 13.9 (1.2)%. General characteristics of the study population were shown in Table 1. Living without a partner group was sub-typed into 'divorced or separated,' 'widowed,' and 'never married.' In men, proportions of each group were 5.0 (0.7)%, 1.0 (0.3)%, and 3.6 (0.8)%, respectively, and were 5.6 (0.7)%, 7.3 (0.8)%, and 0.9 (0.3)% in women (data not shown).
The mean age was not significantly different between men living with a partner and men living without a partner while the proportion of 50-year-olds was lower in the living without a partner group (P = 0.01). Women living without a partner were older (P < 0.001). The living without a partner group was more likely to have low household income (P for men = 0.01, P for women < 0.001), less education (only for women P < 0.001), and more likely to be unemployed (0.04, 0.02, respectively). Chronic disease and BMI were not significantly different by marital status in both male and female groups (Table 1).
2. Health Behavior
1) Cigarette smoking
The unadjusted smoking rate for men living with a partner group was 44.4 (2.0)% and 56.9 (6.4)% for men living without a partner. However, after covariate adjustment, there was no significant difference in smoking rate by marital status (OR, 1.48; 95% CI, 0.88 to 2.50). Women living without a partner (8.6 [2.2]%) were more likely to be smokers (OR, 2.27; 95% CI, 1.09 to 4.73) than their counterparts (4.1 [0.9]%) (Tables 2, 3).
DISCUSSION
Regardless of population subgroup (age, education level, household income, occupation, or chronic disease) married middle-aged Korean adults were generally found to have healthier behaviors than single adults, and the association between marital status and health behavior differed by sex. Among dimensions of health behavior, regular breakfast consumption and periodic health examination were more sensitive to marital status in men as were smoking and high-risk alcohol intake in women.
Living with a partner allows one to have a good-quality diet and provides access to proper medical care.4,12) Eng et al.6) reported that divorced or widowed men eat less vegetables and more instant food. Davis et al.13) also found that single men have a low quality diet when compared to their married counterparts. In a similar vein, our study showed that men living with a partner eat breakfast in a more regular fashion and undergo periodic health examinations more than men without a partner, while women were not influenced by marital status. This may be due to a characteristic typical of Korean culture, in which wives prepare food for their husbands. Hence married men are more likely to eat breakfast.
Some previous studies showed that the health benefits by marriage do not differ by sex,14,15) while most other studies had results similar to ours, showing that men get more benefits than women through marriage.16,17) Some explanations include the fact that that women generally have better health behaviors than men and are more interested in monitoring and intervening on their partners' health behaviors,18) and women give more social support and psychological stability to their partners than men.19)
The effects of marital status on health behaviors in Korean middle-aged adults differed by gender. Smoking rate and the rate of high-risk alcohol intake were higher in women living without a partner than in women living with a partner in our study. Women who experienced divorce, separation, and death of spouse might get distressed by financial burden and the responsibility of rearing children by themselves, which might increase smoking rate.20,21) Release from social control (telling or reminding someone to engage in certain health behaviors) and loss of social support (support when changing health behavior) from partners might increase the smoking rate further.22) Umberson23) reported that social control and social support have beneficial consequence for health behaviors among those individuals who remain married. A similar mechanism might be exercised in the rate of excessive alcohol intake in single women.24,25)
Contrary to expectations, middle-aged Korean men living without a partner did not smoke or drink alcohol significantly more than married men did. The Korean men living without a partner group was a mixture of different subtypes (i.e., widowed, separated, never married, and divorced) who have different health risk behaviors. Western studies reported that divorced men showed a higher smoking rate and heavier alcohol consumption than their married counterparts,5,6,24) while, never married men's health behavior was similar to men living with a partner.2) Therefore, the resultantly null relationship was shown in middle-aged men in our study.
Schone and Weinick26) reported that living with a partner has positive influence on practicing regular exercise. Interestingly, the influence of marital status on regular exercise differed completely between men and women in Korea. Men living without a partner and women living with a partner had a higher rate of practicing regular exercise than their counterparts. The reason might be that most married men in Korea bear the economic responsibility of their families and therefore use their time and energy on working. Even in free time, they tend to use it with their families rather than exercising for themselves.
Two hypotheses may explain why married adults were healthier than unmarried single adults. First, married adults are more likely to be economically stable and get social and psychological supports from their partner. They are more interested in their own heath and the pursuit of a happier life. This interest drives them towards healthier behaviors (marriage protection effects). Joung et al.27) reported that married people were more likely to engage in positive health behaviors and less likely to engage in negative ones than singles because they experience less stress and more social support.
The second hypothesis is that of marriage selection effects, which explain that healthier individuals are more likely to marry and to stay married while less healthy people either do not marry or are more likely to become separated, divorced, or widowed, and the change in marital status causes stress, increases morbidity and mortality, and negatively influences health behaviors.28,29) However, the KNHANES was not designed to evaluate the exact mechanisms connecting marital status and health behaviors. We cannot tell which hypothesis more correctly reflects the relationship between marital status and healthy behavior in Korean adults.
Other limitations are as follows. The KNHANES is a cross-sectional survey and so causality in the marital status and health behaviors cannot be determined. Our results are based on self-reported data. The accuracy of information on health behaviors obtained from self-filled questionnaires and health interviews could be limited. The low prevalence of single adults in middle-aged Koreans in the 2010 KNHANES makes subgroup analysis (divorced or separated, widowed, and unmarried) of the living without a partner group impossible due to low statistical power.
The study had strengths as well. We used a nationally representative sample of Korean adults which increases the external validity of our results. This study is the first to assess the relationship between marital status and health behaviors from a representative sample of Korean adults. We included both men and women to confirm the interaction effects between sex and marital status. Hence we could suggest that the difference in health behaviors might be a possible explanation for the association between marital status and health.26) We hope this study could be a basis to organize health promotion programs especially directed at separated, divorced, widowed, and never married persons to encourage healthier lifestyle.